Chapter 149 Systemic Evaluation and Management of Patients with Uveal Melanoma
Introduction
In developed nations, patients with metastatic uveal melanoma rarely present with the classic “distended abdomen and artificial eye.” Occurring in up to 50% of cases, most metastases are asymptomatic and found by hematologic and radiographic screening.1–3 The rationale for screening is that early detection allows for both palliative treatment or enrollment in clinical trials. Furthermore, early detection offers patients more time to plan future medical and personal care. Indeed, Eskelin and associates demonstrated that largest tumor dimension of metastasis and serum alkaline phosphatase levels could be correlated to median patient survival.4 Survival extends from 2.5 months to 14 months in patient subgroups with the lowest tumor burden at diagnosis.4,5 Screening aims at uncovering smaller, less numerous and even solitary metastases. Though the liver is typically involved in over 80% of cases, alternative common sites include bone and subcutaneous skin.2,3,5,6 Since the liver is most commonly involved, periodic radiographic abdominal evaluations are widely recommended for early detection of metastases.7 Unfortunately, there exist no standardized practice guidelines nor comparative studies to determine the relative efficacy of current staging and screening methods for metastatic uveal melanoma.
Physical examination
Most retinologists and eye cancer specialists will not disrobe patients for examination. However, they can play an integral role during their periodic patient interactions. For example, a history of weight loss, subcutaneous nodularity or abdominal pain should raise suspicion. The eye cancer specialist should ensure or coordinate systemic patient care including: a physical examination looking for subcutaneous nodularity, organomegaly and periodic clinical testing. (Additionally, use of the 7th edition of the American Joint Committee on Cancer’s (AJCC) site-specific universal staging system enables analysis of risk factors for metastasis and multicenter cooperative studies.8)
Serology: liver function tests
Liver function tests (LFTs) include gamma-glutamyl transpeptidase, lactate dehydrogenase, alkaline phosphatases, aminotransferases and bilirubin. When considered individually, they have demonstrated reported sensitivities ranging between 0.27 and 0.67 for metastases detection.9 However, in studying the 2320 patients enrolled in the Collaborative Ocular Melanoma Study (COMS), the authors concluded that sensitivity, specificity, positive predictive value and negative predictive value associated with at least one abnormal LFT before diagnosis of metastatic disease were 14.7%, 92.3%, 45.7% and 71.0%, respectively.9 Elevated LFTs are thought to be less sensitive for and specific to the diagnosis of hepatic metastases than radiographic imaging. Therefore, LFTs should be used for metastases screening only as a complement to radiographic imaging.9
Radiologic assessment: computerized tomography, magnetic resonance imaging and ultrasonography
The liver is easily visualized through various radiographic imaging procedures. In general, ultrasonography (US) can uncover metastases not detected by LFTs.7,10 Contrast enhanced US will demonstrate increased sensitivity and specificity over standard US.10 Triphasic computed tomography (CT) has shown excellent sensitivity, but has a low positive predictive value due to misleading benign lesions found on imaging.11 Contrast-enhanced magnetic resonance imaging (MRI) is considered to be the most sensitive hepatic imaging tool.12 However, there exists concern about gadolinium-associated renal toxicity and is contraindicated for patients with metallic implants. Consequently, without a preferred practice pattern, the choice of imaging is largely governed by cost, radiation exposure and physician preferences.
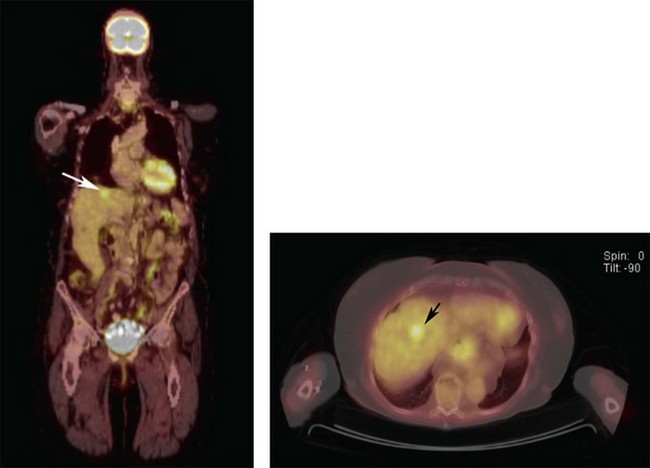
Positron emission tomography/computed tomography
Unlike the previously mentioned radiographic imaging modalities, positron emission tomography/computed tomography (PET/CT) was the first to add PET-function to CT-form on the same diagnostic page (Fig. 149.1).13,14 This enabled discrimination between inflammatory and neoplastic tumors. In contrast to abdominal CT, MRI and US, PET/CT routinely allows for whole body scanning and staging. In practice, we have found PET/CT to yield a remarkably high positive predictive value for uveal melanoma metastases detection.2,3 In addition, PET/CT has been used for initial and follow-up tumor staging as well as detection of synchronous cancers, determination for risks for metastasis, evaluation of post-irradiation tumor viability and for clarification of suspicious CT or MRI findings.13–18 The potential benefits of PET/CT screening have been downplayed due to radiation risks and cost. In our opinion, though most patients prefer initial total body scanning, those at high risk for metastatic uveal melanoma (e.g., T3 and T4 tumors) may be the subgroups to most benefit from PET/CT imaging.3
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


