Mixed Tumor
Overall, mixed tumor or pleomorphic adenoma is the most common neoplasm of the seromucinous glands of the upper aerodigestive tract.
3,5 These tumors may develop in patients of any age and are somewhat more common in women. Within the upper aerodigestive tract, the tumors most commonly develop in the palate, likely secondary to the large number of seromucinous glands present at this site.
Grossly, the tumors are firm and appear well circumscribed. They may be mobile; however, they can involve the adjacent bone, as space for growth tends to be limited throughout the upper aerodigestive tract.
6 Unlike their counterparts in the major salivary glands, these tumors rarely
will have well-developed capsules. They should, however, remain circumscribed without widely infiltrative margins (e-
Fig. 6.1).
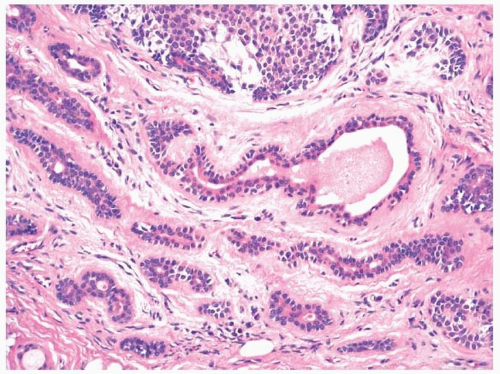
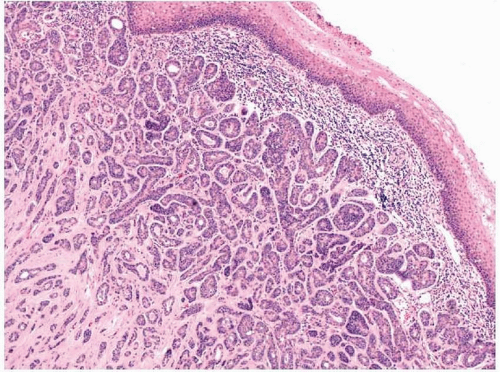
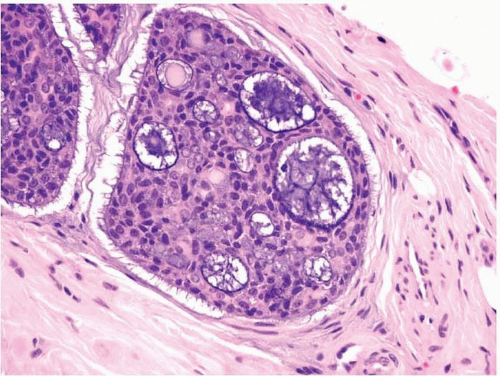
5,6Mixed tumors are especially known for their histologic heterogeneity and will display both epithelial and mesenchymal components.
3,5,6 The epithelial components show both true epithelial and myoepithelial differentiation. Architecturally, the epithelial cells often form glandular structures with lumina (
Fig. 6.1, e-
Fig. 6.2). The architecture, however, can be complex and numerous anastomosing trabeculae, small tubular glands, nests, and single epithelioid cells may be present (e-
Fig. 6.3). The epithelial cells may be columnar, cuboidal, squamous, plasmacytoid, oncocytoid, basaloid, clear, or spindled (e-
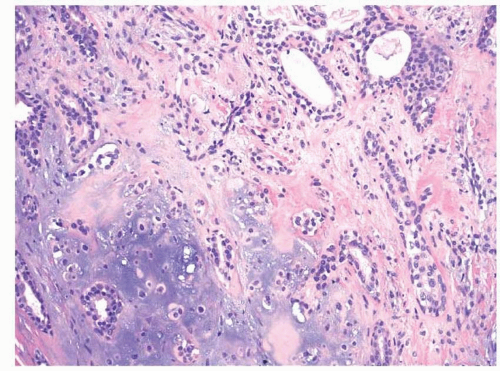
Fig. 6.4). Most tumors have more than one epithelial cell type scattered throughout the lesion. The stromal elements may by myxoid, hyaline, chondroid, adipose, or even osseous (
Fig. 6.2, e-
Fig. 6.5). Both the mesenchymal and epithelial elements generally show bland cytologic features, and mitotic figures are rare. Mixed tumors of the seromucinous glands typically show a more cellular, myoepithelial phenotype than their counterparts in the major salivary glands and have less stromal elements.
