Surgical Management of Thyroid-Associated Orbitopathy
Nicholas J. Schmitt
Randall L. Beatty
John S. Kennerdell
Thyroid-associated orbitopathy (TAO), also known variously as thyroid eye disease, Graves eye disease, or dysthyroid orbitopathy, is the most common specific inflammatory condition affecting the orbit and periorbital tissues. The management of TAO involves both surgical and medical components, the latter of which are covered elsewhere in these volumes. This chapter discusses the surgical management of TAO, which includes the following procedures: orbital decompression, strabismus correction, and correction of eyelid retraction.
TAO is associated with Graves’ thyroid disease and can present at any time in the course of the disease, whether the patient is in a euthyroid, hypothyroid, or hyperthyroid state. The cause of TAO is unknown. In theory, a combination of cell-mediated and humoral activation may promote orbital inflammatory cell migration, edema, and fibrosis. Extraocular muscles are the primary site of inflammation. Orbital fat and eyelid muscles are also commonly involved. Demographically, TAO is most prevalent among middle-aged Caucasian women, though it occurs in all races. It is particularly rare among Asians. Though less often affected, men tend to have a more severe course than women.1
Two phases define TAO: an active, inflammatory phase, and a nonactive, postinflammatory phase. The active, or inflammatory phase is self-limited and usually lasts from 6 months to 5 years. Signs and symptoms include eyelid retraction (particularly lateral flare), dry eye symptoms, periorbital edema, conjunctival chemosis, restrictive strabismus, proptosis, and, more rarely, compressive optic neuropathy. Typically, the signs and symptoms change or progress over weeks to months. Medical management, which includes corneal lubrication, systemic corticosteroids, and orbital radiation, is directed at the active phase of the disease. The nonactive or postinflammatory phase of the disease begins once the signs and symptoms have remained stable for at least 6 months. Sequelae commonly appearing in the nonactive phase include lid retraction, exposure keratopathy, restrictive myopathy and strabismus, exophthalmos, and possibly compressive optic neuropathy; these conditions usually require surgical treatment1 (Fig. 1). In sum, surgical management is generally reserved for the postinflammatory or nonactive phase of the disease, except when vision-threatening disorders (e.g., optic neuropathy or severe exposure keratopathy) are present.
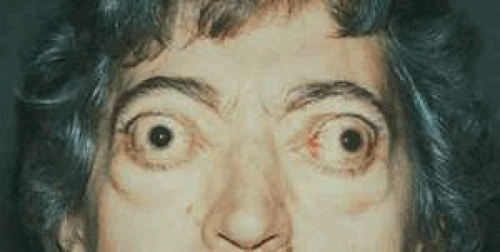 Fig. 1. A 59-year-old woman with severe thyroid-associated orbitopathy, including bilateral optic neuropathy, left lid retraction with corneal exposure, restrictive strabismus, and cosmetic disfigurement. |
SURGICAL EVALUATION
The surgical evaluation of a patient with dysthyroid orbitopathy is critical to proper surgical planning. It begins with a thorough past medical history and history of the presenting illness to determine if the patient is in the active phase of the disease. It is important to ask the patient about symptoms of myasthenia gravis, which is associated with thyroid disease. The physical exam begins with a best-corrected visual acuity, followed by refraction. The pupils and color vision are tested for optic neuropathy. Exophthalmometry is performed to measure proptosis. Eyelid position is examined by measuring the fissure width, the position of the upper and lower lids relative to the limbus, the margin to reflex distance, the amount of levator function, and the presence or absence of lagophthalmos. Schirmer testing is useful for documenting ocular dryness. Ocular motility is assessed and the amount of strabismus, if present, is quantified using prisms in the cardinal positions of gaze. Forced duction testing is useful if a restrictive process is in question. Intraocular pressure is measured in primary and upgaze positions. Formal visual fields are obtained to document optic neuropathy. A dilated funduscopic examination is performed with attention to the optic nerve. Optic nerve edema or pallor suggests apical optic nerve compression and must be correlated with formal visual fields. Orbital computed tomography or magnetic resonance imaging is indicated when compressive optic neuropathy or extraocular muscle enlargement is suspected. Orbital ultrasonography may also be used to evaluate the size of the extraocular muscles. External photographs are taken to document proptosis, lid position, and motility deficits.
Because of the self-limited and variable nature of TAO, surgery to correct disease-related functional abnormalities is carefully timed and individualized. Surgical management of TAO must follow a staged sequence of procedures. Though not all stages are necessary for every patient, orbital decompression is performed first, followed by strabismus correction, and, finally, correction of lid retraction.
