OVERVIEW
- Any patient who is hoarse for longer than 3 weeks needs an urgent chest X-ray, and if negative an ENT referral for a laryngoscopy
- Any patient with “red flag” symptoms should be referred urgently
- Understanding the anatomy and physiology of the larynx allows the clinician to make an accurate provisional diagnosis from the history and listening to the patient’s voice
- Histologically proven laryngeal cancer in an early stage is likely to be cured
- Assessment in the ENT clinic ideally involves a multidisciplinary approach with a speech and language therapist and laryngologist
What is voice?
There are three essential components to voice production:
A problem located with any of the three listed above can affect voice—for example if you pinch your nose the voice assumes a nasal quality—but this chapter will concentrate on disorders of the larynx and the vocal cords.
The human voice—unique!
In most animals the larynx lies either above or at the level of the palate (or its equivalent). In some cases this allows constant stimulation of the olfactory organs which are much more sensitive than in the human and necessary for survival, but more importantly it separates the feeding passages from the airway. The human is unique in that the larynx descends down to the level of the sixth cervical vertebra which increases the volume of the vocal tract and contributes to the complexity of the human voice. As a result of this lower position the primary function of the larynx is to protect the distal tracheobronchial tree and prevent any aspiration and voice production is very much secondary to this. The third function of the larynx is to provide a closed glottis so that the diaphragm can be splinted for lifting and/or straining (Box 17.1).
- Protection of the distal tracheobronchial tree
- Production of voice
- Closed glottis on straining or lifting to give support to the diaphragm
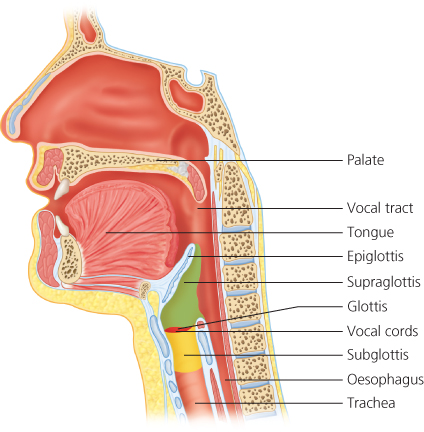
Anatomy of the larynx
There are three divisions (Figure 17.1):
Embryology
The larynx is the perfect organ to demonstrate the importance of embryology and how easy it is to remember its anatomy and nerve supply. The supraglottis comes from the IVth branchial arch (nerve supply: superior laryngeal nerve)—the Vth branchial arch disappears in the human—the subglottis from the VIth branchial arch (nerve supply: recurrent laryngeal nerve). The glottis lies between these and as a result has very poor lymphatic drainage—inflammation can give very swollen vocal cords but conversely any glottic tumour has a good prognosis as its lymphatic spread is poor—a T1 carcinoma of the glottis has a 95% cure rate either with radiotherapy or laser resection.
Remember that the laryngeal nerves lie in close proximity to the thyroid gland and can be damaged at surgery. It is also worth remembering that the recurrent laryngeal nerve on the left passes down into the chest so that one of the presenting signs of a bronchial tumour may be hoarseness.
Vocal cords in normal voice
The vocal cords open (abduct) to allow breathing and close (adduct) during voice production (Figure 17.2).
Figure 17.2 The “normal anatomy” of the larynx and hypopharynx (the vocal cords are in their resting position).
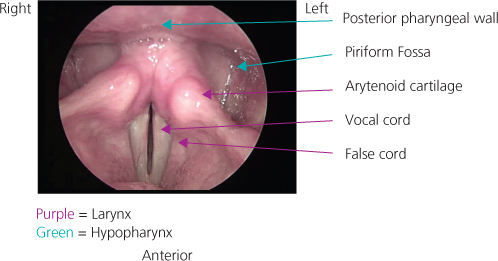
As air passes up from the lungs it causes the membranous parts of the vocal cords (vocal folds) to vibrate. The vocal folds vibrate 100 times per second in the male and almost double this in the female—this gives the female voice a higher pitch but may also explain the predominance of vocal pathology in females. To vibrate at this rate, the vocal folds need to be well lubricated—consider trying to blow a raspberry with dry versus moist lips. The dryness associated with any inflammation will affect vibration hence the importance of steam inhalations and good hydration in these situations, especially in singers.
Changes in the vocal folds can be considered in four subgroups:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


