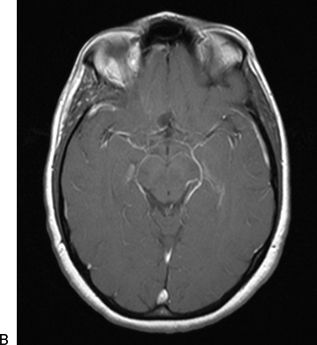
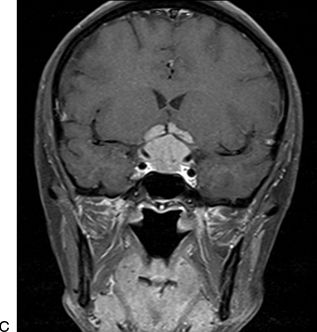
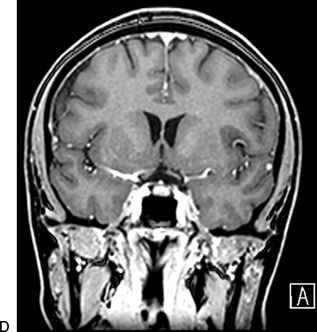
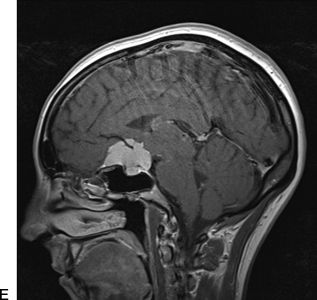
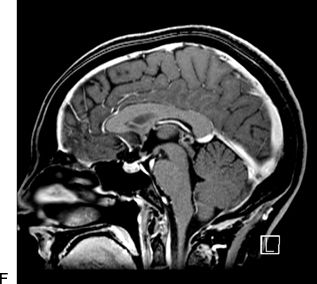
FIGURE 16.1 A–F. Preoperative (A, C, E) and postoperative (B, D, F) MRIs of a tubercular meningioma resected via a right supraorbital keyhole approach. The large size of the lesion and involvement of neurovascular structures were not contraindications to this keyhole approach. The postoperative MRI demonstrates a gross total resection.
Before surgery, patients for whom a supraorbital approach is selected should be counseled regarding the risk of numbness of the forehead, frontalis palsy, and nasal CSF leak although the rates of these complications are very low in experienced hands. In our series of over 450 cases, our CSF leak rate is negligible, and only two patients experienced permanent frontalis palsy.
SURGICAL TECHNIQUE
After intubation under general endotracheal anesthesia, the patient is placed in the supine position. The head is fixed in a 3-point rigid head holder. The table is placed in approximately 20 degrees of reverse Trendelenburg to optimize venous drainage. After pinning, the head is gently extended to bring it above the level of the heart, and 20 degrees of neck extension is applied to facilitate the natural “retraction” of the frontal lobe by gravity. This maneuver is crucial in opening the subfrontal corridor through which microsurgery will proceed and in avoiding the use of retractors. The head is then rotated slightly to the contralateral side to bring the malar eminence to the uppermost position. The degree of contralateral rotation may depend on the site of the surgical pathology, with 15 to 30 degrees used to address ipsilateral lesions and up to 45 to 60 degrees of rotation required to approach contralateral lesions. The ipsilateral eye is lubricated and closed with a temporary nylon tarsorrhaphy suture to prevent surgical prep solution from contacting the cornea.
Following positioning, the image-based frameless stereotaxic system is registered. Use of image guidance prior to incision is helpful to assess the position of the frontal sinus and to ensure an optimal trajectory to the lesion of interest. The lateral margin of the frontal sinus is marked, and the supraorbital notch is palpated. The supraorbital notch represents the medial limit of the skin incision. When the supraorbital notch is lateral to the frontal sinus, it also marks the medial limit of the craniotomy. In cases where a large frontal sinus extends lateral to the supraorbital notch, the lateral margin of the frontal sinus marks the medial limit of the craniotomy.
After prepping and draping, a skin incision is made within the eyebrow in its superior half (Fig. 16.2), extending from the supraorbital notch medially to the lateral aspect of the brow. The subgaleal layer is undermined, and the soft tissue is retracted superiorly with fishhooks. A U-shaped pericranial flap is fashioned by incising the pericranium as superiorly as possible and reflecting it inferiorly to the orbital rim. This pericranial flap is held inferiorly with sutures to the drapes. Laterally, the superior portion of the temporalis muscle is dissected to allow placement of a burr hole below the superior temporal line in the keyhole region. Any further temporalis dissection is unnecessary and should be avoided. A craniotomy is fashioned as low on the frontal floor as possible. The supraorbital craniotomy is typically 2 to 3 cm wide and 1.5 to 2 cm high (Fig. 16.3). While a small craniotomy can provide versatile access, the opening in the bone must be wide enough to accommodate a fully spread bipolar instrument. Particular lesions, such as those with a wide superficial component, may require a wider opening. Care is taken to preserve the supraorbital nerve medial to the craniotomy and to avoid violation of the frontal sinus. If the frontal sinus is breached, it can be packed with Betadine-soaked Gelfoam and sealed with bone wax, or repaired with the pericranial flap.

FIGURE 16.2 Proper positioning for the supraorbital craniotomy with eyebrow skin incision. The right eyelid temporary suture and skin incision, extended from the supraorbital notch to the lateral aspect of the brow (yellow line), are demonstrated in this photograph. The patient’s head is extended to allow the frontal lobe to fall away. The degree of head rotation may vary, depending on the size and location of the lesion of interest. In this case, minimal contralateral rotation was used. Rotation of the operating table during surgery, however, allows for the angle to be tailored during the course of the procedure.
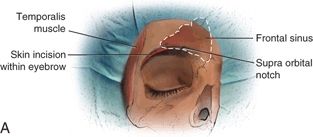
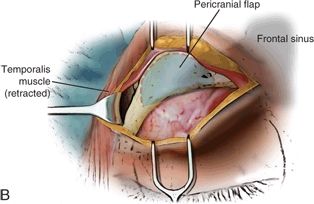
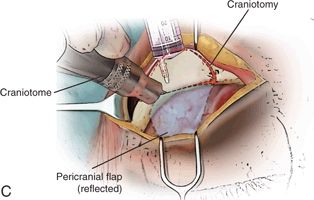
FIGURE 16.3 A. A skin incision is made within the eyebrow in its superior half, extending from the supraorbital notch medially to the lateral aspect of the brow. B. After the subgaleal layer is undermined and the soft tissue is retracted superiorly with fishhooks, a U-shaped pericranial flap is fashioned by incising the pericranium as superiorly as possible and reflecting it inferiorly to the orbital rim. C.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


