OVERVIEW
- Treat one-sided ear symptoms or one-sided head and neck symptoms with respect
- Whilst most tumours in the cerebellopontine angle are benign, their location is hazardous
- With the above and if the ear canal and eardrum are normal—refer
- Have a very low threshold for requesting an MRI scan
- Management options for acoustic neuromas are many and there is no single “best” treatment plan
- Most forms of management require long-term follow-up with careful record keeping, repeat MRI scans and review
The cerebellopontine angle
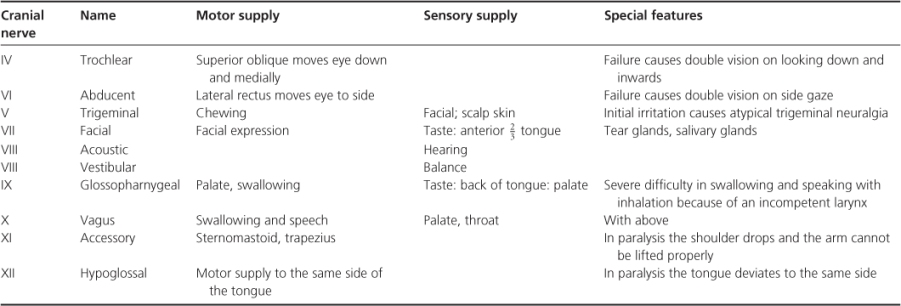
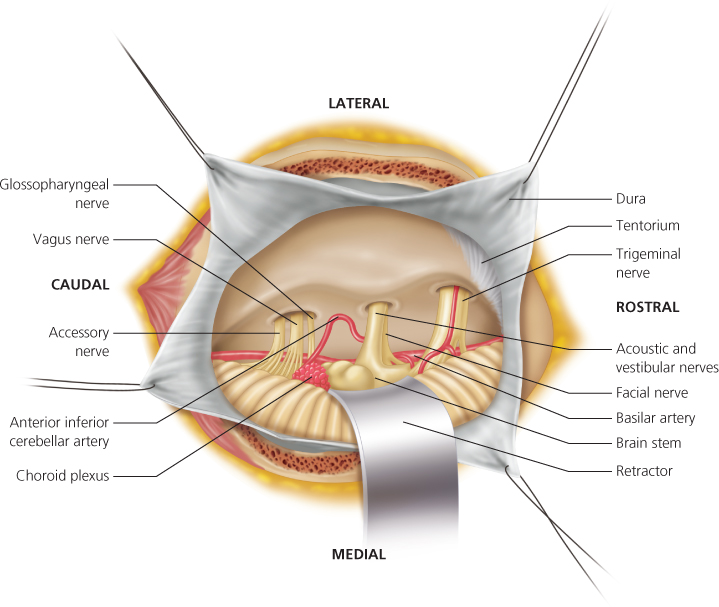
The cerebellopontine angle (CPA) is a tapered space between the skull and the brainstem and cerebellum, and is part of the posterior cranial fossa. It is an anatomist’s dream because the boundaries of the space and the structures that run through it are many and varied and the symptoms that can arise from disease or damage to these structures are protean and can be severely disabling or in extreme fatal. The side wall of the space is the medial aspect of the petrous temporal bone housing the labyrinth. The roof is the tentorium, the tough membrane that separates the posterior cranial fossa from the middle cranial fossa. The medial wall of the space is bounded by brainstem (or pons) and the lateral lobe of the cerebellum. The CPA is filled with cerebrospinal fluid (CSF) and has important sensory and motor nerves crossing it on their way to and from the brain (Table 6.1 and Figure 6.1). A major branch of the basilar artery is the anterior inferior cerebellar artery (AICA) which courses through the CPA and itself has important branches to the pons and to the labyrinth supplying the cerebellum in part.
Table 6.1 Simple description of the nerves of the CPA and their major functions.
Running along the length of the brainstem between it and the cerebellum is the CSF-filled IVth ventricle. This has to be open to allow the circulation of the CSF and obstruction results in raised intracranial pressure and eventually an obstructive hydrocephalus.
The acoustic and vestibular nerve bundle runs across the middle of the CPA from the inner ear to the brainstem. It arises from the sensory epithelium of the cochlea and vestibular labyrinth. There is one acoustic nerve bundle but three vestibular nerve branches—superior, inferior and singular—which join and then fuse with the acoustic nerve close to the brainstem. The facial nerve runs out from the brainstem a little ahead of the acoustic and vestibular but all the nerves run through the internal auditory meatus or canal (IAM or IAC) in the petrous temporal bone (Figure 6.2). The facial nerve takes a complex path through the bone turning first forwards at the geniculate ganglion, then backwards across the middle ear, then downwards through the mastoid bone and finally forwards again through the parotid gland on its way to the muscles of facial expression (Figure 6.3) (see Chapter 9).