5 Furthermore, in our experience, they often contain more prominent squamous differentiation.
The differential diagnosis for these lesions may include other salivary gland-type adenomas and malignancies such as polymorphous low-grade adenocarcinoma, adenoid cystic carcinoma, and, occasionally, mucoepidermoid carcinoma when a prominent squamous component is seen. The distinction between these mixed tumors and other adenomas
on biopsy is somewhat academic; however, even distinguishing them from malignancies is not always necessary as complete (margin-free) excision is recommended for all these lesions. This is necessary as the benign tumors may recur without complete excision and even sometimes develop into or concomitantly harbor malignancies (carcinoma ex pleomorphic adenoma).
The immunohistochemical profile of mixed tumors depends somewhat on the dominant phenotype of the tumor, i.e., whether the tumor shows mostly epithelial, myoepithelial, or mesenchymal differentiation.
7 Most of the epithelial components will express various cytokeratins and show variable degrees of myoepithelial differentiation with expression of smooth muscle actin (SMA), calponin, S100, and glial fibrillary acidic protein (GFAP), CD10, and p63 (e-
Fig. 6.6).
6,7,8 and
9Many mixed tumors have been shown to harbor karyotypic abnormalities, with frequent abnormalities involving 8q12 and the long arm of chromosome 12.
10,11 These abnormalities correspond with the
PLAG1 and
HMGA2 genes, respectively, two genes involved in transcription.
12,13 and
14 Both proteins can be shown to be overexpressed in some mixed tumors by immunohistochemistry.
The distinction between mixed tumors and polymorphous low-grade adenocarcinomas or even adenoid cystic carcinomas can be difficult on biopsy, especially when the particular mixed tumor is very cellular. The identification of a mesenchymal component would be indicative of a mixed tumor, whereas the identification of perineural invasion or obvious
infiltration of surrounding tissues would be indicative of a polymorphous low-grade adenocarcinoma or adenoid cystic carcinoma. Mixed tumors almost always behave in a benign fashion and rarely recur if completely excised.
6,15
Other Adenomas
Other benign salivary gland-type epithelial tumors may also develop throughout the upper aerodigestive tract. These primarily include myoepitheliomas and canalicular adenomas, although basal cell adenomas and sebaceous adenomas have also been described. One should note that malignancy is usually determined by clear-cut infiltration into surrounding tissues, and the unequivocal diagnosis of benignancy cannot always be made based on small biopsy specimens.
Canalicular adenomas most often involve the upper lip.
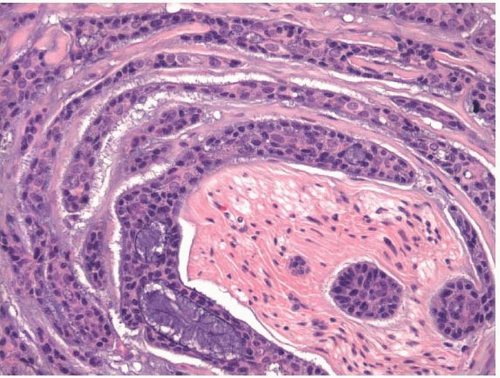
16,17 They are usually but not invariably solitary. They are rarely larger than 2 cm and are typically described as painless. The tumors are circumscribed but most do not have capsules. Microscopically, long rows or columns of cuboidal to columnar epithelial cells interweave throughout the tumors and lead to a “beaded” canalicular pattern (
Fig. 6.3, e-
Fig. 6.7). Cellular atypia and mitotic figures are rare (e-
Fig. 6.8). The entrapped stroma is pink and often contains many small capillaries. Epithelial antigen expression can be detected by immunohistochemistry, as can the expression of S100 protein.
