Advanced stage disease at diagnosis
Early-stage disease at diagnosis when focal therapy is contraindicated or not available
Recurrence after focal therapy
Recurrence after chemotherapy
Post-enucleation with positive margins
Orbital extension
Metastases
When necessary, external beam radiotherapy is a highly effective nonsurgical treatment for retinoblastoma, but its effectiveness must be balanced against its potential for side effects because most patients are very young at the time of diagnosis and there is genetic susceptibility to further malignancy (Chap. 19).
14.2.1 Globe Preservation
Radiation therapy has an excellent track record in preserving the eye. In patients with the Reese-Ellsworth group I–II disease, tumor control rates measured at 5 years are in excess of 95 %. In patients with more advanced disease (Reese-Ellsworth groups III–IV), 5-year control rates reduce to approximately 50 %, owing partly to the greater tumor burden and intraocular extent of disease [6]. Patients with Reese-Ellsworth group Vb disease have 5-year eye-preservation rates of approximately 53 % [7]. Poor tumor control in advanced cases is often attributed to vitreous seeding.
14.2.2 Visual Acuity
Although data on visual acuity are relatively limited, most patients are reported to have good visual acuity (20/20–20/40) after radiation therapy; the rest have at least some prospect for functional vision (20/50–20/400) [8, 9]. Final visual acuity and field are affected by tumor location, which often depends on the patient’s age at the time of diagnosis: younger patients are more likely to have tumors in the macula (Fig. 14.1) [10].

Fig. 14.1
A child receiving external beam radiation therapy
14.3 Side Effects and Secondary Malignancies
The side effects of radiation therapy have framed current clinical trials to include avoidance of radiation therapy for patients with retinoblastoma. These side effects include ophthalmic complications, such as retinal detachment, vitreous hemorrhage, cataract formation, and glaucoma; somatic complications, such as orbital hypoplasia; and the most daunting of all side effects, the second malignant neoplasm (Chap. 19) (Fig. 14.2).
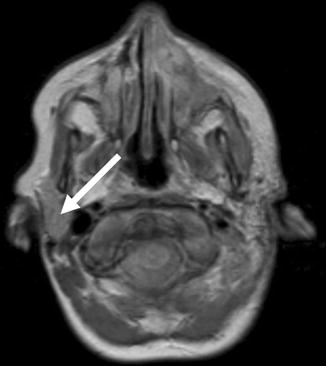
Fig. 14.2
Coronal magnetic resonance image showing a secondary malignancy (sarcoma indicated by arrow) in a patient treated for retinoblastoma
14.3.1 Risk of Second Malignant Neoplasms
The risk of second malignant neoplasms is highest among patients with the germ-line mutation of the retinoblastoma gene (RB1). They may occur without the use of radiation therapy, but radiation-induced tumors are the most frequent, and bone and soft-tissue sarcomas are the most common. Radiation-induced sarcomas are the secondary malignancies that cause most deaths, and more patients die from second malignant neoplasms than from retinoblastoma itself. In a recent SEER analysis, second malignant neoplasm accounted for 52 % of deaths for children with bilateral retinoblastoma [11].
14.3.1.1 The 1914–1984 New York/Boston Patient Series [12]
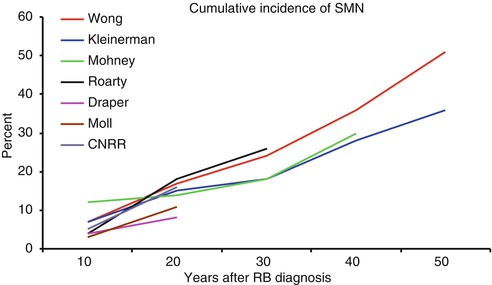
A report published in 1997 had a chilling effect on the use of radiation therapy in patients with retinoblastoma [12]. The report covered a 70-year experience (1914–1984) of treating 1,604 patients with bilateral retinoblastoma. The 50-year cumulative incidence of second malignant neoplasms in irradiated patients was 51 % (1 % per year) for patients with bilateral disease, but only 5 % for patients with unilateral disease (Fig. 14.3). The data clearly showed that radiation-induced tumors are the leading cause of death among long-term survivors. This article is the one most often quoted by parents whose child is referred to a radiation oncologist. It might seem irrational, on the basis of these results, to irradiate a child with retinoblastoma—the radiation oncologist is often put in a difficult position when the family is confronted with the news that external beam irradiation is the only option for ocular preservation.
14.3.1.2 The Incidence of Radiogenic Tumors Is Smaller in Other Series
Moll et al. reviewed 11 series reporting on malignancy induction, each including more than 50 patients, and published between 1966 and 1995, only four were without selection bias [13]. The 11 series included 35 second primary tumors, and three of the larger series showed cumulative incidences of second malignancy of 8 % at 18 years, 16 % at 20 years, and 19 % at 35 years (Fig. 14.3). The same group published an analysis of data from the Netherlands Cancer Registry [14], which included 639 patients diagnosed between 1945 and 1994; 241 had hereditary tumors, and more than 80 % were followed beyond 10 years. The cumulative incidence of a histologically confirmed second malignant neoplasm in patients with hereditary tumors was 3.7 % at 10 years and only 17.7 % at 35 years. Curiously, 7 of the 28 second malignant neoplasms in the data from the Netherlands Cancer Registry were melanoma. One might conclude that the lower incidence of second malignant neoplasms in this report than in the 1997 report [12] was due to the unique patient population that included central referral for an entire country, as well as the definition and types of second malignant neoplasms.
