 acial palsy, which usually affects only one side of the face, is a primary indication for tarsorrhaphy. In facial palsy, the blink reflex is affected and the front surface of the eye may dry out. When this occurs, tarsorrhaphy is indicated to partially close the eye to protect the cornea.
acial palsy, which usually affects only one side of the face, is a primary indication for tarsorrhaphy. In facial palsy, the blink reflex is affected and the front surface of the eye may dry out. When this occurs, tarsorrhaphy is indicated to partially close the eye to protect the cornea.
Tarsorrhaphy is not a simple procedure. Failed surgeries are common because the tarsal plates of the two lids often do not join as expected.
We have devised a procedure that uses stainless steel sutures to bring the tissues together. Raw areas on the lid margins are created using the Fugo blade. The Fugo blade offers a distinct advantage over manual incisions because it produces little or no bleeding.
TECHNIQUE
Anesthesia
Infiltrate the upper and lower lids with 2% lidocaine.
Surgical Technique
- Bring together the upper and lower lids where they are to be joined. Pass a stout nylon suture through both lids (Fig. 7.1). This secures and steadies the lids for the surgical steps to follow.
- Use a 100-µm Fugo blade tip, set at the lowest energy setting, to make two incisions on the intermarginal strip of each lid. Make the incisions about 5 mm apart and less than 1 mm deep.
- Incise the intermarginal strip between the two incisions and gently lift as a flap, starting from the side of the posterior lid margin and proceeding toward the ciliary edge. The flap may be about ¾ mm thick. Take care not to point the Fugo blade anteriorly, which would immediately cut the flap. Treat both lids the same way. The result is a flap each on the two lids and a raw strip of tarsal plate underneath, perfectly aligned (Fig. 7.2).
- Join together the two raw areas of the lid margins as follows. Pass an 80-µm vanadium steel suture from the raw side outward to a short distance from the cilia. Then reverse the suture and pass it from the skin to the raw area side. Repeat these steps in the opposite lid and pass the suture back through the raw areas (Fig. 7.3).
- Now, with one loop of vanadium steel sutures in each lid, use the two ends of the suture to bring the raw areas together. Tie the suture as a reef knot, taking care not to let the marginal flaps get in the way, and cut the suture close to the knot. The knot at this point is covered by the free marginal flaps. The suture becomes buried in the skin and causes no inflammation (Fig. 7.4).
- Suture the flaps from the two lids with 40-µm vanadium steel sutures. Two or three sutures are sufficient.
- Remove the temporary nylon suture holding the lids together.

Figure 7.1. The upper and lower lids are held together with a stout forceps as a thick nylon suture is passed across both lids and secured. Bottom right: Two vertical incisions are made on both lids with the Fugo blade.
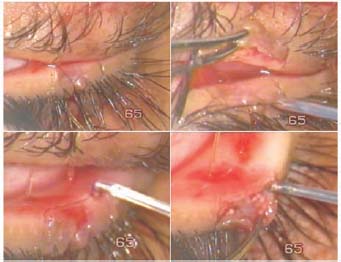
Figure 7.2. After making all four incisions, the lower lid flap has been made. A similar flap is then made in the upper lid.
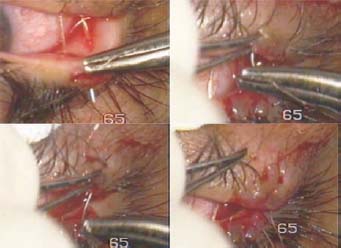
Figure 7.3. The 80-µm stainless steel suture is passed upward through the raw area of the upper lid and is then passed through the skin. The needle is passed through the raw area of the lower lid, then returned from the skin side. The two ends of the suture are tied, bringing the raw areas together.

Figure 7.4. Left: The 80-µm vanadium steel suture has been tied off. The suture is then cut under the flaps. Right: The 40-µm vanadium steel sutures have been applied, thus completing the operation.
For temporary tarsorrhaphy, you can join the lids with 80-µm vanadium steel sutures without creating raw areas on the lid margins.
Postoperative Management
- Remove the dressing after 3 hours.
- Prescribe local antibiotic drops, to be instilled five to six times a day for 15 days.
Summary
Failures with this operation are rare and are usually related to making insufficient flaps, poor suturing, or the use of sutures other than steel. Within days, the main supporting 80-µm steel suture becomes completely buried, as it cuts through the skin under the loops. It need never be removed. Similarly, the 40-µm sutures to the flaps never need to be removed.
Suggested Reading
Beyer-Machule CK. Malposition of lids. In: Heilman, K, Palon, D, eds. Atlas of ophthalmic surgery. New York, NY: Thieme, 1985:1.36–1.37.
Iliff NT. Surgery of the eyelids and lacrimal drainage apparatus. In: Rice TA, Michels RG, Stark WJ, eds. Ophthalmic surgery. St. Louis, Mo: Mosby, 1984:40–41.
Roy FH. Master techniques in ophthalmic surgery. Baltimore, Md: Williams & Wilkins, 1985:740–741.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