18 Other markers of myoepithelial differentiation such as actins or p63 are not expressed.
19 After excision, the tumors rarely recur.
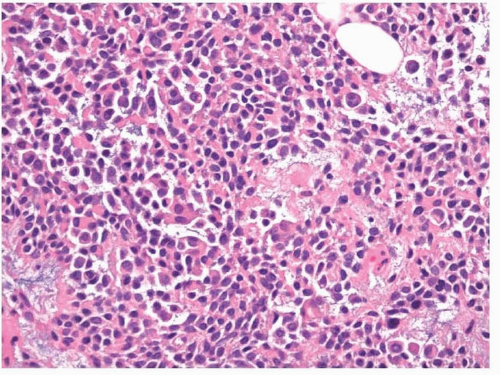
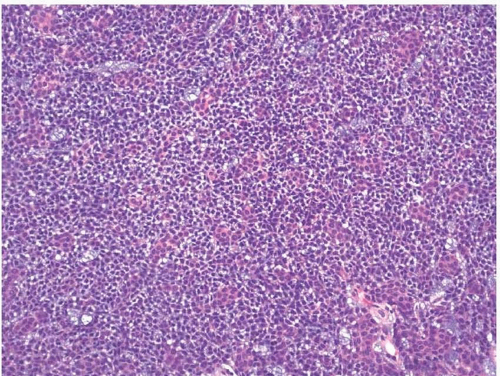
Myoepitheliomas resemble mixed tumors grossly and clinically but microscopically lack epithelial architecture and a significant
mesenchymal component (other than myxoid stroma) (
Fig. 6.4).
20,21 and
22 In other words, they are composed entirely of myoepithelial cells. The myoepithelial cells can show a variety of histologic appearances but are usually categorized as epithelioid, spindled, plasmacytoid (rhabdoid), or clear cell (
Fig. 6.5, e-
Figs. 6.9,
6.10 and
6.11). The tumors can have a variable cellularity and some tumors may have a prominent myxoid background.
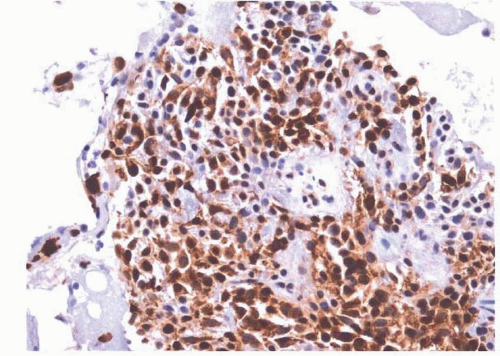
Immunohistochemically, the cells express cytokeratins and will show some degree of myogenous differentiation that can be demonstrated with antibodies to SMA, calponin, S100, GFAP, or p63, although more specific markers of myogenous differentiation are sometimes not seen, especially with the plasmacytoid variant (
Fig. 6.6, e-
Figs. 6.12,
6.13 and
6.14).
8,21,22 and
23 Surgical resection should attempt to achieve free margins and the tumors only rarely recur.
20,22
The differential diagnosis for myoepitheliomas depends on the phenotype. The plasmacytoid variant must be distinguished from melanoma and plasmacytoma, which can be done by showing epithelial or myogenous differentiation. Antibodies more specific for melanoma or plasmacytoma antigens such as HMB-45 or CD138, respectively, may also be helpful. Spindle cell myoepitheliomas have a broad differential diagnosis including numerous mesenchymal tumors (e.g., nodular fasciitis, schwannoma, neurofibroma, solitary fibrous tumor, and melanoma). Antibodies to epithelial antigens or p63 may be helpful, as may antibodies more specific to some of the mesenchymal tumors in the differential diagnosis (e.g., CD34 for solitary fibrous tumors). Finally, clear cell myoepitheliomas must be differentiated from other clear cell tumors (see below). To distinguish myoepithelioma from myoepithelial carcinoma, one must rely on both cytologic features and growth pattern (see below).
Many reported cases of
basal cell adenoma of the upper aerodigestive tract appear to have been canalicular adenomas, and some authors consider canalicular adenoma simply to be a variant of basal cell
adenoma.
24,25 Indeed, in reviewing the literature, it is difficult to calculate the number of basal cell adenomas involving the upper aerodigestive tract that did not have a canalicular pattern. It appears that even if basal cell adenomas are distinguished from canalicular adenomas, basal cell adenomas still most frequently involve the lip when they arise in the upper aerodigestive tract.
