Nonneoplastic Lesions of the Oral Cavity
A vast array of nonneoplastic lesions arise in the mouth, including traumatic, infectious, inflammatory, and autoimmune processes. Given its location and its embryology, it is not surprising that this region can be affected by both cutaneous and gastrointestinal processes. Furthermore, it is the wet, moist, crushing portal of entry for food, drink, and air and thus is often traumatized and infected. This chapter discusses many of the nonneoplastic lesions that can be sampled within the oral cavity, along with differential diagnoses and the ancillary methods that are useful to distinguish these entities.
HETEROTOPIC TISSUES AND CHORISTOMAS
Because of the location of the mouth, its local relationship with other structures, and its role in embryogenesis, it can be affected by a number of heterotopic tissues or choristomas (Table 14.1). Heterotopic glial tissue, which most commonly involves the sinonasal area, can be present within the mouth, most often in the tongue (lingual glial choristoma).1 As in the sinonasal area (Chapter 13), these lesions are composed of mature glial tissue, mostly astrocytes with some ganglion cells. It is unclear whether such a tissue represents true heterotopia or, instead, a monodermic form of a mature teratoma. Regardless, the lesions do not recur following excision.
Lingual thyroid tissue can be present in the posterior dorsal region of the tongue at the foramen cecum, whence the normal thyroid migrates in utero.2 Here, the thyroid tissue usually presents as a painless mass. Sometimes patients are hypothyroid, and larger masses can cause obstruction. Histologically, lingual thyroid is composed of mature-appearing follicular thyroid tissue, intermixed to some degree with the skeletal muscle of the tongue (Fig. 14.1). Conventional thyroid neoplasia can develop in lingual thyroid tissue and should be excluded. Thyroglossal duct cysts are
also found at this site and will present as painful nodules when infected. Histologically, they are lined by ciliated columnar or squamous-type epithelium, with varying degrees of acute and chronic inflammation present (e-Fig. 14.1). Mature-appearing follicular thyroid tissue can be present but is not always seen. As with lingual thyroid tissue, conventional thyroid neoplasia should be excluded.
also found at this site and will present as painful nodules when infected. Histologically, they are lined by ciliated columnar or squamous-type epithelium, with varying degrees of acute and chronic inflammation present (e-Fig. 14.1). Mature-appearing follicular thyroid tissue can be present but is not always seen. As with lingual thyroid tissue, conventional thyroid neoplasia should be excluded.
TABLE 14.1 Heterotopic Tissues of the Mouth | |||||
|---|---|---|---|---|---|
|
Heterotopic gastrointestinal epithelium or enteric duplication cysts are found in the oral cavity, usually in the tongue or in the floor of the mouth. Most often these present as superficial or deep swellings within the tongue; however, there is a report of a child who would squirt others with a brown fluid from one of these lesions that connected to his tongue’s surface via a sinus tract.3 The cysts are lined by an enteric, glandular epithelium that is often intermixed with columnar, ciliated, and
squamous epithelia (Fig. 14.2, e-Fig. 14.2).4 Fundic-type epithelium with parietal cells is frequently seen. We have seen here rare duplication cysts that are associated with enteric-type adenocarcinomas.
squamous epithelia (Fig. 14.2, e-Fig. 14.2).4 Fundic-type epithelium with parietal cells is frequently seen. We have seen here rare duplication cysts that are associated with enteric-type adenocarcinomas.
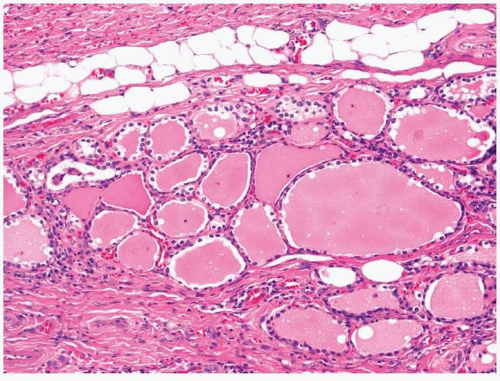 FIGURE 14.1 Lingual thyroid tissue. |
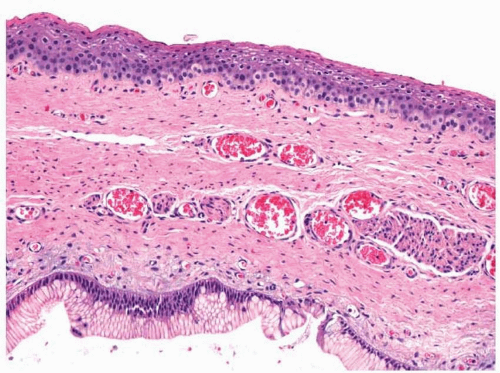 FIGURE 14.2 An enteric cyst immediately beneath the surface epithelium of the tongue. |
Ectopic sebaceous glands or Fordyce granules are sometimes found within the mouth.5 These lesions clinically appear as small, yellow papules, usually within the buccal mucosa (some consider the smaller buccal lesions to be normal). They vary considerably in number. Histologically, the papules are composed of sebaceous glands located within or immediately beneath the surface epithelium (Fig. 14.3). When present below the epithelium, ductal connections to the surface are usually not seen. Some have suggested that the formation of these lesions is related to inherited defects of mismatch repair proteins (hereditary nonpolyposis colon cancer).6
Other possible choristomas include osteomas and chondromas of the mouth (discussed in Chapter 12). The vestigial organ of Chievitz found in the area of the retromolar trigone is discussed in Chapter 1. Apparent tonsillar tissue can be present throughout the mouth and usually forms a mass lesion.
