 Surgical Management of Orbital Tumors
Surgical Management of Orbital TumorsSurgical Management of Orbital Tumor
The details of surgical approaches to orbital tumors and pseudotumors are discussed elsewhere (1,2). Enucleation is discussed in the Atlas of Intraocular Tumors and is not covered here. Illustrated and briefly described here are the indications and techniques of orbital fine-needle aspiration biopsy (FNAB), conjunctival approach, cutaneous approaches, and orbital exenteration (3,4,5). In general, well-circumscribed tumors should be managed with excisional biopsy; poorly circumscribed, diffuse tumors are best managed by incisional biopsy. The diagnostic method chosen depends largely on orbital imaging studies and varies with the size and location of the lesion and the suspected diagnosis. Local anesthesia can be used for most FNAB and for very anterior relative small orbital lesions. For larger lesions in the midportion or posterior portion of the orbit, general anesthesia is generally preferable.
Fine-Needle Aspiration Biopsy
FNAB is a useful method for obtaining a diagnosis in selected cases (1,3). It is used most often to confirm the diagnosis of orbital lymphoma or metastasis in a patient who has known systemic lymphoma or a primary neoplasm. If lymphoma or metastasis are suspected and there is no known systemic malignancy, incisional or excisional biopsy usually should be done to provide more tissue for histopathologic study. FNAB should generally not be used for circumscribed orbital tumors in which complete excision is anticipated. Cases where FNAB is indicated have been illustrated throughout this atlas.
There are different methods of performing FNAB for orbital tumors. A pistol grip instrument (Asper-gun) can be used with a 25 or 22 gauge needle. If the orbital lesion is palpable through the skin, the needle can be placed directly into the mass and aspiration done to draw tumor cells into the needle bore. Orbital FNAB can also be performed by a similar technique that is used frequently for intraocular tumors. By this method, a similar needle is attached to a plastic connector tubing about 25 mm long, which is in turn attached to a 10-cc syringe. The needle is guided into the lesion and aspiration is performed to draw tumor cells into the needle bore.
Once the tumor cells are in the syringe, there are two methods of placing the cells onto a slide for cytopathologic stains. One is to use a syringe to express the cells immediately onto the slide and spread them with another glass slide to facilitate staining. The second method, which our cytopathologists prefer, is to immediately place the needle into a small bottle of normal saline and to aspirate it immediately into a syringe. This flushes the cells in the needle bore into the saline solution. The syringe is then submitted immediately for preparation for cytopathologic studies. The solution is placed in special preservative and centrifugation with a millipore filter technique is done to allow a better distribution of the cells for cytopathologic study.
Conjunctival Approach
A conjunctival approach is frequently the best method for selected anterior orbital tumors. It usually requires less surgical time and avoids performing a skin incision and suture removal. The authors use it more frequently for circumscribed anterior orbital tumors that are most likely benign, like cavernous hemangioma, schwannoma, and soft tissue dermoid cysts. An incision is generally made in the conjunctival fornix and Tenon’s fascia is separated by spreading with scissors. Two or three rectus muscles are isolated with nylon sutures for rotation of the globe. Blunt dissection with scissors and cotton-tipped applicator sticks is done until the tumor is exposed and an attempt is made to remove the tumor intact (excisional biopsy) when possible. In using the conjunctival approach inferotemporally, the surgeon should identify the inferior oblique muscle and isolate it with a rubber drain. For superotemporal lesions, the superior oblique muscle must be identified and protected from damage. In the case of an anterior nasal lesion, a transcaruncular approach with a vertical incision can provide good exposure. The tumor can be removed primarily or with assistance of a cryoprobe to facilitate removal. When the tumor has been removed, the conjunctiva is closed with running 7-0 absorbable sutures, antibiotic or corticosteroid ointment is applied, and a patch is placed on the eye until the next day at which time the patient undergoes an office examination with visual acuity, pupil evaluation, and motility check.
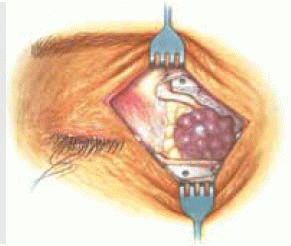
Cutaneous Approach
A cutaneous approach, which provides some what better surgical exposure, is generally preferred for larger, more posteriorly located tumors and for tumors that involve the orbital lobe of the lacrimal gland. Depending on the location and size of the lesion as determined by axial and coronal imaging studies, the incision should be made superotemporally, superonasally, inferotemporally, inferonasally, or directly nasally. A subcutaneous injection of local anesthesia combined with epinephrine along the incision line is performed to achieve better hemostasis. Transconjunctival 4-0 silk bridal sutures can be used to isolate rectus muscles in the quadrants of the tumor, so that they can be continuously identified during the procedure.
Once the skin incision in done, either a transeptal or transperiosteal entry into the orbit can be used, also depending on the imaging and surgical findings. Blunt dissection should be employed as much as possible in the orbital soft tissues. With a transeptal approach, the lesion can be approached directly by gently separating the orbital fat and identifying nearby extraocular muscles and retracting them with sutures or rubber drains. The tumor can be removed directly or with assistance of a cryoprobe.
With the extraperiosteal approach, the skin incision is carried down to the periosteum about 3 mm outside the orbital rim. A periosteal elevator is used to separate the periosteum from the orbital bone and this separation is carried as far posterior as necessary in the orbit. This approach minimizes bleeding and prevents premature exposure of the orbital fat. The periosteum is then separated with scissors and the orbital fat is exposed in the area of the tumor. The tumor
is then removed by methods described under the conjunctival approach. When hemostasis is attained, the subcutaneous tissues and skin can be closed with the surgeon’s choice of sutures. We generally prefer 5-0 absorbable sutures for both. Antibiotic or corticosteroid ointment is applied to the wound and a patch is placed on the eye until the next day, at which time the patient undergoes an office examination with visual acuity, pupil evaluation, and motility check.
is then removed by methods described under the conjunctival approach. When hemostasis is attained, the subcutaneous tissues and skin can be closed with the surgeon’s choice of sutures. We generally prefer 5-0 absorbable sutures for both. Antibiotic or corticosteroid ointment is applied to the wound and a patch is placed on the eye until the next day, at which time the patient undergoes an office examination with visual acuity, pupil evaluation, and motility check.
Regardless of the surgical approach, it is best to remove most tumors entirely if that can be achieved without much damage to vital structures like the extraocular muscles and optic nerve. In the case of a noncircumscribed or very large tumor, it may be necessary to remove the lesion piecemeal. If the diagnosis is uncertain and there is residual tumor in the orbit, a diagnostic frozen section can be performed to determine whether to remove more of the tumor before terminating the procedure. In the case of radiosensitive malignant tumors like lymphoma and metastasis, it may not be necessary to remove the entire tumor. In the case of nonradiosensitive malignant tumors, further attempts can be made to excision all of the tumor if possible.
Orbital Exenteration
Orbital exenteration is used for massive orbital extension of uveal melanoma, orbital extension of primary eyelid and conjunctival malignancies, and certain primary orbital malignancies. When possible, an eyelid-sparing technique should be employed (4,5). After general anesthesia is administered, an outline of the planned skin incision is made with a sterile marking pencil for 360 degrees. If the eyelids are to be sacrificed because of tumor involvement, the line is drawn outside the eyelids but inside the eyebrow superiorly. If the eyelid skin is to be preserved, the 360-degree line is drawn just outside the cilia.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