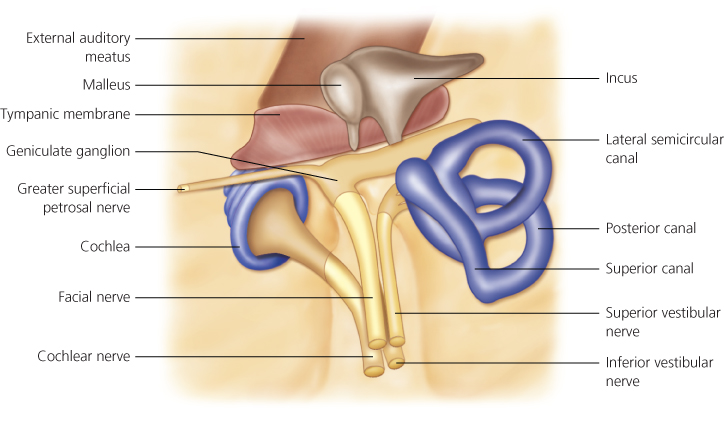
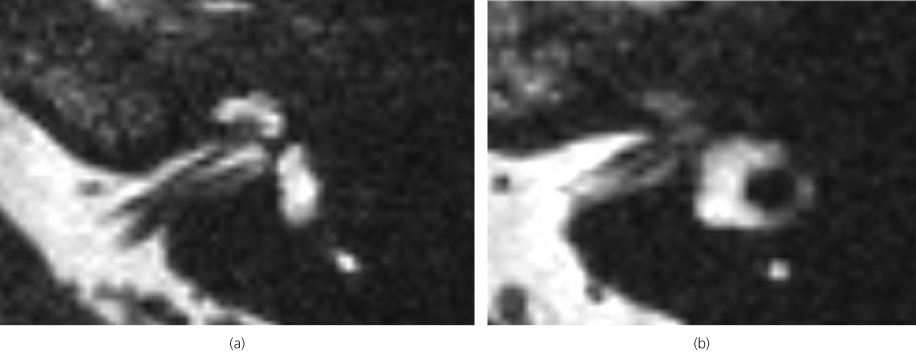
Figure 6.3 Axial MRI scan of a normal IAM with a “cut” (a) through the cochlea and showing the cochlear nerve to the left and the inferior vestibular nerve to the right; (b) through the lateral semicircular canal and showing the facial nerve to the left and the superior vestibular nerve to the right.
Growths in the CPA
With the diversity of structures in the CPA, it is not surprising that many different tumours can grow there. Fortunately, most of them are benign and by far the most common is the doubly misnamed acoustic neuroma. Not only do these usually develop on the superior vestibular nerve, but they are tumours of the nerve sheath cells—the Schwann cells—which make the myelin sheets that insulate the nerve fibres. Thus they should correctly be called vestibular schwannomas and any web search should include this term or the term neurilemmomas, which is also sometimes used by purists and pedants. They seem to arise from a single defect on the long arm of chromosome 22 which is why they rarely, if ever, become malignant, although with continued growth they can be fatal.
The incidence of acoustic neuromas has usually been quoted as 1 in 100 000 per year. With improved imaging and a greater awareness of the condition, the incidence seems to be increasing slightly. However, the post-mortem prevalence seems much higher, which suggests that many people go to their graves with these tumours rather than because of them (see “Diagnosis”).
The next most common growth is a meningioma which arises from the meninges of the inner surface of the skull in this region. They are generally slow growing and of low-grade malignancy. The other lesions that can occasionally be found in the CPA are listed in Table 6.2.
Table 6.2 Lesions in the CPA and their frequency of occurrence.
| Type | Percentage |
| Acoustic Neuromas | 75 at least |
| Meningiomas | 6 |
| Cholesteatomas | 6 |
| Gliomas | 3 |
| Others | 10 at most |
| Metastatic tumours | |
| Osteomas | |
| Osteogenic sarcomas | |
| Neuromas of V, VII or IX | |
| Angiomas | |
| Papillomas of choroids plexus | |
| Teratomas | |
| Lipomas |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


