 trabismus is a very common condition that often needs surgical treatment to make the eyes orthophoric, prevent amblyopia, and promote binocularity and stereopsis. In this surgery, the various rectus muscles are recessed or resected; the oblique muscles are mostly cut, not strengthened. The instruments used are very basic: forceps, scissors, and bipolar cautery. The sutures used are usually absorbable. Surgery is followed by continued oozing to frank bleeding. The tenon capsule is difficult to exactly define, cut, and keep and suture in place. The extraocular muscle is detached from the insertion for both recession and resection purposes. Perfect realignment of the detached muscle may not be obtained while suturing. Postoperative reaction and scarring of the operated area are common. Repeat surgery on the same muscle is quite difficult.
trabismus is a very common condition that often needs surgical treatment to make the eyes orthophoric, prevent amblyopia, and promote binocularity and stereopsis. In this surgery, the various rectus muscles are recessed or resected; the oblique muscles are mostly cut, not strengthened. The instruments used are very basic: forceps, scissors, and bipolar cautery. The sutures used are usually absorbable. Surgery is followed by continued oozing to frank bleeding. The tenon capsule is difficult to exactly define, cut, and keep and suture in place. The extraocular muscle is detached from the insertion for both recession and resection purposes. Perfect realignment of the detached muscle may not be obtained while suturing. Postoperative reaction and scarring of the operated area are common. Repeat surgery on the same muscle is quite difficult.
By virtue of its ability to ablate tissues bloodlessly, use of the Fugo blade as a cutting and ablating tool brings about a sea change in how surgery on extraocular muscles may be done in the future. This extraordinary facilitation has permitted us to improve the surgical technique, reduce surgery time, increase the accuracy of alignment, minimize postoperative problems, and rehabilitate the patient more quickly. The surgical management of recti and the oblique muscles is described below.
Block Removal/Recession of a Rectus Muscle
The philosophy of this new recession procedure is not to detach the muscle but to weaken it by removing a muscle block while leaving intact a thin strip of muscle on either side. It may be likened to a sutureless recession. The vascularity of muscle tissue close to the insertion is not touched, therefore no danger of anterior segment necrosis exists if more than one muscle is addressed. The insertion can be cut selectively to reduce hypertropia or hypotropia. Because misalignment of the muscle is out of the question, the technique can be safely applied in cases of symptomatic phorias.
TECHNIQUE
Anesthesia
Most strabismus surgery is in pediatric patients, so general anesthesia is the normal choice. Under anesthesia, the eyeball may roll up and rotate, but this action will not prevent accurate positioning of the extraocular muscle.
Surgical Technique
- Fixing the eyeball: Pass a suture through the episclera close to the limbus and weight it to expose the surgical area. We use an 80-µm vanadium steel suture for this purpose.
- Use a Lim forceps to nudge the edge of the muscle to determine its position. As the muscle edge engages the forceps, the eyeball rotates.
- Make the conjunctival-tenon incision over the muscle as far away from the limbus as possible. On the nasal side, make the incision under the plica semilunaris, so that in the end the incision line is buried. Not dissecting the conjunctiva from the limbal side and not making large conjunctival flaps helps to prevent unnecessary injury to the tenon capsule and damage to the subconjunctival lymphatics and consequent scarring. Use a 100-µm Fugo blade tip at the lowest energy settings. Life the conjunctiva as it is being incised. The incision deepens imperceptibly with the incision of tenon capsule. Life the tenon capsule every time the incision is deepened. As the thickness of the tenon capsule is crossed, you will encounter very loose tenon connective tissue under which the muscle belly or tendon is clearly visible. The tenon capsule is very thick in children and needs bloodless ablation layer by layer until the muscle fibers become visible. Extend the incision up and down to reach the muscle edges. Once the edges have been defined, insert a muscle hook underneath it. Hold the tenon capsule with a forceps at the edge of the muscle and strip the capsule toward the fornix. Treat the other edge of the muscle in the same way. Once you strip the tenon capsule, it becomes easy to insert the second muscle hook and stretch the muscle between the two hooks. Hold any remnant of the capsule in the surgical field with a fine forceps and remove it with the Fugo blade. The whole process is bloodless (Fig. 15.1).