ORBITAL DECOMPRESSION
Orbital decompression, if required, is performed first in the surgical staging of TAO. There are several indications for orbital decompression in patients with TAO. These include compressive optic neuropathy, exposure keratopathy due to exophthalmos, orbital pain, elevated intraocular pressure, and cosmesis. Optic nerve compression and subsequent optic neuropathy are caused by rectus muscle swelling at the orbital apex. Even after months of compression, optic neuropathy due to TAO can be reversed by decompressing the orbit.2 Exposure keratopathy from proptosis can be quite severe, occasionally leading to corneal perforation. Orbital decompression can reduce the severity of the proptosis and thus the extent of exposure. TAO can also cause orbital pain, which patients commonly attribute to “sinus disease.” Therefore, such pain is rarely reported unless elicited by direct questioning. Orbital decompression can effectively relieve orbital pain.* Additionally, chronically elevated intraocular pressure from orbital congestion can eventually produce a glaucomatous optic neuropathy, which must be treated by decompressing the orbit. Finally, the psychological devastation from cosmetic disfigurement, due to marked proptosis, can be reduced by orbital decompression.
Orbital decompression in TAO is achieved by removal of orbital bony wall and/or orbital fat. Removing portions of one or more of the bony walls of the orbit expands the volume available to the orbital fat and extraocular muscles. Removal of orbital fat alone is useful when fat hypertrophy, rather than extraocular muscle enlargement, is the major contributor to orbital congestion. The surgical approaches to orbital decompression discussed in this chapter include lateral wall decompression with fat decompression, balanced medial and lateral wall decompression, three-wall decompression (lateral, inferior, and medial wall removal), and four-wall decompression. As more walls are excised, reduction of exophthalmos is enhanced. However, excising more walls also increases morbidity due to strabismus, enophthalmos, and inadvertent damage to intra- and extraorbital structures.
The choice of surgical approach for orbital decompression is made after considering the patient’s findings, including the amount of proptosis, any pre-existing strabismus, and the presence or absence of optic neuropathy. To predict the risk of postoperative strabismus, it is useful to categorize exophthalmos into two clinically distinct types.3 Type I typically presents without restrictive myopathy, and the predominantly affected orbital tissue is fat and connective tissue. These patients may benefit from fat decompression alone.4 In contrast, type II presents with restrictive myopathy and enlarged extraocular muscles and is associated with a significantly higher rate of postoperative strabismus.
* When surgical decompression is not yet indicated, an intraorbital injection of corticosteroid during the active phase of the disease is a viable alternative to systemic corticosteroids for orbital pain and congestion. A suggested dose is triamcinolone acetonide 40 mg (Kenalog-40; Bristol-Myers Squibb Co., Princeton, NJ), injected via a tuberculin syringe with a 26-gauge and 5/8-inch needle in the inferior lateral quadrant of the orbit.
Surgical Technique
The following sections describe in detail the surgical techniques for orbital decompression: (1) lateral wall decompression with fat decompression, (2) balanced medial and lateral wall decompression, (3) three-wall decompression (lateral, inferior, and medial wall removal), and (4) four-wall decompression. All of these procedures require general anesthesia, with the possible exception of fat decompression only, where local anesthesia with intravenous sedation may be sufficient. Dexamethasone phosphate, 8 to 12 mg, and cephazolin, 1 g, are given intravenously at the beginning of surgery to control, respectively, postoperative inflammation and infection.
Lateral Wall Decompression with Fat Removal.
Lateral wall decompression is indicated in patients presenting with mild to moderate proptosis but without optic nerve compression. When combined with intraconal fat removal, lateral orbital wall removal should reduce proptosis by 1 to 3 mm. Of the four types of decompression listed above, lateral wall decompression with fat removal is least often associated with postoperative strabismus.5 However, this procedure does not usually relieve the apical crowding that causes optic neuropathy. Lateral wall plus fat decompression and balanced medial and lateral wall decompressions produce similar amounts of decompression.5
Lateral wall decompression begins with a lateral approach made through a superior lid crease incision, which is extended 1 cm to the lateral orbital rim. Before the incision, the eyelid crease is marked with a marking pen, and, for hemostasis, the area is infiltrated with a local anesthetic solution containing 2% lidocaine and epinephrine in a 1:100,000 dilution. The dissection through the skin is performed with a no. 15 blade. Using small retractors, the orbicularis dissection is carried to the superior and lateral rim. The periorbita is incised and reflected off the lateral orbital wall with a periosteal elevator. To avoid premature perforation of the periorbita, malleable retractors are used to retract the orbital tissues medially. Zygomaticofacial and zygomaticotemporal neurovascular bundles are identified and cauterized to prevent hemorrhage. The superior and inferior orbital fissures are identified as surgical landmarks. The bone sculpting is performed using an irrigated 4-mm egg-shaped cutting burr on an angled, high-speed surgical drill. Next, while preserving the lateral orbital rim, decompression begins as the body of the zygoma and the lateral part of the maxilla are removed to the boundary of the inferior orbital fissure. To avoid excessive bleeding, bone removal is stopped upon reaching the temporalis fascia. Next, the lacrimal fossa of the frontal bone is sculpted to provide space for repositioning of the lacrimal gland, which can actually prolapse outside of the orbital boundary to provide substantial volume expansion.6 Finally, the most substantial and effective decompression occurs with the posterolateral sculpting of the trigonal region of the greater wing of the sphenoid.6,7 This thick, marrow-filled bone lies almost posterior to the globe. In tight, fibrotic orbits, it may be the only area of bone that can effectively reduce proptosis.6 The dura of the middle cranial fossa may be exposed in sculpting of this area of bone. Thus, care is taken to avoid dural perforation and cerebrospinal fluid leakage.7 Using a sickle-shaped blade, the periorbita is opened superiorly and inferiorly to the lateral rectus, allowing orbital fat to prolapse into the spaces created by the bone removal.
