Purpose
To study the utility of hybrid single photon emission computed tomography / computed tomography (SPECT/CT) scan and dual-dye technique in identification of the sentinel lymph node (SLN) in patients with an advanced malignant eyelid tumor.
Design
Nonrandomized prospective interventional study.
Methods
setting : A tertiary eye care center. study population : Patients with an advanced malignant eyelid tumor without clinically involved regional lymph nodes. intervention : SLN biopsy was performed using dual-dye technique (a combination of radiotracer and vital blue dye) following localization by SPECT/CT. main outcome measures : Localization of SLN in the regional node basin by hybrid SPECT/CT scan; SLN identification rate using dual-dye technique; SLN positivity rate; false-negative rate; and complications, if any, of SLN biopsy.
Results
Sixteen patients of biopsy-proven eyelid malignancy (7 squamous cell carcinomas [43.75%], 5 sebaceous cell carcinomas [31.25%], and 4 malignant melanomas [25%]) were included in the study. Preoperative localization of SLN was performed using SPECT/CT in 12 patients. SLN biopsy using dual-dye technique was performed in 16 patients. SPECT/CT accurately localized SLN in 11 out of 12 patients. The preauricular region was the most common site of SLN. SLN identification rates for dual-dye, radiotracer, and blue dye techniques were 100% (16/16 patients), 100% (16/16 patients), and 87.5% (14/16 patients), respectively. SLN showed metastasis in 2 patients (12.5%). On follow-up, 1 patient developed cervical lymph node metastasis, thus giving a false-negative rate of 7.14%. There were no complications associated with SLN biopsy.
Conclusion
Accurate preoperative localization of SLN in relation to adjacent anatomic structures using SPECT/CT aids in intraoperative identification of SLN. SLN biopsy should be considered in patients with eyelid tumors at significant risk for metastasis who have clinically negative nodal basins. Dual-dye technique is safe and feasible in advanced eyelid tumors. Blue dye technique can be used for SLN biopsy in settings where nuclear medicine facilities are not available, albeit with a lower SLN identification rate. Detection of metastasis in SLNs in ∼12% of cases emphasizes the utility of SLN biopsy in accurate staging and treatment of eyelid malignancies.
The sentinel lymph node (SLN) is defined as the first lymph node along the lymphatic drainage pathway of a region. SLN biopsy has been shown to predict nodal status as accurately as regional lymph nodal dissection in most solid cancers, without its attendant morbidity. SLN biopsy can be performed using vital blue dye (blue dye technique), radiotracer (radiotracer-guided technique), or a combination of both (dual-dye technique). Combination technique (dual-dye technique) has been shown to have the highest SLN identification rate and lowest false-negative rate in breast cancer and cutaneous melanomas.
Preoperative dynamic and plain lymphoscintigraphy is performed by most investigators to localize and plan SLN biopsy. However, as no anatomic landmarks are delineated in conventional lymphoscintigraphy preoperatively it is difficult to accurately localize the SLN, especially in head and neck cancers. Hence, hybrid single photon emission computed tomography / computed tomography (SPECT/CT) is becoming a popular tool for accurate preoperative localization of SLN(s). There are few reports evaluating the role of SLN biopsy in ocular and adnexal malignancies. All the published studies have included few patients, and 4 of these studies are from a single center.
The current study was undertaken to evaluate the feasibility and utility of SPECT/CT and dual-dye technique for localization of the SLN in patients with advanced malignant eyelid tumors.
Methods
This was a nonrandomized prospective interventional study conducted at a tertiary eye care center. Patients were recruited prospectively between January 2010 and December 2011 after obtaining Institutional Ethics Committee (All India Institute of Medical Sciences, New Delhi, India, ethical clearance ref. no. IESC /T-91/2010) approval. Informed written consent to participate in this study was obtained from all patients. Patients with biopsy-proven advanced malignant eyelid tumor (squamous cell carcinoma/sebaceous cell carcinoma/melanoma) involving more than one third of the eyelid with or without orbital involvement (fornix, extraocular muscles, or other orbital structures) were enrolled in the study. Patients with other eyelid tumors, proven metastasis, pregnancy, or history of radiotherapy were excluded. Detailed locoregional examination of the eye, eyelid tumor, and regional nodes was performed. Patients with palpable regional lymph node were excluded. The tumors were assigned to surgical zones as proposed by Spinelli and Jelks zone I, on upper eyelid; zone II, on lower eyelid; zone III, at the medial canthal region; zone IV, at the lateral canthal region; and zone V, any area outside zone I to IV but contiguous with these zones. Contrast enhanced computed tomography head and neck was done in all patients to assess the extent of the primary tumor and regional lymph node status. Systemic examination included hemogram, serum liver and renal function tests, chest radiograph, and ultrasound of the abdomen and pelvis. TNM staging (tumor, node, and metastasis staging for malignant tumors) was done as per the 7th edition of AJCC (American Joint Committee on Cancer).
