OVERVIEW
- Airway obstruction may present as an emergency, requires a high index of suspicion to prevent a catastrophe, and should prompt immediate hospitalisation
- Stridor is caused by turbulent flow of air through a partially obstructed segment of the respiratory tract and can be diagnosed on the phase it manifests in the respiratory cycle
- Acute sudden onset of stridor, in an apyrexial and previously normal person, should arouse suspicion that a foreign body has been aspirated
- In the absence of any definitive precipitating cause and relevant history, acute and chronic stridor in adults should be considered to be neoplastic until proven otherwise
Of all emergencies seen in otolaryngologic practice, diagnosing and managing airway obstruction is one of the most complex, needing multiprofessional input and an experienced team to achieve good outcomes. The upper airway can be obstructed by a range of disease processes, from pathology in the anterior nasal cavity to the lower airways. Problems associated with breathing usually present as nasal obstruction, stertor and stridor. Nasal diseases are discussed elsewhere and this chapter will focus on pathology in the larynx, pharynx and trachea that causes airway obstruction.
Pathophysiology
Breathing is under involuntary control and is mediated by the respiratory centre in the brainstem. The vocal cords abduct during inspiration and with the negative pressure caused by diaphragmatic contraction and expansion of the lungs, air is drawn into the lungs. The recurrent laryngeal branches of the vagus nerves control vocal cord movement, with a complex arrangement of intrinsic muscles in the larynx providing fine control. The cricoid cartilage is the only complete ring in the respiratory tract, and surrounds the subglottic region. Thus, any airway oedema compromises the lumen, and even a minimal reduction in the airway can cause dramatic compromise of the airflow. Thus, 1 mm of mucosal oedema reduces the cross-sectional area by more than 40%.
Stridor is a harsh, vibratory noise caused by turbulent flow of air through a partially obstructed segment of the respiratory tract. This should be differentiated from stertor, where the noise is caused by vibration of the pharyngeal structures, such as the soft palate, during sleep and leads to a lower-pitched noise. Respiratory distress may not be a feature where a chronic, non-progressive lesion causes stridor and the patient has adapted well. Stridor can be present during the inspiratory or the expiratory phase or be biphasic; this can inform the site of obstruction (Box 18.1).
- Inspiratory: supraglottic and glottic obstruction
- Expiratory: low tracheal obstruction
- Biphasic: glottic and subglottic obstruction
Stridor in children
Evaluation
A careful history provides useful pointers to the diagnosis (Box 18.2). A previously well child presenting with acute onset stridor should arouse suspicions of foreign body aspiration. A preceding upper respiratory tract infection (URTI) indicates croup or bacterial tracheitis. Epiglottitis (supraglottitis) typically presents as rapid onset fever, dysphagia and drooling in children aged between 2 and 7 years.
- Age of onset
- Duration/phase of stridor
- Worsening/improvement of stridor since onset
- Precipitating causes
- Failure to gain weight
- Breath-holding spells
- Fever
- Feeding /swallowing problems
- Hoarse/muffled voice
- Intubation in the past
- Cough/chest infections
The child with acute stridor is ideally assessed in a setting where instrumentation and experienced personnel are available for emergency intervention to secure and stabilise the airway. The areas that clinical assessment should cover are shown in Box 18.3. Respiratory rate and level of consciousness are the most important indicators of severity of obstruction. Increasing intensity of the sound is not an indicator of the severity, as in severe obstruction the airflow is significantly diminished and thus no stridor may be heard. Measures should be taken not distress the child further for fear of precipitating an acute obstruction. This includes keeping the parent or carer at all times with the child, until the airway is secure. With increasing hypoxia and carbon dioxide retention, the child can become drowsy and unresponsive.