14.3.1.3 A 2005 Update on the 1914–1984 New York/Boston Patient Series
A recent report by Kleinerman et al. provided an update on some of the 1,601 previously studied retinoblastoma survivors through the year 2000 [15]. The analysis included nearly 1,000 patients with irradiated or non-irradiated tumors in patients with heritable retinoblastoma. The standardized incidence ratio (ratio of observed to expected cancers) was 22 in the irradiated group and 7 in the non-irradiated group, a threefold difference. The cumulative incidence of new cancers at 50 years was 38 % among those irradiated and 21 % in those not irradiated (Fig. 14.3). Sufficient data were available to determine risks of malignancy induction after orthovoltage irradiation (32.9 %) and modern megavoltage irradiation (26.3 %); this finding provided some indication that the use of newer radiation therapy modalities might reduce the risk of secondary malignancy. In this series, tissues calculated to receive a cumulative dose more than 0.4 Gy were considered at risk of radiation-induced malignancy. This definition augmented the risk of various tumors, from pineoblastoma to breast cancer. Although the authors justified their inclusion criteria on the basis of atom-bomb survivor data, the small number of events leading to the increased risk (three cases of breast cancer), and the lack of potentially influential clinical variables leaves these results open to debate among radiation oncologists. At face value, these results indicate that all external beam radiation modalities will result in an excess of secondary malignancies and that the use of any diagnostic x-ray procedure in the clinical assessment of patients with retinoblastoma should cease.
14.3.2 Patient Age at Radiation Appears to Be Important
In 1998, Abramson et al. determined that the risk of a second malignancy was smaller for patients older than 12 months than for patients younger than 12 months when they received radiation therapy [16]. The risk of secondary malignancies in patients irradiated when older than 12 months was equal to that in patients who did not receive radiation therapy. Therefore, delaying radiation therapy until the patient is older than 1 year appears to reduce the risk of a second malignancy. This information has played a prominent role in clinical decision making. Similar findings were observed by Moll et al., who reviewed the Dutch Registry of 1945–1997, which included 263 patients with heritable retinoblastoma [17]. In that series the cumulative incidence of second malignancy at age 25 years was 22 % in patients who were younger than 12 months of age at the time of irradiation and only 3 % in those irradiated after age 12 months. The infield tumor induction rate was 11 % in the younger patients and 3 % in the older ones, but this difference was not statistically significant. The “infield” evaluation is meant to specify the location of the event within the irradiated volume determined by detailed review of radiation portals or two- or three-dimensional dosimetry. The authors concluded that the similarity of the infield failure rates suggested that factors other than radiation therapy are involved in the induction of malignancy in younger patients and that the estimation of the risk of second malignancy depends on how the second malignancy is defined, how carefully the irradiated volume is analyzed, and how the statistical analysis treats pineoblastoma. In that study, pineoblastoma was not defined as a secondary malignancy.
14.4 Reducing Side Effects from Radiation Therapy
A number of measures may be taken to reduce the likelihood of second malignant neoplasms and radiation-related treatment effects in children with retinoblastoma [1]: delay radiation therapy until the patient is at least 12 months old [2]; reduce the total dose of radiation [3]; use episcleral plaque brachytherapy; and [4] apply new external beam treatment methods and modalities, including conformal radiation therapy, intensity-modulated radiation therapy, and proton-beam radiation therapy (Box 14.1).
Box 14.1. Measures to Reduce Radiation-Related Treatment Effects in Children with Retinoblastoma
Delay radiation therapy until the patient is at least 12 months old.
Reduce the total dose of radiation.
Use episcleral plaque brachytherapy (if applicable).
Consider new external beam treatment methods including conformal radiation therapy, intensity-modulated radiation therapy, and proton-beam radiation therapy.
14.4.1 Delay Radiation
The fact that delay of radiation until after age 12 months reduced the risk of second malignant neoplasms [16] provides hope that teletherapy may still have a major therapeutic role in the eyes with advanced disease that have had their tumor load reduced but not eliminated by primary chemotherapy. It is now common practice in some retinoblastoma centers to use systemic chemotherapy in patients with bilateral advanced disease diagnosed before 1 year of age, delaying radiation until after the first birthday.
14.4.2 Lower the Radiation Dose
The standard dose for irradiation is 45 Gy. One of the largest studies to show the feasibility of low-dose irradiation included 49 eyes in 38 patients treated with 36 Gy between 1978 and 1998 [18]. At a median follow-up of 88 months, rates of tumor control in patients who had undergone low-dose irradiation therapy were equivalent to those attained with higher doses in other series. The estimated 10-year ocular preservation rate was 82 ± 6 %. The 5-year ocular preservation rate for patients with Reese-Ellsworth group I or II tumors was 95 ± 4 % and for patients with Reese-Ellsworth group III or IV tumors, 66 ± 11 %. Ocular preservation rates after external beam irradiation at various doses indicate that low-dose external beam irradiation may be an option for selected patients. The role of response-based radiotherapy dosing for stage 4a and 4b retinoblastoma is currently being evaluated in a Children’s Oncology Group trial, ARET0321 (NCT00554788).
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


