OVERVIEW
- Discharge from the ear is an unpleasant symptom that in some communities can result in stigmatisation
- Before an accurate diagnosis can be made, the discharge should be cleared by microsuction or dry-mopping
- Topical antibiotic/steroid drops are most effective in treating otitis externa
- Discharge due to chronic otitis media occurs in the presence of a defect in the eardrum
- Cholesteatoma can be associated with serious complications
Discharge from the ear is an unpleasant symptom that reflects infection, inflammation, trauma or rarely neoplasm of the external or middle ear (Box 3.1). Persistent ear discharge and its associated odour can result in stigmatisation and social isolation in some communities (Figure 3.1).
- Otitis externa (acute and chronic)
- Otitis media (acute and chronic)
- Trauma to the temporal bone
- Neoplasms of the ear (very rare)

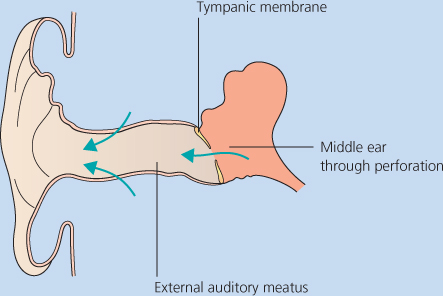
The discharge itself arises either from the skin of the external ear canal, the surface of the tympanic membrane (eardrum), or the lining of the middle ear cleft (Figure 3.2). Discharge from the middle ear cleft often is profuse and mucoid in nature, because of the mucosal lining of the middle ear. In the clinical management of a discharging ear, accurate diagnosis is important and is facilitated by thorough history taking and examination. ENT specialists have the advantage of the use of the operating microscope available in the outpatient setting (Figure 3.3). Using the microscope in combination with suction equipment allows the specialist to aspirate discharge and closely inspect the ear canal and tympanic membrane. In the primary care setting discharge can be removed by so-called dry-mopping using cotton wool on a suitable applicator.

Topical medications for discharging ears
The most useful medications for the treatment of ear discharge are delivered topically, usually in drop form, but also as ointments and creams. They contain a combination of antibiotics, antifungals, antiseptics, solvents and steroids. In this method, the ear to be treated is placed uppermost and drops instilled using the so-called displacement method. In this way pressure on the tragal cartilage forces the drops down the ear canal and, in the presence of a perforated eardrum, into the middle ear (Figure 3.4). The use of ear drops in the presence of a perforated eardrum is controversial, and centres around the use of preparations containing aminoglycoside antibiotics such as neomycin, gentamicin and framycetin. These antibiotics are particularly effective in discharging ears because they act against the Gram negative microorganisms such as Pseudomonas aeruginosa that are most commonly found in these conditions. Aminoglycosides given systemically are toxic to both the auditory and vestibular parts of the inner ear. In the UK, the “data sheets” for topical aminoglycoside preparations contraindicate their use in the presence of a perforated eardrum. Nevertheless British otologists widely use aminoglycoside ear drops in treating discharging ears. The risk to the inner ear from aminoglycoside ear drops is very small indeed. Current ENT-UK guidance (Philips et al. 2007) permits their use for actively discharging ears for up to 2 weeks at a time. Other antibiotics such as quinolones (ciprofloxacin and ofloxacin) are not ototoxic and are often effective. The overuse of quinolones, however, can theoretically lead to the development of bacteria resistant to these antibiotics.

Chronic otitis externa
A number of factors predispose to the development of chronic otitis externa (Box 3.2). Normally the ear canal is kept clean by the process of epithelial migration. Desquamated skin from the deep ear canal is carried outwards where it mixes with cerumen produced by glands and is discharged from the ear canal as ear wax. Any factor that disturbs this natural process makes the development of chronic otitis externa more likely. Keen swimmers and surfers can develop bony overgrowth (exostoses) of the ear canal, which predispose to chronic infection (Figure 3.5
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


