Surgery to Correct Cyclotropia
Anya A. Johansen
Donny W. Suh
David L. Guyton
Ocular torsion is rotation of the eye about its anterior-posterior axis. Cyclodeviations are relatively common in patients with strabismus. Approximately a quarter of patients (24%) with diplopia also show a torsional contribution to the diplopia on subjective testing.1 Despite the high incidence of cyclodeviations, rarely are they symptomatic and of clinical concern. The reasons for cyclodeviations being asymptomatic are multiple with some being more intuitive than others. First, humans can use both sensory and motor cyclofusion to fuse up to 5 to 10 degrees of cyclodisparity (Table 1). Second, sensorial adaptation can occur via image suppression, anomalous retinal correspondence, or head tilt.2 Third, infants and children can develop re-orientation of the retinal meridians at the cortical level.3 Additionally, large horizontal or vertical deviations can interfere with a patient’s ability to recognize torsion. Last, and the least understood, is psychological adaptation that can occur in adults.
Table 1. Patient Awareness of the Presence of a Cyclodeviation Relative to the Degree of Torsion as Measured by Double Maddox Rods | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||
Cyclodeviations are most commonly caused by an imbalance between the muscles that intort the eye (superior oblique and superior rectus) and the muscles that extort the eye (inferior oblique and inferior rectus). The abnormalities associated with cyclodeviations are diverse and include: cyclovertical muscle paralysis, particularly superior oblique paresis; A- and V-pattern strabismus;4,5 craniofacial developmental anomalies; iatrogenic conditions from previous surgeries, mostly strabismus surgeries; and restrictive deviations, including thyroid ophthalmopathy and nondysthyroid restrictive ophthalmopathy.
Ocular torsion is not only an important phenomenon in the evaluation of strabismus, but also in refractive surgery and macular translocation surgery. Correction of astigmatism with laser in situ keratomileusis (LASIK) has become increasingly more precise, and yet results have not been any more satisfactory. Only recently has it become evident that a change in ocular torsion of 2 to 4 degrees can occur as a patient changes from a seated to a supine position, rotating the axis of astigmatism.6,7 By marking the limbus prior to taking the corneal measurements, the refractive surgeon can adequately monitor ocular torsion and correct for it during laser ablation.8 Macular translocation is a newer surgical technique used to relocate the macula over healthy retinal pigment epithelium in patients with age-related macular degeneration. This procedure is known to produce high degrees of effective ocular torsion and will be discussed briefly under indications for surgical correction.
Assessment of Cyclodeviations
Both subjective and objective cyclodeviations must be assessed for proper clinical analysis and management. Commonly used tests for measuring subjective torsion include the double Maddox rod test and the Lancaster red-green test. The double Maddox rod test uses specially constructed parallel cylinders that convert a point of light into a streak of light oriented perpendicular to the direction of the parallel cylinders. A Maddox rod lens is placed in front of each of the patient’s eyes with the cylinders oriented vertically, and, looking at a point light source, the patient sees two roughly horizontal lines. The patient is instructed to rotate each Maddox rod lens until the two lines are horizontal and parallel with each other. The amount of subjective torsion is the difference between the final positions of the Maddox rod lenses. Classically a red Maddox rod is placed before the right eye, and a white Maddox rod is placed before the left eye, but recent studies have shown less error when the same color Maddox rods are used before both eyes, preferably red.10 Double Maddox rod testing is easily performed, and measures both cyclotropia and cyclophoria by disrupting fusion. Limitations of the test are that environmental clues can allow sensory cyclofusion and the test is difficult to perform reliably in directions other than primary gaze.
Our preferred method of testing for subjective torsion is the Lancaster red-green test11 (Fig. 1). This test allows the clinician to evaluate torsion in nine positions of gaze and clearly indicates where torsion is greatest and where vertical deviation is most significant. The test is performed in a darkened room so that no spatial clues in the environment can help in orienting the streaks of red and green light. By convention, a red filter is placed over the right eye and a green filter over the left. The examiner takes the colored light (red or green) corresponding to the desired “fixing eye” and shines it on the wall successively in the nine diagnostic positions of gaze. In each position, the patient is asked whether the vertical streak of light is straight or tilted. If the streak is tilted, the examiner adjusts the light until the patient sees the streak exactly vertically. The patient then shines the second colored light to superimpose the second streak on the first streak. The examiner records the position and orientation of the streaks to analyze the torsional and vertical components of the deviation in the different fields of gaze (Fig. 2). The Lancaster red-green test can easily be performed in the nine diagnostic positions of gaze and helps to establish the pattern of torsional deviation. The limitation of the Lancaster red-green test is that the actual amount of torsion is difficult to measure numerically. Also, the absolute horizontal deviation is difficult to judge with this test because of the poor control of accommodation provided by the streaks of colored light. The relative amounts of horizontal deviation, however, are reasonably reliable, and are used for judging A- or V- patterns.