- Respiratory rate
- Cyanosis
- Apnoeic spells
- Use of accessory muscles
- Intercostal/sternal retraction
- Nasal flaring
- Timing/severity of stridor
- Hoarseness
- Temperature/toxicity
- Level of consciousness
- ENT examination in controlled setting
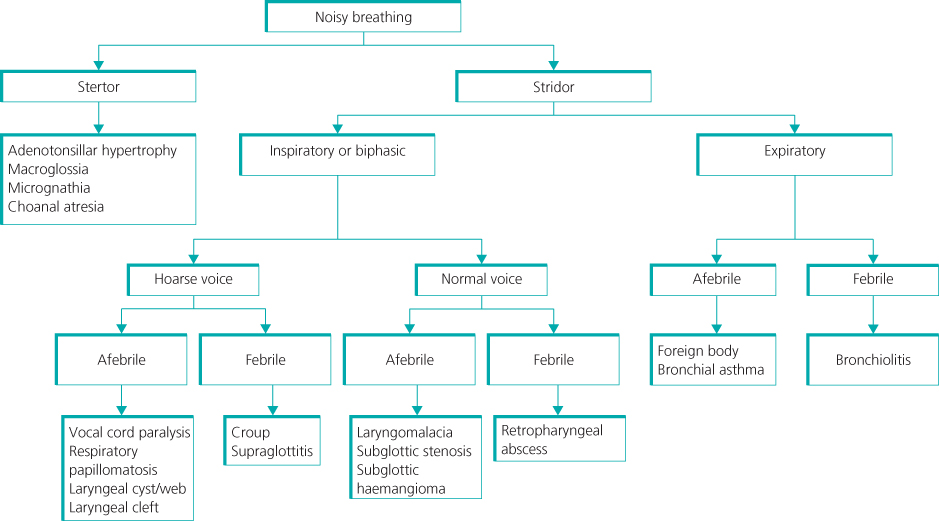
A working diagnosis of the cause of obstruction can be made in the majority of cases before direct examination of the airway (Figure 18.1). Most of these conditions are in the evolving phase when initially seen, and if observation only is planned, this is best done in an intensive care or high-dependency setting where rapid intervention is possible if the patient deteriorates.
Congenital structural lesions rarely present in the acute setting. For children with chronic stridor a diagnostic laryngotracheoscopy will be required in the majority of patients, unless the condition is mild and readily diagnosed on clinical examination alone. In the cooperative child with no evidence of hypoxia, flexible laryngoscopy in the clinic can be very informative. Surgical treatment is usually necessary for chronic obstruction that doesn’t respond to conservative treatment.
Acute stridor
Retropharyngeal and peritonsillar abscesses
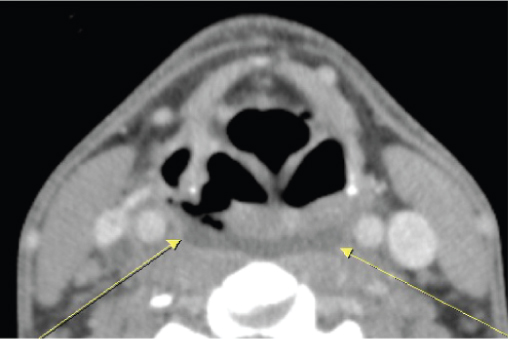
Drooling, painful swallowing and systemic upset are usually seen at presentation, usually with a preceding URTI. Retropharyngeal abscesses in the lower pharynx can cause laryngeal oedema and stridor. Neck stiffness and torticollis, if present, can help differentiate this condition from supraglottitis. Once suspected, imaging is recommended to confirm the diagnosis and identify the extent of the abscess collection (Figure 18.2). Peritonsillar abscesses are associated with trismus and more likely to present with stertor and do not need imaging. Urgent drainage is required for both conditions.
Figure 18.2 CT image of a retropharyngeal abscess showing an abscess cavity (arrowed) and generalised soft tissue swelling.
Supraglottitis
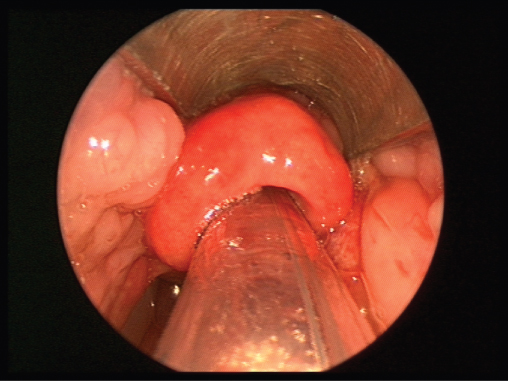
Haemophilus influenzae type B is the usual infective agent, although the incidence has significantly decreased with HiB vaccination. Children between the ages of 2 and 7 years of age are affected, with a peak incidence in 3-year-olds. The disease typically presents with a rapid onset of high fever, toxicity, agitation, stridor, dyspnoea, muffled voice and painful swallowing. Examination will reveal a child seated and leaning forward with the mouth open and drooling. If supraglottitis is suspected, no further examination is recommended outside of a controlled setting. In acute supraglottitis, the risk of complete obstruction is high and the airway has to be secured. Endotracheal intubation is the method of choice as the supraglottic swelling is usually reversible in a few days, unless complications occur. An oedematous, cherry-red epiglottis with inflammation of the surrounding supraglottis is seen on direct laryngoscopy (Figure 18.3). Intravenous antibiotics are required.
Figure 18.3 Laryngoscopic view of oedematous and red epiglottis, with generalised oedema of supraglottic.
Laryngotracheobronchitis
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