- Next, remove a block of the muscle to weaken it. The effect of this step is similar to the recession of the muscle. Depending on the weakening that is to be achieved, choose the proximal point on the muscle and bring the proximal muscle hook under it. Use the activated Fugo blade tip to make two longitudinal full-thickness cuts on the muscle over the muscle hook. Make each cut about 1 mm from the edge of the muscle. Never make the incision without a metallic support underneath, otherwise the sclera will be incised instantly. Advance the incisions toward the insertion over a metal spatula (the lens spatula). Stop the incisions short of the insertion, so that the blood vessel–bearing distal portion of the muscle is left untouched for about 1.5 mm. Now take the proximal muscle hook back again under the initial incisions. Cut the muscle vertically between the two incisions, over the muscle hook. The cut muscle block now hangs free from the insertion side. Lift it with a utility forceps and cut with Fugo blade about 1.5 mm from the insertion. At this point an approximately 1.5-mm strip of the intact muscle exists at insertion, from which a 1-mm strip along either edge stretches to the proximal part of the muscle. There is a rectangular empty area from which the block of muscle has been removed. Depending on the requirements of the case, further weaken the muscle by performing marginal tenotomy on the muscle strips that are left after block removal. The whole process is essentially bloodless and unaccompanied by tissue charring. The occasional bleeder can be touched with a 600-µm Fugo blade tip at the lowest setting. To improve concomitant hypertropia or hypotropia, cut the muscle strip along one edge, so that the eyeball gets more support toward the uncut side.
- Bring the tenon capsule and conjunctiva together in layers. The cut edges of the tenon capsule are easy to pick. We use 40-µm vanadium steel sutures for this purpose because they are nonmagnetic, cause no inflammation, and need no removal. The conjunctival sutures do not irritate and will eventually fall off. Absorbable sutures are also acceptable.
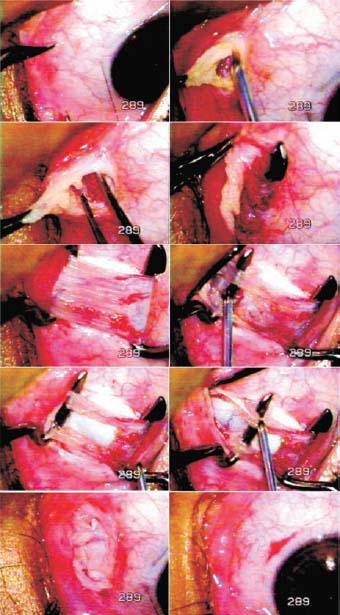
Figure 15.1. Medical rectus weakening. The forceps tip is used to find the edge of the muscle. The Fugo blade makes incisions through the conjunctiva and tenon capsule. The exposed muscle is stretched between muscle hooks. A block of muscle is removed, followed by marginal tenotomy of the remaining muscle strips. The tenon capsule and conjunctiva are sutured in layers.
Postoperative Management
The postoperative period is usually uneventful. No postoperative edema results after block removal/ recession.
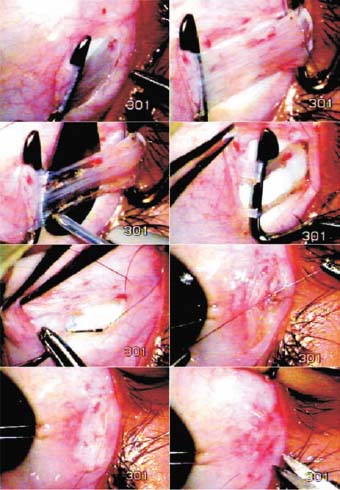
Figure 15.2. After the muscle is stretched between two muscle hooks, an anchoring 80-µm steel suture is passed through the belly of the muscle. Incisions are made to remove a block of the muscle and to leave thin strips along the two edges. The anchoring suture is passed through the insertion and tied. Notice the presence of a spatula beneath the muscle when the strips are being created with the Fugo blade.
Block Removal plus Plication/Resection
Surgical steps for block removal plus plication/resection are the same with regard to exposing muscle weakening. The muscle is stripped of the tenon capsule and stretched between the two muscle hooks (Fig. 15.2).
Surgical Technique
- Pass an 80-µm vanadium steel suture through the belly of the muscle at the desired distance from the insertion. Pass the suture twice and then fasten it.
- Block removal of the muscle is the next step. Keep the Fugo blade away from the knot, as touching the steel suture with the activated Fugo blade can weaken and even break the suture.
- Loose the eyeball-fixating suture. Pass the advancement suture through the episclera at the insertion of the muscle. Tie the suture in a reef knot and cut close to the knot. The suture should not project forward or it will cause severe irritation. Although our preference is for steel sutures, an absorbable suture can be used.