Preoperative Lymphoscintigraphy
99m Tc-sulfur colloid (t½ 6 hours) radiotracer was used. Preoperative lymphoscintigraphy was performed in the nuclear medicine department, wherein 0.1 mL of 400 μCi (if SLN biopsy was performed on the same day) or 4 mCi (if surgery was planned as the first case on the following day) was injected perilesionally (intradermal/subconjunctival), depending on the epicenter of the primary tumor. Hybrid SPECT/CT scan was performed to identify and locate the SLNs in the regional nodal basin (preauricular, intraparotid, and submandibular).
Intraoperative Procedure
SLN biopsy and surgical excision of the primary tumor were performed in 2 different sittings during the same hospital stay. In the first sitting, SLN biopsy was performed under general or local anesthesia by a single surgeon (V.S.). A hand-held gamma probe was used transcutaneously to localize SLN(s) in the preauricular and neck areas, using images from preoperative SPECT/CT as a guide. The area of highest radioactive counts (in vivo 10-second count) as compared to background (opposite shoulder) was identified and marked on the skin. One milliliter of 1% isosulfan blue dye was injected perilesionally (intradermal). Gentle massage of adjacent tissues was performed to augment lymphatic drainage. A curvilinear skin incision was made after 5 minutes, directly over the area of highest radioactive counts. Using blunt and sharp dissection, effort was made to identify blue-stained lymphatic tract leading to a blue node. Any lymph node that was blue, radioactive, or radioactive and blue was considered an SLN and was excised with surrounding fat. In addition, any suspicious intraoperatively palpable node adjacent to the SLN was also excised. If the node was deeply embedded in the parotid tissue, superficial or total parotidectomy with preservation of the facial nerve was performed. Ex vivo radioactive counts (10 seconds) of the excised SLN were obtained by placing the node on the tip of the gamma probe. All lymphatic tissue with counts 10% or more compared to the highest ex vivo counts was excised and labeled as SLN. The preauricular and neck region were rechecked with the gamma probe to confirm the removal of SLNs.
All the dissected lymph nodes were sent in 10% neutral buffered formalin for histopathologic examination. The lymph nodes were breadloafed in 2-mm-thick slices. Blocks were evaluated by routine hematoxylin-eosin stain.
In the second sitting, depending upon the extent of primary tumor, orbital exenteration or local excision of the tumor (under frozen-section control of the margins) with eyelid reconstruction was performed.
Postoperatively, patients were monitored for hemorrhage, edema, facial nerve palsy, wound infection, wound dehiscence, or any other problem. Following discharge, all patients were followed up at 3 monthly intervals and evaluated for locoregional recurrence and distant metastasis. An SLN was considered as false negative if any of the patients with negative sentinel lymph node presented with nodal metastasis at follow-up.
Statistical Analysis
At the end of the study, data analysis was done using SPSS software version 15 (SPSS Inc, Chicago, Illinois, USA). Mean and frequency distribution was calculated for all variables in the study. Correlation calculation was done using appropriate statistical tests (Pearson χ 2 test, Kruskal-Wallis test, Fisher exact test) and P value < .05 was considered significant. Association or comparison between 2 techniques (radiotracer vs blue dye) was done by agreement analysis (measuring kappa value, κ %).
Results
Sixteen patients with biopsy-proven eyelid malignancy (squamous cell carcinoma, 7 [43.75%]; sebaceous cell carcinomas, 5[31.25%]; and malignant melanoma, 4 [25%]) were studied. The age of patients ranged between 25 and 75 years (mean ± SD, 55.9 ± 14 years); 5 patients were female. The left eye was more frequently affected than the right (13:3). The duration of symptoms ranged from 3-48 months (mean ± SD, 15 ± 16 months).
Surgical zone distribution of the tumors was as follows: zone I: 10; zone II: 5; zone III: 0; zone IV: 1; zone V: 0. Overall, zone I was the most common (10/16, 62.5%) zone involved. While zone I was the most common zone involved in sebaceous cell carcinoma (4/5) and melanoma (4/4), zone II was the most common zone affected in squamous cell carcinoma (5/7). TNM stage distribution was as follows: T2bN0M0, 5 patients; T3aN0M0, 2 patients; T3bN0M0, 8 patients; T3cN0M0, 1 patient. Whereas palpebral conjunctiva was involved in all the cases, bulbar conjunctival involvement in addition was present in 8 patients. Orbital involvement was present in 8 patients. None of the patients had clinical or imaging evidence of regional or systemic metastasis.
