Surgical management of stapes fixation is well defined for otosclerosis and congenital stapes fixation, with respectable results.1,2 However, the management of stapes fixation in chronic ear disease is more challenging, with far less predictable results. Whereas some surgeons find chronic ear disease a possible contraindication to ossiculoplasty in cases of stapes fixation, others believe that significant benefit can be achieved with surgery.3,4,5
The basic principles of treatment are restoration of footplate mobility or labyrinthine fenestration. Mobilization of the stapes is generally considered the first option and remains the technique of choice for several otologists.3,5 If mobilization fails to improve hearing, some are reluctant to open the labyrinth because of the risk of inner ear damage6 and propose a hearing aid instead. Still others choose labyrinthine fenestration as salvage surgery after insufficient mobilization attempts3,5,7 or as a primary technique,4,8,9 claiming that mobilization itself carries the same risks for the inner ear.
31.2 Patient Selection
The risks and benefits should be evaluated for each patient and depend on the underlying pathology, the estimated progression of the middle ear disease, the surgeon’s experience, and the patient’s expectations. All ossiculoplasty attempts have to be balanced against the benefits of conventional or implantable hearing aids. Continuous improvements in bone-conducting hearing devices and new methods for coupling active middle ear implants onto the round window membrane, even in case of stapes fixation, further compete with risky ossiculoplasties.
31.3 Causes of Stapes Fixation in Chronic Ear Disease
In chronic ear disease, there exist three main causes of stapes fixation. The most frequent etiology is tympanosclerosis, which was first reported by Zöllner in 1956.10 In 1873 von Trölsch already described the characteristics of tympanic cavity sclerosis, named “Paukensklerose,” which was further identified as a long-term sequela of chronic middle ear infections, with calcareous deposits within the tympanic membrane (myringosclerosis), tympanic cavity, and ossicular chain. In 1977, Shea reviewed his 1502 surgeries for chronic otitis media (COM) and found an incidence of stapes fixation in 112 patients, or 7.5% overall.11 Within this subgroup, 62% were due to tympanosclerosis. In general tympanosclerosis affected 5% of his COM patients. The incidence of tympanosclerosis varies greatly (between 11% and 32%12,13), and not all patients present with stapes fixation. Such an oval window involvement was estimated by some authors to occur in 35% of patients with tympanosclerosis.14 Since tympanoclerosis is an “end-stage” disease, the ear is usually dry and the non-affected mucosa can be quite healthy. Involvement of the tympanic cavity and the ossicles typically leads to severe hearing loss with an air-bone gap (ABG) of 40 dB or more.
Shea described another cause of stapes fixation, which he termed “postinflammatory osteogenic fixation.”11 Analyzing his 1502 middle ear surgeries for COM, he found 19 cases (1.2% overall) with a rigid stapes fixation as a consequence of chronic ear disease. He proposed that this was due to a new membranous bone growth along the stapediovestibular joint caused by an inflammatory reaction from either infection or trauma from vigorous footplate manipulation during previous surgeries. The ABGs ranged from 10–50 dB. Typically 80% of his patients had undergone previous middle ear surgery to correct the underlying suppurative otitis media.
Rarely, stapes fixation existing with COM can also be caused by concomitant otosclerosis or other occasional entities (Paget‘s disease, osteogenesis imperfecta, fibrous dysplasia, systemic inflammatory disease).
31.4 Preoperative Reflections: The Triple “A”
When facing a fixed stapes in chronic ear disease, and before choosing the surgical strategies, the following three factors should be taken into account.
31.4.1 Anticipation
Preoperative computed tomography (CT) scans infrequently detect stapes fixations; however, they do highlight the degree of pneumatization and ventilation of the middle ear and mastoid, and therefore provide an overall view of the middle ear pathology. That being said, neither CT scans nor the audiogram patterns can predict with reasonable sensitivity the non-otosclerotic fixation of the stapes. In case of previous surgery, an effort should be made to obtain the operating note of the previous surgeon, verifying the mobility of the stapes. However, one must keep in mind that concurrent granulation tissue at the time of first surgery may not allow proper assessment of stapes mobility, that partial fixation is even more difficult to evaluate, and that any progression of the middle ear disease may impair the footplate mobility after previous surgeries. Careful preoperative evaluation should anticipate the intraoperative findings and help in the planning of the surgical options.
