 hallmark of modern cataract surgery is excellent visualization with a modern coaxial operating microscope. As with any biologic phenomenon, dilation of the pupil can be quantitated by placing it on a bell-shaped curve. My colleagues and I have noted that some patients’ eyes maximally dilate with one set of dilating eye drops whereas others barely dilate with a large series of dilating eye drops. Patients on alpha-antagonists such as tamsulosin, alfuzosin, terazosin, and doxazosin manifest poor dilation with an “irrational” acting iris during cataract surgery, such as a billowing iris. This phenomenon is known as “floppy iris syndrome”1 (Fig. 21.1). The surgeon can stretch the iris when performing a Fugo blade capsulotomy because the nucleus is removed from the lens bag and lodged in the pupil. Herein, the nucleus acts to stabilize the iris while the phaco tip is meticulously disassembling the nucleus (Figs. 21.2 and 21.3) Corneal opacity such as seen in Salzmann nodular degeneration is also a challenge for modern cataract surgery because it poses an obstruction to visualization.
hallmark of modern cataract surgery is excellent visualization with a modern coaxial operating microscope. As with any biologic phenomenon, dilation of the pupil can be quantitated by placing it on a bell-shaped curve. My colleagues and I have noted that some patients’ eyes maximally dilate with one set of dilating eye drops whereas others barely dilate with a large series of dilating eye drops. Patients on alpha-antagonists such as tamsulosin, alfuzosin, terazosin, and doxazosin manifest poor dilation with an “irrational” acting iris during cataract surgery, such as a billowing iris. This phenomenon is known as “floppy iris syndrome”1 (Fig. 21.1). The surgeon can stretch the iris when performing a Fugo blade capsulotomy because the nucleus is removed from the lens bag and lodged in the pupil. Herein, the nucleus acts to stabilize the iris while the phaco tip is meticulously disassembling the nucleus (Figs. 21.2 and 21.3) Corneal opacity such as seen in Salzmann nodular degeneration is also a challenge for modern cataract surgery because it poses an obstruction to visualization.

Figure 21.1. A pupil with floppy iris syndrome has been stretched and an 8-mm capsulotomy is being created under the iris out of the surgeon’s view.
Many types of iris retraction devices can mechanically dilate the iris.2–5 All of these devices have issues such as cost, lengthening the time of surgery, corneal trauma, and iris trauma. Iris retraction with micromanipulator probes is often helpful, but it provides limited dilation.6,7 A large superior sector iridectomy is often helpful, but it can cause an undesirable cosmetic outcome.8 Small incisions scattered along the pupil margin require expensive micro-scissors and produce only a moderate increase in pupil dilation. This approach can cause bleeding and significantly increase surgical time.

Figure 21.2. The nucleus in Figure 21.1 is impaled with the phaco tip, which is used to pluck it out of the lens bag while visco-elastic material is injected behind the nucleus with a side port cannula.

Figure 21.3. A pool of visco-elastic material acts to hold up the nucleus in the pupil, thereby acting to stabilize this iris as the nucleus is meticulously disassembled in the iris plane.
The Fugo blade offers a new dimension in the management of small-pupil cataract surgery.9 The Fugo blade allows the surgeon to ablate anterior capsule under the iris out of view of the surgeon.10 Because I prefer large capsulotomies, I perform about 40% of my capsulotomies under the iris without any visualization of the capsulotomy. The learning curve for this maneuver is quite low, while the outcome is truly invaluable.11
Surgical Technique
- Infuse visco-elastic between the iris and capsule to lift the iris off the anterior capsule 360 degrees.
- Introduce the Fugo blade tip into the anterior chamber and begin ablating the capsule within the pupil, then slowly continue the ablation outward under the iris. You will see the iris surface mildly tent up as the Fugo blade tip passes under a given point of the iris (Fig. 21.4).
- Do not move the Fugo blade under the iris if the tip is not activated because this risks a mechanical tear in the capsule.
- Perform capsule ablation in one continuous maneuver or in several connected arcuate maneuvers that begin and end within the pupil, thereby beginning with visualization and ending with visualization.
- A major risk of Fugo plasma capsulotomy is to leave a skip lesion in the capsule, resulting in the capsulotomy not being a complete 360-degree ablation but rather a peninsula-shaped skip area attached to the central capsule island created with the Fugo blade. To eliminate skip lesions, I perform three or four 360-degree capsulotomies at the same general location on the capsule. I perform each in a slow and deliberate manner, requiring about 30 seconds each. If a skip lesion in the capsule is left when phaco begins, removal of the central capsule island may cause the island to tear out peripherally toward the equator.
- Since I routinely use a large capsulotomy, I can impale the nucleus with the phaco tip and rock it out of the lens bag (Fig. 21.5). I normally ablate the capsule at a distance of 2 mm from the limbus. This leaves a small but healthy capsule rim with no significant damage to the zonules. Be sure to hydrodissect prior to impaling the nucleus with the phaco tip.
- Once the nucleus is out of the lens bag and still on the phaco tip, a visco-elastic cannula can be inserted through a cornea side stab incision and visco-elastic material can be injected behind the nucleus to push the posterior capsule backward and hold the nucleus in the pupil after it is released from the phaco tip (Fig. 21.6).
- The nucleus acts to hold the pupil open as you mechanically crack it, then you perform phaco-emulsification on the cracked piece of nucleus in the iris plane (Fig. 21.7).

