Chapter 15 Surgery of Acute Infections and Their Complications
DEFINITION AND CLINICAL SIGNIFICANCE
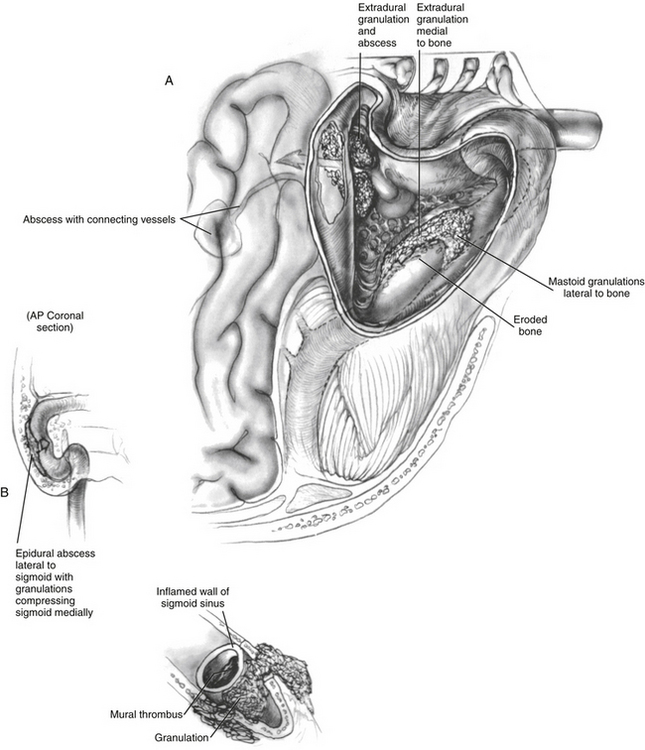
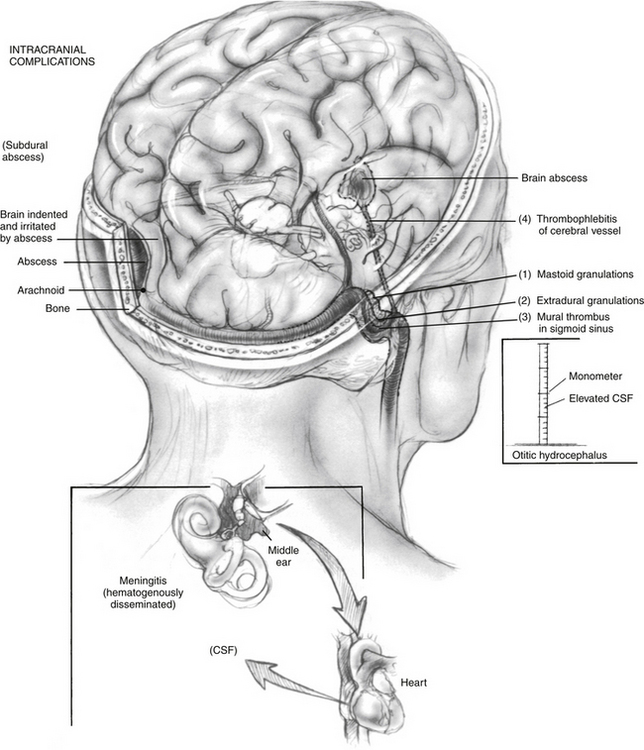
Complications of acute or chronic suppurative ear disease manifest acutely and are medical and surgical emergencies. These complications are defined as a spread of infection beyond the confines of the pneumatized spaces of the temporal bone and the attendant mucosa. Complications are classified into two groups: aural (intratemporal) and intracranial. Aural complications include (1) mastoiditis, (2) petrositis, (3) labyrinthitis, and (4) facial paralysis. Intracranial complications include (1) extradural abscess or granulation tissue, (2) dural venous sinus thrombophlebitis, (3) brain abscess, (4) otitic hydrocephalus, (5) subdural abscess, and (6) meningitis (Fig. 15-1).1
Because of the significant reduction in absolute numbers of complications, individual clinicians do not have extensive experience in treating patients with complications of suppurative ear disease. This limited experience contributes to decreased familiarity and recognition of otogenic complications.2,3 The combination of lack of awareness and masking of early signs and symptoms leads to delay in diagnosis and subsequent treatment. Physician delay has been noted to be the most significant factor in late diagnosis and treatment of otogenic complications. Delay in diagnosis and treatment of complications of suppurative ear disease is associated with worsening morbidity and mortality.2,4
ETIOLOGY AND PATHOGENESIS
The organisms responsible for otogenic complications in the acute setting are Streptococcus pneumoniae, Streptococcus pyogenes, Staphylococcus aureus, and Haemophilus influenzae.5 Organisms that cause complications in chronic otitis media are frequently gram-negative or anaerobic, or both; the presence of anaerobes is significantly associated with complications.6–9 Pseudomonas aeruginosa, Enterobacteriaceae, S. aureus, and anaerobic bacteria are most common in chronic mastoiditis; anaerobes tend to predominate in chronic mastoiditis when techniques allow their discovery.5
In patients with infratemporal complications, isolates from cultures of middle ear effusions, otorrhea, and mastoid have shown S. pneumoniae to be the most common organism,10 followed by P. aeruginosa, S. pyogenes,11 S. aureus, and H. influenzae.12,13 P. aeruginosa was the most common organism found in a review of 134 patients with acute mastoiditis.14
S. pneumoniae15 and H. influenzae type B are the most common causes of bacterial meningitis.16 Proteus mirabilis, P. aeruginosa, and staphylococcal organisms are common pathogens isolated in patients with intracranial complications.17 Gram-negative isolates have been major organisms in other series.18,19 Polymicrobial cultures are common in brain abscess.8
These studies are important for a general reference; however, organisms change over time, and culture-specific treatment is important, as illustrated by the fact that a more recent study determined that methicillin-resistant S. aureus was the second most common organism in chronic suppurative otitis media.20
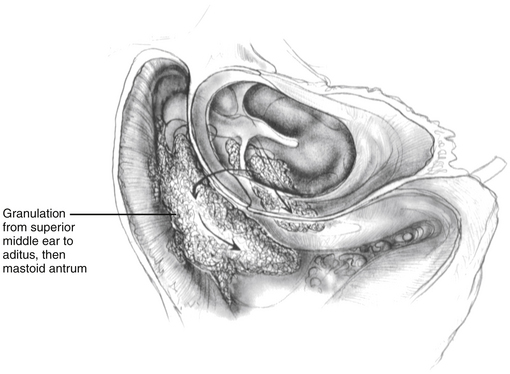