31.4.2 Audible Range and Status of the Middle Ear
As in any ossiculoplasty, the condition of the ipsilateral hearing ear (type and degree of mixed hearing loss, speech discrimination score, high-frequency sensorineural impairment) and the condition of the contralateral ear determine how to estimate the benefit for the patient overall. In case of large asymmetry with poor cochlear reserve on the affected ear, surgery should be avoided. This is best anticipated by the Belfast rule of thumb: patients are likely to benefit from surgery if the air conduction threshold within the speech frequencies (500–4000 Hz) will be ≤30 dB or if the interaural difference is reduced to ≤15 dB.15 The final result should also be plotted on the Glasgow Benefit Plot to account for bilateral hearing benefit.16 In case these audiological goals cannot be anticipated, alternative methods may be more justified.
Equally important is the status of the middle ear: the presence of an acute infection at the time of stapes surgery increases the risk of sensorineural hearing loss.17 Interestingly, pseudomonas infections harbor a much greater risk than other pathogens, such as Haemophilus or Streptococcus pneumoniae, at least in the animal model.18 It seems safe to carry out a stapedotomy or malleostapedotomy in the setting of inactive or previously treated COM with an intact tympanic membrane.19,20
In summary, before planning any labyrinthine fenestration in COM, the middle ear must be dry and the eardrum closed. As the majority of patients in chronic ear disease (85% in a series of 775 patients by Asiri, Hasham, al Anazy, Zakzouk, and Banjar12) may still present with a tympanic membrane perforation, the fenestration should be performed in a second stage. Concomitant round window involvement with tympanoslerotic obliteration further reduces the chance of hearing improvement.
The status of the remaining ossicular chain and the type of previous or planned surgery is equally important: at least the presence of a mobile malleus in proper contact to the drum allows coupling of a prosthesis for reconstruction. If incus and malleus are absent, staged reconstructions with a neo-malleus and, later, a neo-malleus-vestibulopexy (malleostapedotomy) assembly may become an option. This may be further challenged by an open or closed cavity setting.
Many surgeons choose to avoid labyrinthine fenestration procedures in the background of poor Eustachian tube function because of concern related to subsequent prosthesis migration. Furthermore, in the absence of satisfactory middle ear ventilation, even the most well-conceived ossicular reconstruction is doomed to result in at least a 35–40 dB ABG.21 With poor ventilation neither mobilization nor labyrinthine fenestration will provide good results. In all these instances, alternative methods should be proposed.
31.4.3 Alternatives
Conventional hearing aid amplifications are always an alternative in dry external ear canals with an intact drum, either in a closed or open cavity setting. Contralateral Routing of Offside Signaling (CROS) and Bilateral-CROS hearing aids, for use in cases of severe mixed and asymmetric hearing loss, have regained popularity since the reintroduction of wireless communication between the processors. The major competitors to ossiculoplasty remain the fitting of bone-anchored hearing devices or active middle ear implants coupled to the round window or to a cochleostomy/vestibulopexy approach.
31.5 Surgical Technique
Preconditions required to perform an ossiculoplasty are:
Sterile middle ear cavity with an intact and healthy eardrum in a favorable position.
Adequate ventilation of the middle ear space on long term.
The presence of a malleus or reconstruction of a neo-malleus for prosthesis fixation is advisable.
Expected outcome within the Belfast rule of thumb.
Alternative hearing aids or implants have been discussed with the patient.
Long-term follow-up (at least 5 years) is feasible, allowing surgeons to evaluate their own results and to improve their personal skills.