 Figure 1. Performance of the Lancaster red-green test. |
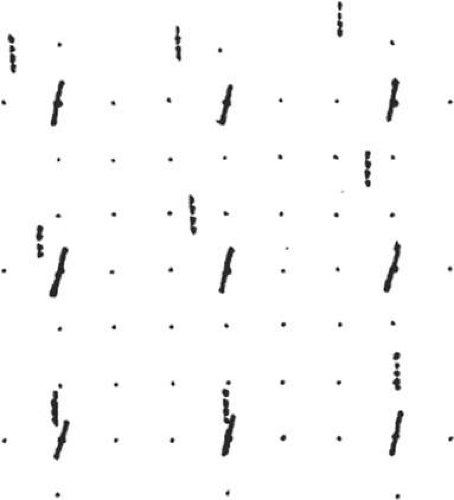 Figure 2. Lancaster red-green plot of a patient with a left superior oblique paresis. The solid line (red streak) is the projection of the subjective vertical meridian of the right, fixing eye, and the dotted line (green streak) represents the left eye. Subjective extorsion appears in both eyes and a small V-pattern exotropia is present. The left hyperdeviation is greatest in upgaze and to the right. |
Other less commonly used methods of subjectively testing cyclodeviations are the Bagolini striated glasses test and the synoptophore method. The Bagolini striated glasses are two streaked lenses with the striations in the lenses causing a fixation light to appear as a streak of light. Similar to the Maddox rod test, the lenses can be rotated until the two streaks appear parallel. The Bagolini lenses permit a nearly normal view of the visual environment while the patient is fixing on the streaks of light, allowing cyclofusion. Thus, the Bagolini lenses can only measure subjective cyclotropia, not cyclophoria.
The synoptophore (major amblyoscope) method involves two dissimilar images being visualized by each eye. The patient adjusts the images until they are superimposed. To better measure cyclodeviations, the dissimilar images used are a black circle with hash marks (similar to a clock face), and black perpendicular crossbars. Once the images are centered, the degree of cyclodeviation is measured by the patient reading off the degree mark where the vertical or horizontal line of the cross intersects the black circle. Using this method, it has been found that while measuring cyclodeviations, the horizontal line of the cross usually indicates more cyclodeviation, as there is less sensory cyclofusion for horizontal meridians.12 The drawback of the synoptophore is that it is not readily available in most clinical practices, and it only works well in primary gaze.
Objective torsion is best assessed by indirect ophthalmoscopy or fundus photography.5,13 Although the double Maddox rod and Lancaster red-green tests are good for measuring subjective torsion, they are difficult for children to perform accurately and are also difficult to use for patients with large horizontal or vertical deviations. Anatomically, the normal position of the fovea in reference to the optic disc is within the lower third of the optic disc, which equals a 9-degree range.5 When evaluating objective torsion with an indirect ophthalmoscope, it is important to remember that the patient should be looking in primary position and that because the view is inverted and reversed, the fovea should be located within the upper third of the disc. If the fovea is higher than the optic disc, the eye is extorted; if the fovea is lower than the upper third of the optic disc, the eye is intorted. While performing surgery for ocular torsion, the indirect ophthalmoscope can be used intra-operatively to evaluate the amount of correction achieved. Ocular torsion can also be documented using fundus photos.
Indications for Surgical Correction
Cyclotropia, if symptomatic, cannot be corrected with prisms but requires surgical correction. As discussed previously, the underlying etiologies of cyclodeviations are diverse, with a few of the more commonly encountered and/or more complex situations discussed later.
Superior oblique palsy is the most common type of vertical paralytic strabismus. Scott and Kraft reported that 29% of superior oblique palsies are bilateral.14 These bilateral cases are invariably associated with excyclotropia that frequently goes unrecognized. The constellation of findings in bilateral superior oblique paresis are (1) left hyperdeviation worse on right gaze, (2) right hyperdeviation worse on left gaze, (3) right hyperdeviation worse on right head tilt, (4) left hyperdeviation worse on left head tilt, (5) a V-pattern strabismus, and (6) excyclodeviation that often exceeds 15 degrees in primary gaze and increases in downgaze. The goal of treatment in these cases is to correct the symptomatic cyclotropia without producing a significant vertical deviation. For bilateral symmetric cases, the Harada-Ito procedure is the surgery of choice. If the bilateral superior oblique palsy is asymmetric, surgical correction can involve performing a judicious superior oblique tuck in an attempt to improve the action of the superior oblique muscle without causing a significant Brown’s syndrome.