Obstruction of the aditus ad antrum, congenitally preformed pathways through the oval or round window; obstruction of acquired pathways from fractures or chronic erosive infection, granulation tissue, or cholesteatoma, especially virulent organisms such as H. influenzae type B; and synergistic pathogenicity resulting from anaerobic organism microenvironmental changes all may play a role in the pathogenesis of complications (Fig. 15-2).1,21 Clinically, several important observations can be made that help alert the physician to the possible occurrence of a complication and may reflect some of the pathobiology. Signs and symptoms of possible impending complications are (1) persistent acute infection for 2 weeks; (2) recurrent symptoms of infection within 2 weeks; (3) acute, fetid exacerbation of chronic infection; (4) fetid discharge during treatment; (5) H. influenzae type B or anaerobes cultured from the ear; and (6) fever in the presence of a chronically perforated tympanic membrane, with or without cholesteatoma.
CLINICAL PRESENTATION
Obvious Complications
Labyrinthitis
Labyrinthitis manifests as ipsilateral sensorineural hearing loss, nystagmus toward the contralateral side, and vertigo. It is classified according to what enters the perilymphatic space: serous labyrinthitis (toxins), suppurative labyrinthitis (bacteria), or chronic labyrinthitis (soft tissue, such as cholesteatoma).22 Suppurative labyrinthitis destroys all the hearing and may rapidly progress to meningitis. Labyrinthitis with some hearing, resulting from acute infection, is usually serous and isolated without other complications. Labyrinthitis with hearing, resulting from a cholesteatoma, may be associated with a labyrinthine fistula of the horizontal canal and a dehiscence of the fallopian canal, with or without facial paralysis.
Less Obvious Complications
Classic mastoiditis is easily recognized; however, without such obvious signs, masked mastoiditis (defined as radiographic evidence of bone destruction) may manifest as mild discomfort in the ear, with or without mastoid tenderness. The pathophysiologic and diagnostic key to occult complications is mastoiditis. Without careful medical care, the classic presentation of acute coalescent mastoiditis with subperiosteal abscess predominates and is quickly diagnosed. Masked mastoiditis may occur in patients with seemingly adequate care, however, and is much harder to diagnose promptly, and consequently can be much more devastating and is more often associated with intracranial complications.23,24 Patients with any of the signs and symptoms of impending complication, particularly with a recurrence of deep, although not severe, pain, may have masked mastoiditis. If bone destruction is present, the diagnosis is made. Masked mastoiditis may exist, however, without early evidence of radiographic bone destruction. If pain persists despite seemingly adequate culture-guided antibiotic administration, surgical mastoid exenteration with facial recess approach to the middle ear creating a posterior tympanotomy, deep mastoid cultures with sensitivities for aerobes and anaerobes, and aggressive medical treatment may be indicated.
Rarer subperiosteal or soft tissue abscesses can occur in the deep neck (Bezold’s abscess) or zygoma (Luc’s abscess). If purulent debris escapes through eroded bone and along vessels from the medial tip cells (medial to the digastric ridge and muscle) and diploetic bone and enters the neck through the incisura digastrica (the digastric groove on the inferior surface of the temporal bone), a Bezold’s abscess is formed. Purulent debris deep to the fascial planes of the sternocleidomastoid and trapezius muscles is difficult to localize by palpation.25 If pus tracks along the external auditory canal and accumulates under the temporalis muscle, a rare Luc’s abscess is formed.26
Brain abscesses have four stages, as follows:
Brain abscesses are silent; take weeks from onset to be detectable, even with imaging; and can be devastating. It is prudent to look for brain abscesses in cases of mastoiditis initially and again 3 to 4 weeks later (Fig. 15-3).