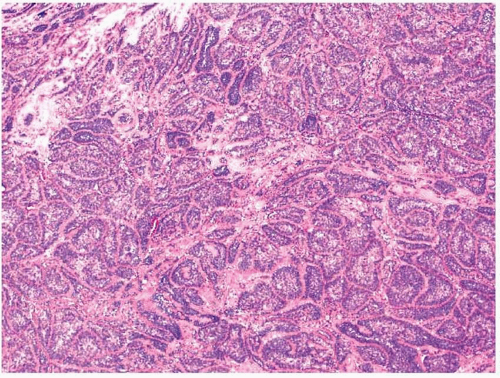
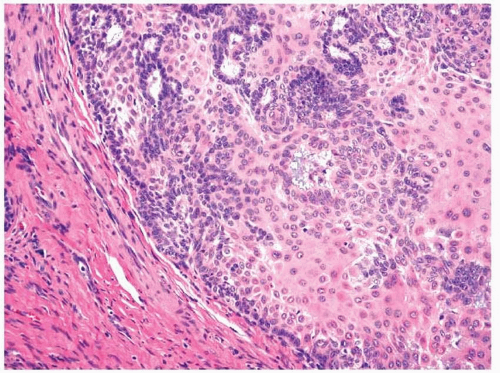
6Grossly, basal cell adenomas are well circumscribed.
26 Histologically, they are composed of basaloid cells that grow as somewhat organoid nests (the solid pattern), trabeculae, and tubules (
Fig. 6.7, e-
Figs. 6.15 and
6.16).
6,26,27,28 and
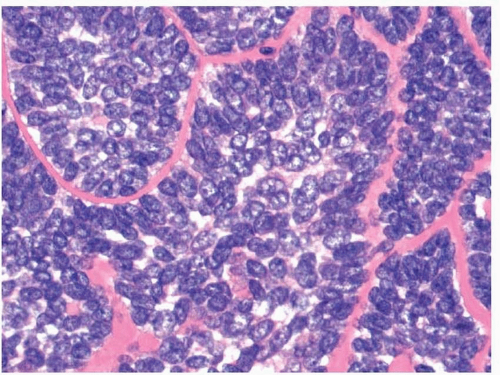
29 A variable amount of moderately cellular stroma is present between the aggregates of basaloid cells. The basaloid cells themselves are bland cytologically and have scant cytoplasm (
Fig. 6.8). Nuclear palisading is usually noted at the periphery of the epithelial structures, and some cells, particularly in the centers of the cell aggregates, may have more abundant, eosinophilic cytoplasm and show overt squamous differentiation. Lumina may be seen within the epithelial nests and trabeculae and are often lined by columnar ductal cells. Some cases may have hyaline material surrounding the groups of basaloid cells (membranous-type or dermal analogue tumor). Immunohistochemically, all the cells will show immunoreactivity with antibodies to keratins. Cells lining the apparent lumina stain most intensely.
30 Conversely, antibodies to S100 protein, SMA, and p63 highlight the peripheral cells that are juxtaposed to the connective tissues (e-
Fig. 6.17). p63 will also highlight areas of squamous differentiation. KIT (CD117) expression can be seen with both basal cell adenomas and adenocarcinomas.
31Basal cell adenomas must be distinguished from other basaloid neoplasms such as basaloid squamous cell carcinomas, basal cell adenocarcinomas, and adenoid cystic carcinomas. Basaloid squamous cell carcinomas are high-grade, infiltrative malignancies with numerous mitotic figures and severe cytologic atypia. Basal cell adenocarcinomas are primarily distinguished from adenomas by their infiltrative borders, and thus, the two cannot usually be distinguished on small biopsy specimens. Adenoid cystic carcinomas are highly infiltrative, typically have perineural invasion, and many have somewhat higher grade cytologic features. Furthermore, a cribriform growth pattern is not often seen with basal cell adenomas. Aside from the membranous type, basal cell adenomas do very well and almost never recur after adequate resection.
6
Papillomas
Papillary neoplasms of the salivary glands that cannot better be classified as other salivary gland-type neoplasms occur predominantly within the seromucinous glands of the upper aerodigestive tract. These include inverted papillomas, intraductal papillomas, and the rare sialadenoma papilliferum.
32 These lesions are all benign and do not develop into malignancies.
Inverted papillomas occur most frequently in the mouth, either at the lip or beneath the buccal mucosa.
32,33 These lesions present as nodules or swellings that typically measure approximately 1 cm in size. Grossly, they appear well circumscribed. Microscopically, these tumors appear to involve a large duct that may be seen to be in continuity with the surface epithelium (e-
Fig. 6.18). The duct is filled and expanded by a papillary
proliferation of predominantly squamous epithelium with scattered mucous cells that is frequently covered by columnar cells (e-
Fig. 6.19). This squamous epithelium shows maturation without atypia and usually does not keratinize (
Fig. 6.9). True infiltration of the stroma should not be seen and if identified should raise the question of a malignancy.
Intraductal papillomas also most frequently involve the lip or buccal mucosa.
