OVERVIEW
Vertigo is caused by vestibular disturbance and is the result of:
- Intrinsic labyrinthine diseases—Menière’s disease, benign paroxysmal positional vertigo and acute vestibular failure
- Spread of disease from an infected middle ear to the labyrinth
- Disease in the brainstem or cerebellum
- General systemic conditions affecting the vestibular system
Vertigo, by definition, is an illusion of movement, of the patient or the surroundings. The origin of the name suggests a sense of rotational movement, but should apply to any direction of movement experienced. Imbalance always accompanies vertigo, but is not always due to vertigo and is not a synonym. Imbalance occurs for many reasons without vertigo.
Normal balance needs:
- accurate sensory information from the eyes, proprioceptive receptors and the vestibular labyrinth with coordination of this information within the brain
- normal motor neural control by the central nervous system of an intact musculoskeletal system: normal muscles and joints (Figure 8.1).
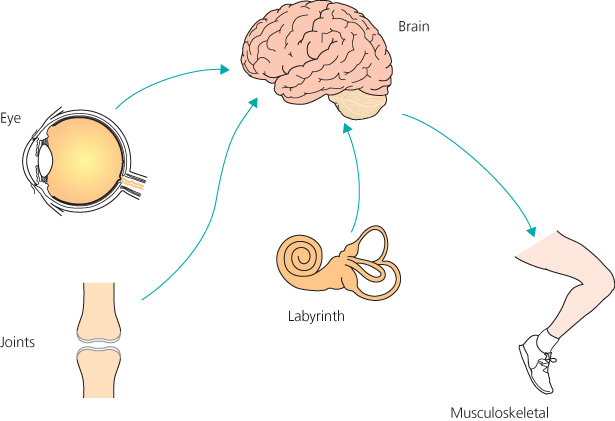
Defects in any of these impair balance—with or without vertigo.
Vertigo arises if information from vestibular sources conflicts with data from the other sensory systems, or when a disordered central integration system in the brain does not correctly relate the body’s movements to the vestibular input. Vertigo is always a symptom of vestibular defect. This may lie in the labyrinth (peripheral) or in its connections within the brain (central). When severe, it is accompanied by nausea and vomiting.
Vertigo is caused by: (a) peripheral vestibular disorders (labyrinthine); (b) middle ear infections spreading to the labyrinth; (c) central vestibular disorders, such as multiple sclerosis, tumours, infarcts; and (d) external damage to the vestibular system—trauma, drugs, anoxia, anaemia, hypoglycaemia, hypotension or viral infections (Box 8.1).
- Peripheral (labyrinthine)
- Central: in the brain (brainstem, cerebellum or higher)
The commonest peripheral vestibular disorders (labyrinthine) are Menière’s disease and other forms of endolymphatic hydrops, benign paroxysmal positional vertigo, sudden vestibular failure and vascular disturbances (Box 8.2).
- Menière’s disease
- Benign paroxysmal peripheral vertigo (BPPV)
- Sudden vestibular failure
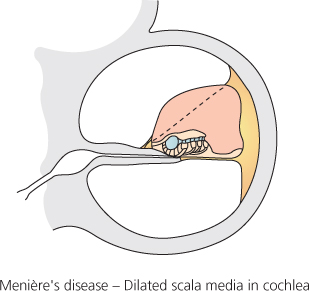
Menière’s disease (idiopathic endolymphatic hydrops)
This is a disorder of endolymph control, associated with dilatation of the endolymphatic spaces of the membranous labyrinth (hydrops) (Figure 8.2). This dilatation, or endolymphatic hydrops, may be caused by disorders of the otic capsule, but in Menière’s disease it is, by definition, idiopathic.
The disease usually affects only one ear, first producing symptoms between the ages of 30 and 60 years. It is characterised by attacks of violent paroxysmal vertigo, often rotatory, associated with deafness and tinnitus. Attacks occur in clusters with periods of remission, during which balance is normal. Each lasts for several hours, rarely less than 10 minutes or more than 12 hours (Box 8.3), and is accompanied by prostration, nausea and vomiting. A sensation of pressure in the ear, increase or change in the character of tinnitus, pain in the neck or increased deafness often precedes an attack.
- Menière’s disease: hours
- Benign paroxysmal positional vertigo: seconds only
- Sudden vestibular failure: days
The accompanying deafness is sensorineural and fluctuates noticeably in severity. It is associated with distortion of speech and musical sounds, and with severe discomfort on exposure to loud noise (hyperacusis). Hearing loss may precede the first attack, although both symptoms may first arise together. The vertigo may be so catastrophic that hearing loss is not noticed. Hearing improves during remission, but gradually deteriorates persistently, until its impairment becomes severe. The tinnitus is roaring, low-pitched and worse when hearing is most impaired.
At least 20–30% of patients have disease in both ears. The prevalence of bilateral disease varies widely in reports from different centres, with implications for treatment, and deafness then tends to become more worrying than the vertigo. A variant known as vestibular hydrops produces attacks of episodic vertigo without any auditory symptoms. Another variant of Menière’s disease is cochlear hydrops, which is a very common cause of fluctuating hearing loss with tinnitus and distortion, but without vertigo. This common complaint may often be ascribed incorrectly to Eustachian tube obstruction.
Similar vestibular vertigo may be secondary to total cochlear hearing loss from any cause. It has been seen by the author, usually after many years, when the deafness has arisen congenitally, after mumps viral infection or head trauma.
Treatment of Menière’s disease
Medical treatment is usually chosen from an armamentarium including histamine agonists such as Betahistine (Serc), often used in the UK as a first choice (but not in the USA, since the FDA consider evidence of efficacy to be insufficient), vasodilator drugs such as nicotinic acid in a dose sufficient to cause flushing, diuretics combined with a sodium-restricted diet and corticosteroids. These treatments may need symptomatic support with antivertigo drugs. This wide range of medication is testimony to our continuing uncertainty about the underlying causes of this disorder.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