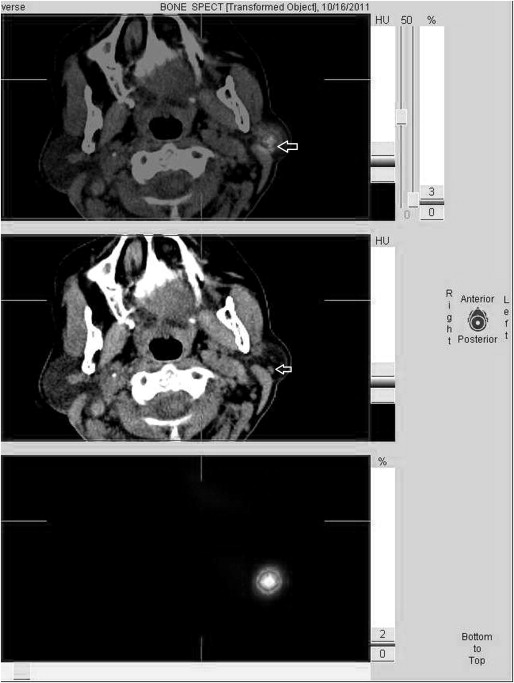
Preoperative localization of the SLN using SPECT/CT was performed in 12 patients ( Figure ). In 4 patients, because of malfunction of the SPECT/CT machine, SPECT/CT could not be done and radiotracer was injected in the operating theatre, following which lymphatic mapping was done preoperatively using a hand-held gamma probe. SPECT/CT successfully located the SLN basin in all but 1 patient (11/12). Dual-dye technique for intraoperative identification of SLN was performed in all 16 patients. SLN biopsy was done under general anesthesia (14 patients) and local anesthesia (2 patients). Radiotracer identified the SLN in all patients (100%), while blue dye technique could identify SLN in 14 patients (87.5%). Statistical analysis for identification of SLN using radiotracer vs blue dye technique showed excellent agreement (κ = 94%) between the 2 techniques. In the patient in whom SPECT/CT failed to map SLN, dual-dye technique identified 1 radioactive and blue SLN.
The most common lymphatic basin where the SLN was identified was preauricular (87.5%), followed by submandibular (12.5%). Submandibular SLN was harvested in 1 patient with squamous cell carcinoma (zone II) and 1 with sebaceous cell carcinoma (zone IV). In 1 patient with sebaceous cell carcinoma in zone I, an SLN was found deeply embedded in the parotid gland, necessitating total parotidectomy with preservation of facial nerve. The harvested SLN was negative for metastasis. A total of 26 nodes were harvested in 16 patients and the average number of nodes harvested per patient was 1.6 (range 1-4).
Harvested nodes (n = 26) were only radioactive (n = 7), only blue (n = 4), or both radioactive and blue (n = 13) (2 nodes that were neither radioactive nor blue were excised because of their close proximity to the SLN). Average duration of SLN biopsy was 30 minutes (median, 25 minutes; range, 15-45 minutes). No intraoperative complications were observed.
Histologically positive SLNs were found in 2 out of 16 patients (SLN-positive rate, 12.5%). One patient in whom 2 submandibular nodes were harvested had a well-differentiated sebaceous cell carcinoma (zone IV) ( Supplemental Figure , Top, available at AJO.com ). Both nodes were radioactive as well as blue. Because of the high clinical suspicion of metastasis, the nodes were sent for frozen-section analysis, which was positive for metastasis. Subsequently, complete cervical lymph node dissection was done in the same sitting. After 1 week, exenteration was done and adjuvant radiotherapy was given to the ipsilateral neck. Another patient with positive SLN, in whom 1 preauricular node was harvested that was radioactive but not blue ( Supplemental Figure , Middle, available at AJO.com ), had squamous cell carcinoma (zone II). Exenteration with complete cervical lymph node dissection was done thereafter and adjuvant radiotherapy was given.
Exenteration was done in a total of 7 patients with orbital involvement (3 squamous cell carcinoma, 1 sebaceous cell carcinoma, 3 melanoma). In the remaining 9 patients, frozen-section-guided local excision with eyelid reconstruction was done. For histopathologic examination of the primary tumor, routine hematoxylin-eosin staining was done. Four out of 5 patients with sebaceous cell carcinoma (including the SLN-positive patient) had well-differentiated tumors and 1 patient had a moderately differentiated tumor. None of them had any evidence of pagetoid spread. All squamous cell carcinomas were well differentiated except 1, which was poorly differentiated with intraocular (uveal) involvement and was also SLN positive. Mean Breslow thickness in malignant melanoma was 3.68 mm (range, 2.32-4.86 mm). All melanomas were of epithelioid cell type with no ulceration.
Postoperative Period and Follow-up
All patients had bluish discoloration of the eyelid/periocular skin and urine for first 24-48 hours after SLN biopsy. No allergy or anaphylaxis was noted. All patients had ipsilateral facial edema, which subsided spontaneously in 4-5 days. One patient, in whom total parotidectomy was done, complained of dryness of mouth for 3-4 weeks; symptoms subsided thereafter. The median follow-up time was 12.25 months (range, 9-23 months). No eyelid or orbital residual disease or recurrence was found in any patient. One patient with melanoma developed cervical lymph nodal metastasis at 1 month follow-up. SLN of this patient was reported negative at initial evaluation. Slide review revealed subcapsular singly lying melanoma cells that were missed during earlier evaluation ( Supplemental Figure , Bottom, available at AJO.com ). The patient underwent complete cervical lymph node dissection followed by radiotherapy and is disease free at last follow-up. Thus the false-negative rate of SLN biopsy in the present study was 7.14% (1/14). Two patients in whom SLN biopsy revealed metastasis underwent modified radical neck dissection and adjuvant radiotherapy, and were disease free at last follow-up.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