32 The lesions present as swellings or nodules and usually measure about 1 cm in size. Microscopic examination shows a large duct lumen distended by arborizing papillae that are lined by a single layer of cuboidal to columnar epithelium with occasional mucous cells, all devoid of cytologic atypia.
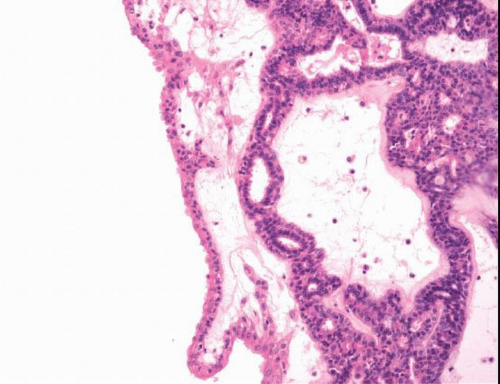
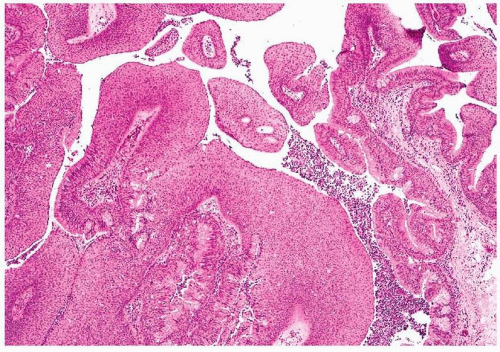
Sialadenoma papilliferum is extremely rare and most often involves the palate of middle-aged to older individuals.
32,34 Grossly, the lesions usually appear somewhat verrucoid or papillary. The papillary structures are covered at the tips by a thickened and often keratotic squamous epithelium (
Fig. 6.10). Lining the sides of these papillae and separating one from another is ductal epithelium that is often two cells thick (e-
Figs. 6.20 and
6.21). These epithelial cells may appear somewhat oncocytic and can show tufting. The ducts extend into the stroma and branch. Some degree of chronic inflammation is usually noted within the stroma.
Other Benign Neoplasms
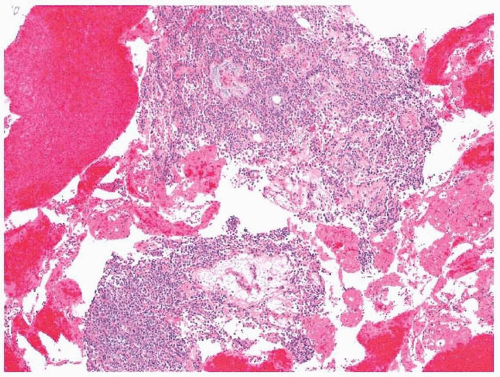
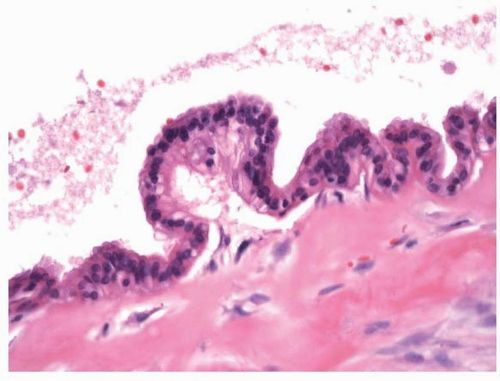
Cystadenomas represent between 5% and 10% of benign salivary glandtype neoplasms of the upper aerodigestive tract and often involve the lips, buccal mucosa, and palate.
5 The age range of patients with these
lesions is large, and about twice as many occur in women. Nodular and cystic spaces can be seen on cut section.
6,35 Histologically, the cysts are lined by a cuboidal or columnar epithelium (
Fig. 6.11, e-
Fig. 6.22). Mucinous, oncocytic, and squamous epithelia have all been described. The cytologically bland epithelium varies in thickness and often forms papilla. Some cystadenomas have been noted to involve the supraglottic
larynx. Here, they are composed of bland oncocytic epithelium, often with papillae.
36,37
Other benign salivary gland-type tumors described in the upper aerodigestive tract include
sebaceous adenomas and oncocytic proliferations, including
oncocytomas.38,39 Lesions similar in appearance to
Warthin tumors have also been described.
40 These tumors share the histologic features of their counterparts in the major salivary glands.