Figure 21.4. A Fugo blade is seen under a constricted iris while an 8-mm capsulotomy is ablated out of the surgeon’s view.
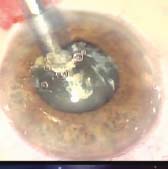
Figure 21.5. After an 8-mm capsulotomy formation, the phaco tip is used to impale the nucleus to lift it out of the lens bag as well as having the nucleus stretch the pupil open.

Figure 21.6. The impaled nucleus is used to pull the pupil open while visco-elastic material is injected behind it to hold the nucleus up in the pupil.
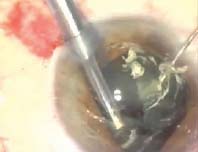
Figure 21.7. Held in the pupil on a cushion of viscoelastic material, the nucleus is mechanically cracked in the iris plane with the phaco tip and the nucleus manipulator.
Summary
This Fugo blade technique dramatically simplifies cataract surgery in small-pupil cases. Once a surgeon learns this procedure, he or she will be able to take control of those difficult small-pupil cataract cases (Figs. 21.8 and 21.9).

Figure 21.8. Once the nucleus and cortex are removed, the intra-ocular lens is unfolded into the lens bag.

Figure 21.9. The intra-ocular lens (IOL) is being moved back and forth with the IOL manipulator to check for haptic spring and IOL centration. In this case, the observed results are excellent.
References
1. Chang DF, Campbell JR. The intraoperative floppy iris syndrome associated with tamsulosin. Cataract Refract Surg Today. 2005;31:664–673.
2. De Juan E, Hickingbotham D. Flexible iris retractor. Am J Ophthalmol. 1991;111:776–777.
3. Fine IH. Phacoemulsification in the presence of a small pupil. In: Steinert RF, ed. Cataract surgery: technique, complications and management. Philadelphia, Pa: Saunders, 1995:199–208.
4. Mackool RJ. Small pupil enlargement during cataract extraction: a new method. J Cataract Refract Surg. 1992;18:523–526.
5. Nichamin LD. Enlarging the pupil for cataract extraction using flexible nylon iris retractors. J Cataract Refract Surg. 1993;19:793–796.
6. Miller KM, Kenner GT. Stretch pupilloplasty for small pupil phacoemulsification. Am J Ophthalmol. 1994;3: 107–108.
7. Dinsmore SC. Modified stretch technique for small pupil phacoemulsification with topical anesthesia. J Cataract Surg. 1996;22:27–30.
8. Lu LW, Fine IH. Phacoemulsification in difficult and challenging cases. New York: Thieme, 1999.
9. Fugo RJ, DelCampo DM. The Fugo blade™: the next step after capsulorrhexis. Ann Ophthalmol. 2001;33:12–20.
10. Fugo RJ, Singh D, Fine IH. Automated Fugo blade capsulotomy: a new technique and a new instrument. Eyeworld. 2002;7:49–54.
11. Fugo RJ. Strategy for capsulotomy. Cataract Refract Surg Today. 2007;7:15.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