OTHER POSSIBLE CONGENITAL ABNORMALITIES
Other disparate congenital abnormalities afflict the mouth. These often present as mass lesions; however, some present secondary to disease to which the lesion has predisposed the patient (e.g., hemorrhage secondary to persistent caliber arteries and median rhomboid glossitis secondary to
candidiasis). Awareness of these lesions and their clinical features helps pathologists to distinguish them from other disease processes.
candidiasis). Awareness of these lesions and their clinical features helps pathologists to distinguish them from other disease processes.
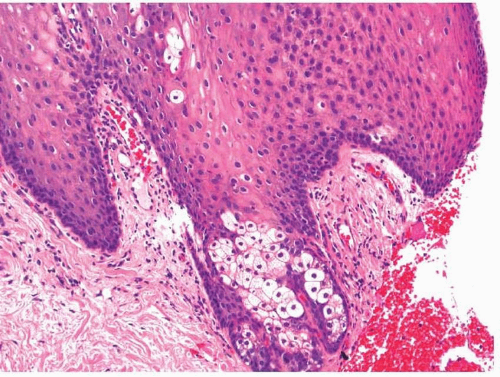 FIGURE 14.3 Fordyce granule. |
Palatal and gingival cysts can frequently be seen in infants and clinically appear as small (approximately 1 mm in size) yellow-white cysts at the midpalatal raphe at the junction of the hard and soft palates and along the alveolar ridge, respectively.7 Palatal cysts are composed of nests of epithelium surrounding the keratin. Gingival cysts are similar; however, nests of odontogenic epithelium are frequently noted within the surrounding stroma.
Median rhomboid glossitis is believed by some to be a congenital lesion, the result of persistent tuberculum impar anterior to the foramen cecum.8 This theory, however, is debated and others believe it to be an atrophic change secondary to the relative decreased vascularity of the area, especially as the lesions are not noted in children.8 These are midline, rhomboid-shaped, flat, and erythematous areas of squamous epithelium anterior to the circumvallate papillae, devoid of papillae. Histologically, the lesions may or may not be keratotic and resemble pseudoepitheliomatous hyperplasia (Fig. 14.4, e-Fig. 14.3). Chronic inflammation is present to some degree in the surrounding stroma. This lesion is frequently associated with infection due to Candida and some patients improve with antifungal therapy.9 In such cases, keratosis is typically seen and fungus can be identified by special stains (e.g., Grocott’s methenamine silver or periodic acid-Schiff staining) (e-Fig. 14.4).
Some arteries in the lower lip fail to reduce in size as they approach the surface near the vermillion border.10 These have been termed as
caliber persistent arteries. These arteries are sometimes associated with ulceration of the surface epithelium and can, when traumatized, bleed significantly. Rarely, they are associated with squamous cell carcinoma, perhaps secondary to the chronic ulcer.
caliber persistent arteries. These arteries are sometimes associated with ulceration of the surface epithelium and can, when traumatized, bleed significantly. Rarely, they are associated with squamous cell carcinoma, perhaps secondary to the chronic ulcer.
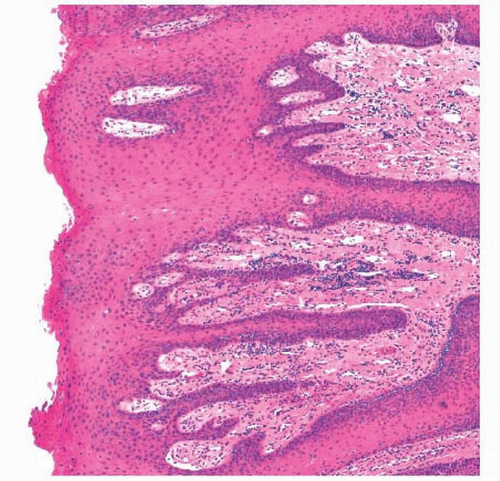 FIGURE 14.4 Median rhomboid glossitis. |
TRAUMA AND IATROGENIC PROCESSES
Not uncommonly, the mouth is traumatized. Acute traumatic lesions are seldom sampled, as their etiologies are rarely in question. Chronic traumatic lesions often have a nonspecific clinical appearance and may be sampled. The most common of these lesions is likely the traumatic fibroma. These fibromas along with their numerous alternative designations are discussed in Chapter 11. Osseous and cartilaginous metaplasias, secondary to chronic trauma or inflammation, are discussed in Chapter 12.