After bone removal, attention is turned to inferior orbital fat decompression. First, the inferior crus of the lateral canthal tendon is severed and the conjunctiva incised with scissors along nearly the entire length of the fornix, allowing access to the inferolateral and inferomedial fat pockets. The majority of fat decompression occurs in the inferolateral fat pocket. Often, a total of 6 to 7 cc of fat can be removed from each eye. Fat decompression is performed with careful attention to hemostasis and avoidance of the inferior oblique, lateral, and inferior rectus muscles. The conjunctiva and periosteum can be left unsutured. Finally, the lateral canthal tendon is re-established, a Penrose drain is placed in the lateral orbit, and the skin is closed with 6-0 fast-absorbing suture.
Balanced Medial and Lateral Wall Decompression.
Balanced medial and lateral wall decompression is indicated when both moderate proptosis and optic neuropathy are present. The combination of medial and lateral wall decompression is more effective in treating optic neuropathy than lateral wall decompression alone and produces an additional enophthalmic effect of 2 to 4 mm (Fig. 2). However, it is more often accompanied by postoperative strabismus. Balanced medial and lateral wall decompression with fat removal can be a viable alternative to medial, lateral, and inferior decompression, as fat removal can substitute for inferior wall removal.7 The medial wall can be accessed by either a transcaruncular or an endoscopic approach. For medial wall removal, transnasal endoscopic approach by an otolaryngologist is recommended.
 Fig. 2. A: A 66-year-old woman with a tight and painful right orbit, with associated raised intraocular pressure (29 mm Hg). B: Postoperative appearance after a balanced right orbital decompression. Intraocular pressure of the right eye decreased to 19 mm Hg. |
A balanced medial and lateral wall decompression begins with lateral wall decompression, as described in the previous section. Next, the nasal mucosa is decongested with neurosurgical cottonoids soaked in oxymetazoline HCl 0.05% (Afrin; Schering-Plough Corporation, Kenilworth, NJ) and lidocaine 4%. Using an endoscope, a septoplasty is performed as needed for visualization of the middle meatus. The uncinectomy follows. The ethmoidal bullae are opened, all ethmoidal air cells are removed, and the anterior wall of the sphenoid sinus is excised, thus exposing the skull base and lamina papyracea. The natural opening of the maxillary sinus is then enlarged in a posterior-superior fashion to prevent postoperative obstructive maxillary sinusitis. After the sphenoethmoidectomy, the lamina papyracea is removed, using care to avoid premature opening of the periorbita. Bone removal is extended to the ethmoid roof superiorly, the orbital apex posteriorly, the medial orbital strut inferiorly, and the frontal process of the maxilla anteriorly. To induce herniation of the orbital contents, multiple full-thickness periorbital incisions using a sickle-shaped blade are made in a posterior to anterior fashion.7,8 A moustache dressing is used for nasal drainage.
Three-Wall Decompression (Lateral, Inferior, Medial Wall Removal).
As compared to balanced medial and lateral wall decompression, the combination of lateral, medial, and inferior orbital decompression enables the surgeon to improve the enophthalmic effect to 6 to 10 mm (Fig. 3). Removal of the floor produces an additional enophthalmic effect of 3 to 5 mm. Floor removal is associated with worsening of strabismus. Numbness or paresthesia in the distribution of the infraorbital nerve may also present and usually resolves after several months. Thus, an attempt is made to avoid disturbing the inferior neurovascular bundle. The preservation of a maxilloethmoidal strut during inferomedial decompressions is advocated to minimize globe dystopia and postoperative strabismus.9
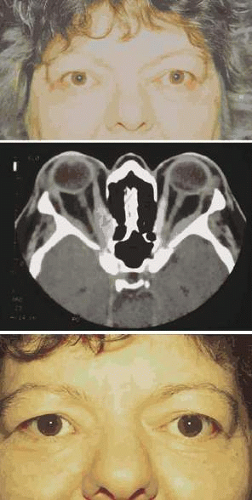 Fig. 3. A: A 48-year-old woman with bilateral, thyroid-associated compressive optic neuropathy. Visual acuity was 20/80 in the right eye (OD) and 20/30 in the left (OS). Color vision by Ishihara color plates was 1/12 OD and 10/12 OS. Goldmann visual fields revealed central scotomas in both eyes. Hertel exophthalmometry measurements were 25 mm OD and 24 mm OS. B: Preoperative axial computed tomography scans showing apical crowding and proptosis. C: Postoperative appearance after bilateral, three wall orbital decompression. Visual acuity improved to 20/30 OD and 20/20 OS. Ishihara color plates improved to 7/12 OD and 12/12 OS. Goldmann visual field showed only an enlarged blind spot OD, normal OS. Hertel exophthalmometry measurements improved to 19 mm OD and 18 mm OS.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|