CHAPTER 94 Temporomandibular Joint Disorders
Anatomy
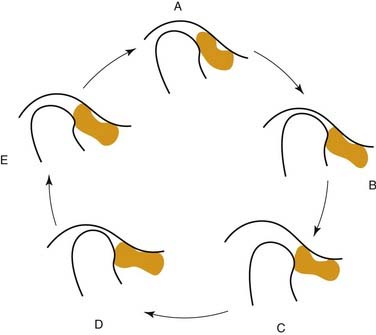
Interposed between the articulating surfaces of the TMJ is the articular disk. The disk is a unique structure that is concavo-convex on its superior surface and concave on its inferior surface, where it contacts the convex condylar head. The presence of the articular disk divides the joint into two distinct compartments and contributes to the dual action of this ginglymoarthrodial joint. The inferior compartment, or inferior joint space, allows for purely anterior and posterior rotational movement between the condyle and disk. The superior joint space allows for translational movement between the disk and the glenoid fossa and articular eminence. In addition to assisting movement within the joint, the disk acts to compensate for any incongruencies between the articular surfaces and acts as a shock absorber within the joint.1
Diseases and Disorders
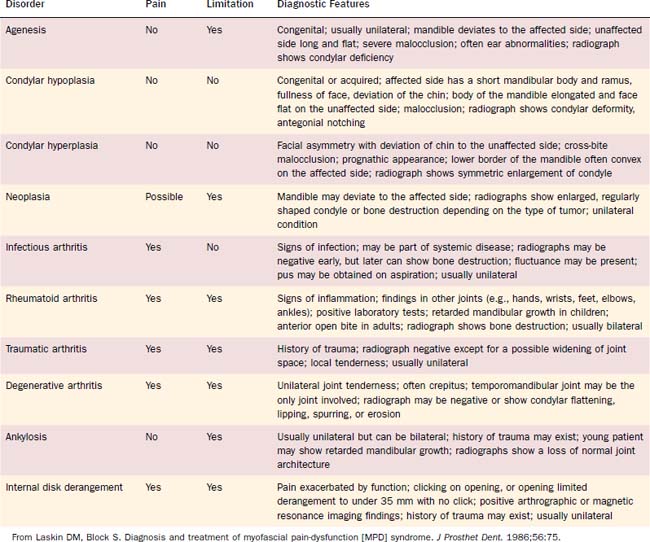
The TMJ is susceptible to the same conditions that affect other joints in the body such as congenital and developmental anomalies, traumatic injuries, dislocations, internal derangements of the articular disk, ankylosis, various arthritic conditions, and, rarely, neoplastic diseases (Table 94-1). Although many of these conditions are treated in the same manner as in other joints, the previously described anatomic and functional differences of the TMJ often require some variations of therapy.
Congenital and Developmental Anomalies
Because the condyle has an important role in mandibular growth, congenital and developmental anomalies such as condylar agenesis, condylar hypoplasia, or condylar hyperplasia can produce severe facial deformity. It is important to diagnose and treat these conditions early in order to limit the degree of mandibular, as well as compensating, facial deformity. However, examination of the current concepts regarding the diagnosis, preparatory treatment, and surgical therapy of the dentofacial deformities is beyond the scope of the current discussion. The reader is encouraged to explore the many good publications that thoroughly discuss orthognathic surgery.2–10
Trauma
Treatment of condylar and subcondylar fractures varies on the basis of multiple factors. Nondisplaced fractures with minimal dysfunction may be treated with soft diet and guiding elastics. Moderate changes in occlusion or function may require short-term maxillomandibular fixation. In situations where the malposed segment is significantly displaced or interferes with jaw function, there are no occluding teeth on the involved side, or the condyloid processes are fractured bilaterally and grossly displaced, open reduction should be performed.11 Additional considerations for open reduction are the inability to perform maxillomandibular fixation and the presence of concomitant fractures in the mandible, maxilla, or midface.
Dislocation
Dislocation that is chronic can be treated by injection of a sclerosing agent into the TMJ capsule and lateral ligament to produce scarring of the stretched tissues,12 capsulorrhaphy, lateral pterygoid myotomy, temporal myotomy, or condylectomy.13 Decision as to the appropriate surgical procedure is based on the etiology, severity, and persistence of the dislocation.
Intracapsular Disorders
Anterior disk displacement is typically caused by trauma. This may be a single, macrotraumatic event or, more likely, frequent episodes of microtrauma that occur over a prolonged period. The majority of microtraumatic events are the parafunctional habits such as tooth clenching or grinding, which is also known as bruxism.14
Anterior Disk Displacement with Reduction
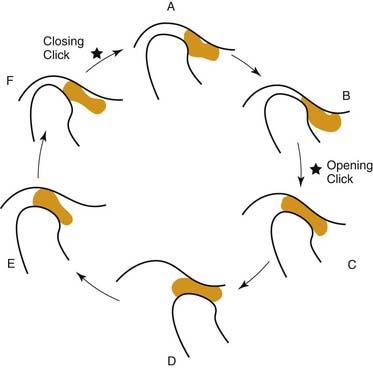
Anterior disk displacement with reduction is typically characterized by clicking or popping sounds on mouth opening (Fig. 94-1). Reciprocal or closing clicks are not consistently present. Patients who present with anterior disk displacement with reduction generally exhibit a normal range of mandibular motion. There may or may not be pain associated with mandibular movement. Multiple studies have shown that asymptomatic anterior displacement with reduction is common and often persists for years without signs of progression.14–16 It is believed that these asymptomatic, nonprogressive cases represent physiologic accommodation of the joint.17 They require no treatment. When pain is present, it is the general determinant of any functional limitation that exists. Treatment of these painful joints consists of soft diet, self-limitation of opening, NSAIDS, splint therapy, and physical therapy. Patients refractive to these conservative modes of therapy may be candidates for more invasive procedures such as arthrocentesis, arthroscopy, or open joint surgery.
Anterior Disk Displacement without Reduction
Anterior disk displacement without reduction is characterized by a closed lock (Fig. 94-2). In the nonreducing joint, forward translation of the condyle on mouth opening forces the disk anteriorly, causing it to become a physical impediment to further opening. The maximum interincisal opening (MIO) is generally only 25 to 30 mm, and the mandible deviates toward the affected joint. Lateral excursive movements of the mandible are generally restricted to the contralateral side but not to the ipsilateral side. Pain is a common symptom, particularly on forced opening (beyond the MIO).