OVERVIEW
- Dysphagia is the symptom of swallowing impairment
- There are four stages of swallowing: oral preparatory, oral, pharyngeal and oesophageal
- Weight loss, when associated with dysphagia, indicates significant disease and needs urgent investigation
- Aspiration is defined as liquids or solids penetrating below the level of the vocal cords, and can be associated with both neurologic and neoplastic conditions
- Multidisciplinary evaluation may be necessary for diagnosis, treatment and rehabilitation
Dysphagia is a symptom experienced when there is an impairment or alteration of the swallowing mechanism leading to difficulty moving food and liquid through the mouth, pharynx or oesophagus. This should be differentiated from globus pharyngeus, where there is a sensation of irritation, tightness or foreign body in the throat, usually noticed at rest and is not affected or relieved by pharyngeal movement. Dysphagia can be an indicator of disease in body systems, from neurological through to hormonal and metabolic. Department of Health figures for 2010–11 record more than 34 000 primary diagnoses of dysphagia in the UK.
Physiology
The swallowing action can be divided into four stages: oral preparatory, oral, pharyngeal and oesophageal. The oral preparatory stage is under voluntary control and good motor control of the facial and lingual musculature is essential. It is characterised by increased tone of the lip, buccal and facial muscles, lateral jaw motion and rolling movement of the tongue from side to side that moves the food bolus for mastication. The oral stage is also under voluntary control, when the tongue pushes the prepared food bolus towards the oropharynx. Contact of the bolus with the anterior tonsillar pillar is traditionally thought of as the trigger point to initiate the pharyngeal stage. The oral stage lasts approximately between 1 and 1.5 s. Tongue movement plays the most important part in these two stages.
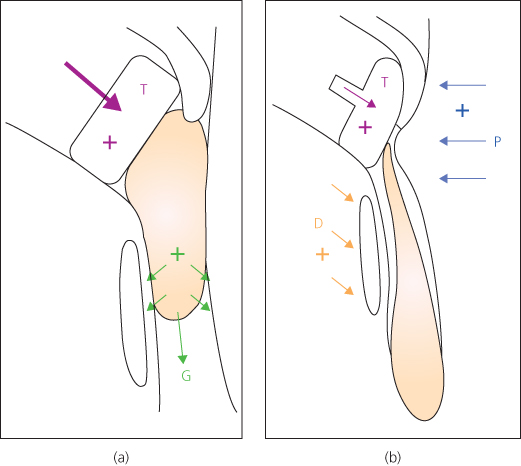
The pharyngeal stage (Figure 20.1) lasts only a second, but is accompanied by numerous neuromuscular activities controlled at the brainstem level. The soft palate closes against the nasopharynx to prevent nasal regurgitation and laryngeal closure occurs to prevent aspiration. Three tiers are involved in laryngeal closure, including the epiglottis and the aryepiglottic folds, the false cords and the true cords. Adduction of the true cords occurs before the other tiers (although there may be individual variation) and plays an important role in airway protection. The epiglottis may play a greater role in directing the bolus into the piriform sinuses than in protecting the airway. Surgical resection of the upper two tiers alone is compatible with aspiration-free swallowing as they can learn to compensate by using an airway protection technique (see therapy). Following laryngeal closure, the pharyngeal constrictor muscles sequentially begin contracting to propel the bolus. The suprahyoid muscles elevate the larynx, clearing the bolus down and the cricopharyngeal sphincter opens, admitting the bolus into the upper oesophagus. The resting tone of the cricopharyngeus reduces with laryngeal elevation and upward movement of the larynx mechanically pulls opens the sphincter and is further opened by bolus pressure. The oesophageal stage is of variable duration, lasting between 8 and 20 s.
Figure 20.1 Pharyngeal phase of swallowing: (a) early phase. (b) late phase. D, depression; E, elevation; G, gravity; T, tongue; +, positive pressure; −, negative pressure.
Symptoms
Swallowing problems can present as difficulty in initiating the swallow, choking or coughing upon swallowing (aspiration), or a sensation of obstruction at the level of the neck or behind the sternum. Dysphagia can be a problem with solids or liquids or both. Dysphagia that is limited to solids initially, progresses to liquids over a period of weeks to months, and is accompanied by weight loss raises suspicion of a malignant lesion. Very slow progression over years occurs in achalasia of the cardia and pharyngeal pouches (Zenker’s diverticula), associated with regurgitation of undigested food. Dry mouth (xerostomia) caused by autoimmune diseases (e.g. Sjögren’s syndrome) and radiation therapy also causes dysphagia.
Weakness of the oral and lingual musculature can lead to drooling and poor mastication. Altered sensation to the pharynx caused centrally (e.g. neurologic disease) or peripherally (e.g. postradiotherapy), can lead to a delay in the initiation of the pharyngeal stage, and food can slip into the oropharynx. This can cause aspiration, as the airway is unprotected except for a very short time during the pharyngeal stage. Aspiration usually manifests as coughing and choking episodes, or a ‘wet’ voice quality. Aspiration can also be caused if any of the laryngeal protective mechanisms are impaired, commonly due to neurologic or neoplastic processes. The severity of the problem will dictate the symptomatology. Minor aspiration is characterised by throat clearing and coughing after swallowing, while significant aspiration can cause choking episodes and pneumonitis. Silent aspiration can also occur in the absence of any of the above symptoms, when laryngeal sensation is impaired.
Clinical evaluation
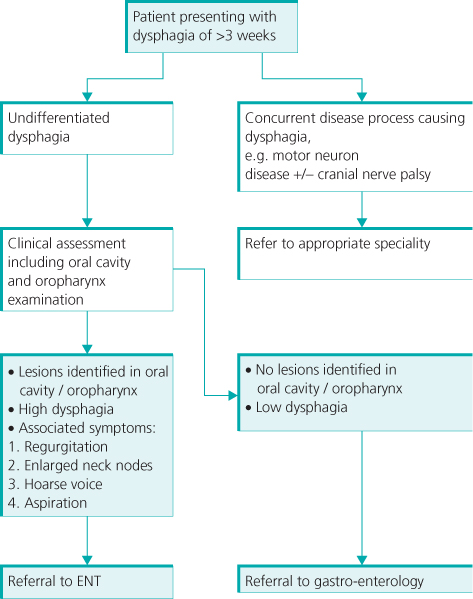
The aim of clinical examination is to assess the swallowing performance and establish the cause of dysphagia. A careful history is required regarding onset of the problem, the severity of dysphagia, weight loss, aspiration, regurgitation and dysphonia. The history can give good pointers towards the diagnosis in 80% to 85% of patients. Acute dysphagia is usually caused by foreign bodies. Meat boluses may pass spontaneously, but most others will need endoscopic management. Dysphagia of longer than three weeks duration needs specialist referral (Figure 20.2). A comprehensive otolaryngologic examination is mandatory, and this includes a flexible fibreoptic assessment of the nasopharynx, hypopharynx and larynx. Lesions in the apex of the pyriform sinus and the postcricoid region may not be evident on flexible endoscopy.
Transnasal flexible oesophagoscopy (TNO) (Figure 20.3
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