Unilateral superior oblique palsy has less excyclotropia and more vertical deviation, and is thus corrected using different surgical methods. In a case of traumatic superior oblique palsy, there can be marked improvement or disappearance of the vertical component over time, with persistence of the torsional component; therefore there should be a minimum waiting period of 6 months between onset and surgical treatment.15,16 Because of the tendency of the vertical deviation to improve with time, there are a number of cases of unilateral superior oblique palsy that have primarily an excyclotropia without significant vertical deviation. These patients are treated with a Harada-Ito procedure or a modification thereof, which will be discussed further under the surgical procedures section. In a patient with unilateral superior oblique paresis and extorsion with significant “over-action” of the inferior oblique muscle, an inferior oblique weakening procedure is indicated to improve both the torsional and vertical components. Alternatively a tuck of the paretic superior oblique tendon may be used, but this runs the risk of causing a post-operative Brown’s syndrome. Contralateral inferior rectus recession also reduces, although to a lesser extent, the relative extorsion between the two eyes. The vertical deviation is occasionally worse with the paretic eye in adduction and depression, a pattern dubbed the “inverted Brown pattern.” In this case it has recently been reported that weakening of the ipsilateral inferior oblique muscle gives a better long-term result then weakening of the contralateral inferior rectus muscle.17 It is clearly important to measure the torsion in multiple fields of gaze to best develop a surgical plan that corrects the complex vertical and torsional deviations associated with oblique muscle palsies.
A- and V-pattern strabismus has been recognized as a common occurrence requiring different surgical correction than when operating for straightforward exotropia or esotropia. Many surgeons prefer to weaken the inferior or superior oblique muscles if the obliques show evidence of overaction. If there is no evidence of oblique muscle overaction, then a symmetric vertical displacement of the horizontal muscles, or a horizontal displacement of the vertical muscles, can be performed (Fig. 3). The horizontal displacement of the vertical muscles approach has been found less satisfactory.18 It is important to note that in some situations, alternative approaches to surgical correction can have very different effects on the torsional deviation, and these effects should be considered when weighing the value of the alternative approaches. For example, if a patient presents with V-pattern strabismus but no fundus extorsion, the surgeon might choose to avoid oblique surgery and instead perform vertical transposition of the horizontal rectus muscles. However, if fundus extorsion is noted, transposing the medial rectus muscles downward or the lateral rectus muscles upward theoretically makes the extorsion worse, although Metz documented only small, nonsignificant changes in subjective torsion in similar cases.18 If a patient with superior oblique paresis undergoes recession of the ipsilateral superior rectus muscle, extorsion worsens. Simultaneous temporal transposition of this muscle may help lessen the extorsional effect.
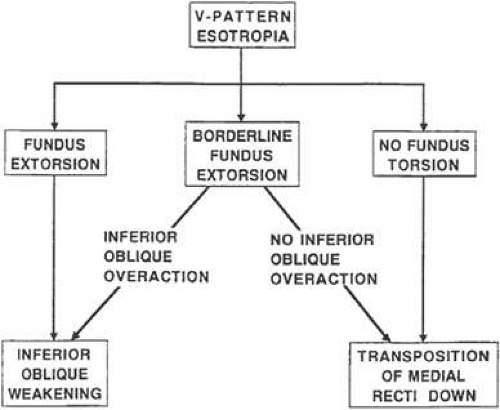 Figure 3. Contribution of fundus torsion to the surgical approach for V-pattern esotropia. |
Fundus intorsion is characteristic of most cases of Brown’s syndrome. Brown’s syndrome responds to superior oblique weakening, which simultaneously decreases the intorsion. In mild to moderate cases of Brown’s syndrome, however, there may not be abnormal fundus torsion in primary position, and intorsion appears only in attempted upgaze in abduction. This suggests that the tendon of the relaxed superior oblique muscle cannot slip forward through the trochlea. If a complete superior oblique tenotomy is performed in this case, extorsion in primary gaze will result. Therefore, a controlled superior oblique lengthening procedure is preferred, which may be adjustable either intraoperatively19 or postoperatively.20
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