When the above conditions are filled, two main strategies are then available: stapes mobilization or labyrinthine fenestration. Most surgeons agree that stapes mobilization does not attempt to “rock” the stapes free, but, rather, to remove sclerotic plaques from the oval window niche using cold instruments (needle, hook, drill) and/or laser technology (Argon, KTP, Diode, or CO2 laser systems). Rocking the stapes superstructure or the footplate itself may lead to fractures or refixation. Labyrinthine fenestration procedures include stapedectomy, stapedotomy, and lateral canal or vestibulum fenestration techniques. This situation is classified as Austin-Kartush Group F (see Chapter 1), or Fisch Class II2 or III3.22,23
31.5.1 Fixed but Intact Ossicular Chain
In case of tympanosclerosis with an intact ossicular chain, a primary attempt should be made to remove the plaques from the stapes arch and footplate in a posterior-anterior direction, allowing the stapes tendon to stabilize the footplate during dissection. Although controversial, we advise disconnecting the incudostapedial joint first to correctly assess the mobility of the incus/malleus complex and the stapes as separate entities. This approach also allows safer access to the oval window niche. Facial nerve monitoring is advisable since the plaques could cover a dehiscent facial nerve, and even careful removal with cold instruments or lasers may induce a facial nerve lesion. In case of additional incus and/or malleus fixation, mobilization of these other ossicles becomes part of the procedure, and incus interposition or prosthesis insertions may become necessary. A final ABG within 20 dB should be achieved in 60% to 80% of patients, and >50% may even end up within 10 dB in cases of a previous intact ossicular chain.
In case of insufficient results or re-fixation of the ossicles, a fenestration procedure remains a good second-stage alternative.5 The technique is described below. Others prefer not to attempt a stapes mobilization as a first option but to proceed with an incus- or malleus-stapedotomy/stapedectomy procedure as their preferred choice.4,8 In favor of a primary fenestration option is the fact that an intact ossicular chain is in the proper anatomic position and, therefore, favorable for the fixation of a piston perpendicular to the footplate.
31.5.2 Fixed Footplate and Incomplete Ossicular Chain
In case of a “fixed footplate–only” situation without a stapes superstructure, or in case of postinflammatory osteogenic fixation of the annular ligament without obvious tympanosclerotic plaques, footplate mobilization is not advisable. Even in cases of an intact superstructure but fixed footplate, any attempt to achieve a tympanoplasty Type III (open cavity setting) or any effort to place a partial ossicular replacement prosthesis (PORP) between the eardrum and the stapes will not provide any benefit. We found only 8 patients in our database of over 5000 files with such attempts. The postoperative hearing remained, as expected, unchanged. There was also no change in bone conduction. Tos, Lau, Arndal, and Plate also stated that any columella reconstruction inserted between a fixed footplate and the tympanic membrane revealed only unfavorable results, with hearing thresholds exceeding 40 dB.3 Therefore, only a labyrinthine fenestration procedure may benefit these patients. There are two types of labyrinthine fenestrations, described below.
Malleostapedotomy or Staged Neo-malleus plus Neo-malleostapedotomy
In case of subtotal or total fixation of the stapes footplate, any reconstruction aims at connecting the sound conduction from the drum to the vestibule, necessitating the opening of the footplate. The stapes superstructure is not helpful and needs to be removed, leading to the Fisch Class III3 or Austin-Kartush Type F basic situation.22,23 These are all staged surgeries in a healthy middle ear environment. A calibrated opening into the stapes footplate is preferred over total stapedectomy to reduce the risk of inner ear damage.24 In case of obliterative tympanosclerosis, a drill must be used to blueline the vestibule before entering. Once the blueline has been reached, the length of the piston is measured, the angulation determined, and the piston prepared to fit perfectly. Next, the stapedotomy opening is completed and the piston introduced 0.5 mm into the vestibule and crimped to the malleus shaft just distal to the short process (▶ Fig. 31.1). The opening can be sealed using soft tissue and the patient’s own blood. Even in the presence of an incus, we prefer to remove the incus to gain better access to the fixed and often obliterated footplate. Our results in 17 patients with malleostapedotomy verify a success rate of 18% of patients with an ABG ≤10 dB, 71% ≤20 dB, and only 1 patient with an ABG of more than 30 dB (▶ Table 31.1). These results are inferior to the overall results of malleostapedotomy in otosclerosis patients, indicating the less favorable middle ear condition in COM patients.25
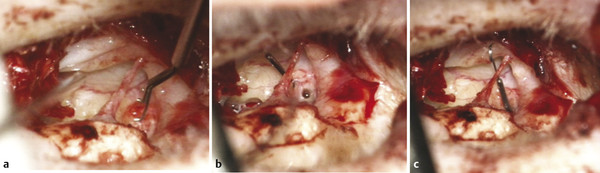
Fig. 31.1 Malleostapedotomy. (a) The length of the piston is measured. (b) Stapedotomy performed with a drill. (c) Introduction of the piston crimped to the malleus.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


