Germ Cell Tumors
It is extremely uncommon for extragonadal germ cell tumors to involve the head and neck and even more uncommon for them to actually arise from the upper aerodigestive tract. Tumors reported to involve this area include teratomas (and dermoids), yolk sac tumors (endodermal sinus tumors), choriocarcinomas, and teratocarcinosarcomas. Mixed tumors with teratomatous and yolk sac components have also been described. Definitive, concise diagnosis will require assessment of the entire tumor, and thus, one should be careful when diagnosing small biopsies too specifically.
TERATOMA
Teratomas are germ cell neoplasms that recapitulate the normal immature and mature tissues that are derived from the three germinal layers of endoderm, mesoderm, and ectoderm. In the head and neck, these tumors occur in both sexes and are almost always identified in infants or young children.1,2,3,4 and 5 They have been described within the nasal cavity, nasopharynx, oropharynx, and mouth. When they are very large, they may be associated with stillbirth. If a malignant component is not identified (somatic malignancy or yolk sac tumor) and the tumor is resectable, both immature and mature teratomas tend to behave well and most patients survive, free of recurrences.3,5
Microscopically, the tumors may show mature or immature differentiation or a mixture of the two. When immature differentiation is present, a prominent neuroepitheliomatous component may be noted, and it is important to distinguish these tumors from neural or neuroectodermal malignancies that can be found in the upper aerodigestive tract.2 Careful attention should be paid in order to identify other germ cell components, especially elements of yolk sac tumor or somatic malignancy.
The diagnosis of a mature teratoma is usually straightforward; however, nonneoplastic lesions such as glial heterotopia and hairy polyps need to be
excluded; this can be done by identifying endodermally, mesodermally, and ectodermally derived tissues.2 Abundant maturing, stratified squamous epithelium is usually present with juxtaposed dermal appendages. Neural tissue, fat, muscle, cartilage, and bone all may also be seen (Fig. 10.1, e-Fig. 10.1), as may epithelium that shows respiratory or gastrointestinal differentiation.
excluded; this can be done by identifying endodermally, mesodermally, and ectodermally derived tissues.2 Abundant maturing, stratified squamous epithelium is usually present with juxtaposed dermal appendages. Neural tissue, fat, muscle, cartilage, and bone all may also be seen (Fig. 10.1, e-Fig. 10.1), as may epithelium that shows respiratory or gastrointestinal differentiation.
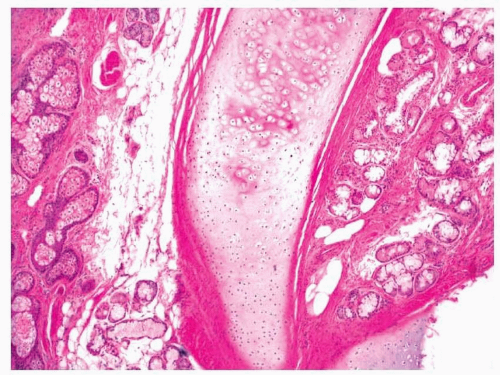 FIGURE 10.1 A mature teratoma with prominent cartilage formation. |
DERMOID CYSTS
Unlike teratomas, dermoid cysts are probably not neoplasms, but instead represent developmental abnormalities.2,5 In the upper aerodigestive tract, the lesions are usually located in the nasal cavity or in the floor of the mouth. Most patients are newborns or young adults. The tumors are composed of only ectodermally and mesodermally derived tissues and, as such, usually form large cystic structures lined by a maturing, stratified squamous epithelium replete with dermal appendages (Fig. 10.2). A small amount of surrounding fibrous tissue and adipose tissue is also usually present. Immature elements and malignancy should not be seen. With resection, the lesions infrequently recur.5
YOLK SAC TUMOR
Yolk sac tumors, also known as endodermal sinus tumors, can occur throughout the head and neck region and infrequently involve the upper aerodigestive tract, where they have been reported in the nose, paranasal sinuses, nasopharynx, oropharynx, and mouth.3,6 They occur mostly in children but have also been noted in middle-aged adults. The tumors show




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