- Suture the tenon capsule and the conjunctiva in layers.
Postoperative Management
Patients feel discomfort for a few hours after plication/advancement because the muscle has been stretched.
Surgery on the Vertical Muscles
The surgery of the vertical muscles is just the same as in the case of the horizontal muscles. The Fugo blade technique of block removal completely avoids dealing with the sclera.
Surgery on the Inferior Oblique Muscle
Overaction of the inferior oblique muscle is frequently responsible for hypertropia. The treatment is myomectomy of the inferior oblique muscle. In the usual approach, muscle body is exposed from either the skin side or the conjunctival side, held between artery forceps, and cut. This is easier said than done. Bleeding from cutting the conjunctiva and tenon capsule makes the surgery cumbersome. Using the Fugo blade makes the surgery bloodless and clean (Fig.15.3).
TECHNIQUE
Surgical Technique
- Reveal the edge of the inferior rectus by nudging with a forceps about 10 to 12 mm from the limbus. The inferior oblique muscle passes underneath this muscle horizontally near the equator of the eye.
- To approach the belly of the inferior oblique muscle, make an incision in the conjunctiva with the Fugo blade about 8 to 10 mm temporal to the lateral edge of the inferior rectus and about 12 to 15 mm from the limbus. Then lift and cut the tenon capsule until the sclera becomes visible.
- Use a stout forceps to move the sclera over to reach and hold the belly of the inferior oblique muscle and pull it out in the incision line. The tenon capsule covering of the muscle is quite thick. Pass the Fugo blade underneath the muscle and the tenon capsule. Then pass a muscle hook through the track made by the Fugo blade, followed by a second muscle hook. Stretch the inferior oblique muscle between the two hooks.
- No artery forceps is used to clamp the muscle. Incise the highly vascular and muscular belly gradually with a 300-µm or 600-µm Fugo blade tip at low energy settings. The muscle is ablated without bleeding. Some muscle fibers are left intact; create a gap by removing a 4- to 5-mm length of the muscle. Touch any bleeder with the 600-µm tip. Remove the muscle hooks.
- Close the tenon capsule and conjunctiva separately with a couple of 40-µm vanadium steel sutures. Absorbable sutures can also be used for closing the incisions.
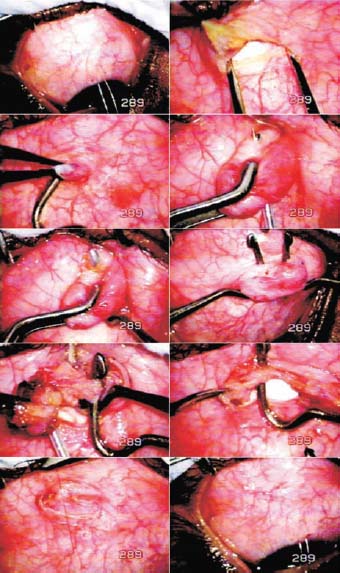
Figure 15.3. After exposing the surgical area, the conjunctiva and tenon capsule are cut with the Fugo blade to expose the sclera. The inferior oblique muscle is pulled out and a Fugo blade track is made under the muscle through the tenon capsule to make room for the muscle hooks. The stretched muscle is attenuated with the Fugo blade. The incision is closed in layers.
Surgery on the superior oblique muscle is similar. The muscle may best be located on the nasal side of the superior rectus muscle.
Repeated Surgery on Extraocular Muscle
Repeated surgery on any extraocular muscle is often difficult because of the presence of scar tissue in the operative field. Ordinarily, dissection is difficult—having to cut through scar tissue to define and operate on the muscle. Bleeding is another problem. The Fugo blade makes resurgery much easier.
Summary
The Fugo blade makes surgery on extraocular muscles bloodless and efficient. The surgical time spent on each muscle is about 7 to 8 minutes. The block removal technique provides a new kind of recession, and plication preserves muscle vascularity near the insertion, thereby abolishing the risk of anterior segment necrosis. Every extraocular muscle is easy to approach and operate. Phoria cases can be operated with greater confidence. Because the blood vessels are closed during Fugo blade incisions on the tenon capsule and the muscle, little postoperative reaction results and recovery is therefore quick. Keeping the incisions away from the limbus preserves the conjunctival lymphatics and minimizes tenon capsule scarring.
Suggested Reading
Singh D, Singh RSJ, Kaur H, et al. Plasma powered squint surgery with the Fugo blade. Ann Ophthalmol. 2003;35:12–14.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