Inflammatory papillary hyperplasia and fibrous hyperplasia are both believed to be secondary to chronic trauma.11 Inflammatory papillary hyperplasia is associated with denture use and most often involves the hard palate. Some have suggested that infection due to Candida may play a role in the development of this condition.12 Clinically, patients present with numerous, red papillary or verrucoid lesions. Microscopically, numerous papillary growths are covered by thickened and parakeratotic squamous epithelium, with some degree of pseudoepitheliomatous hyperplasia, often with the formation of small keratinous cysts (Fig. 14.5).11 The stromal tissue is usually edematous and contains a lymphoplasmacellular
infiltrate (e-Fig. 14.5). Calcification or even cartilaginous or osseous metaplasia can be present. The underlying seromucinous glands may be atrophic and fibrotic. Small mucoid pools can be seen, which, together with the pseudoepitheliomatous hyperplasia and keratinous cysts, can lead one to consider mucoepidermoid carcinoma in the differential diagnosis.
infiltrate (e-Fig. 14.5). Calcification or even cartilaginous or osseous metaplasia can be present. The underlying seromucinous glands may be atrophic and fibrotic. Small mucoid pools can be seen, which, together with the pseudoepitheliomatous hyperplasia and keratinous cysts, can lead one to consider mucoepidermoid carcinoma in the differential diagnosis.
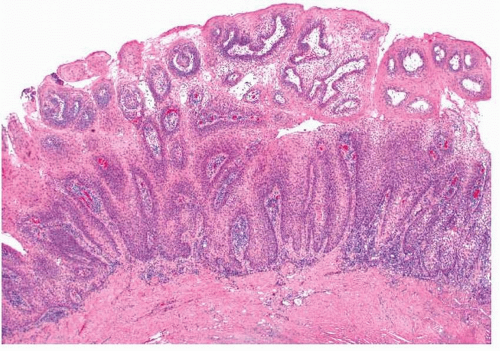 FIGURE 14.5 Inflammatory papillary hyperplasia of the palate. |
The diagnosis of fibrous hyperplasia is generally used to connote traumatic fibrous lesions of the mouth and is synonymous with oral fibroma. These lesions can show a vast range of reactive histologic changes. Aside from cartilaginous and osseous metaplasias, calcification, and cementum formation, some lesions will have many multinucleated giant cells (peripheral reparative giant cell granuloma). These are often quite numerous and resemble osteoclasts.13
Traumatic ulcerative granuloma is an uncommon lesion that can be clinically confused with malignancy. This lesion has acquired a number of appellations, mostly reflecting its presumed etiology and histology (e.g., eosinophilic ulcer, oral traumatic granuloma, ulcerative eosinophilic granuloma, and Riga-Fede’s disease).14,15,16,17 and 18 It develops rapidly in either sex and at any age and is believed to be secondary to trauma, particularly crush injury. Although the lesions frequently involve the lateral or dorsal portion of the tongue, they arise at all locations within the mouth.17,18 Most cases clinically present as ulcers; however, some are raised and exophytic.15
The surface of the traumatic ulcerative granulomas is typically covered by a fibrinopurulent exudate (Fig. 14.6).14,15 and 16,18 A dense mixed inflammatory infiltrate, rich in eosinophils, extends deep into the submu-cosa
and is intermingled with skeletal muscle fibers (e-Fig. 14.6). Other inflammatory cells include lymphocytes, macrophages, and neutrophils. Occasionally larger, atypical mononuclear cells are present (Fig. 14.7). These large cells frequently react with antibodies to CD30, a feature that led some to believe that these lesions were lymphoproliferative disorders
(e-Fig. 14.7).19 Molecular studies have failed to reveal clonality through the analysis of both T-cell receptor and immunoglobulin genes.20 This, together with the benign behavior of these tumors, has led most to conclude that these are nonneoplastic, reactive lesions.
and is intermingled with skeletal muscle fibers (e-Fig. 14.6). Other inflammatory cells include lymphocytes, macrophages, and neutrophils. Occasionally larger, atypical mononuclear cells are present (Fig. 14.7). These large cells frequently react with antibodies to CD30, a feature that led some to believe that these lesions were lymphoproliferative disorders
(e-Fig. 14.7).19 Molecular studies have failed to reveal clonality through the analysis of both T-cell receptor and immunoglobulin genes.20 This, together with the benign behavior of these tumors, has led most to conclude that these are nonneoplastic, reactive lesions.
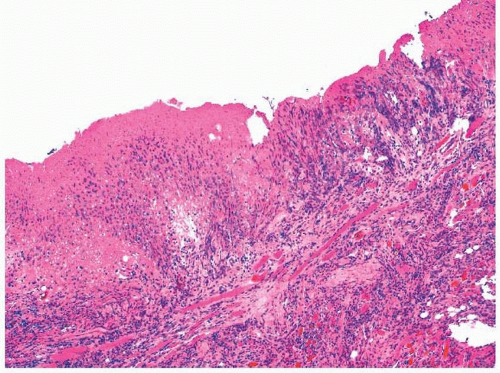 FIGURE 14.6 A traumatic ulcerative granuloma. |
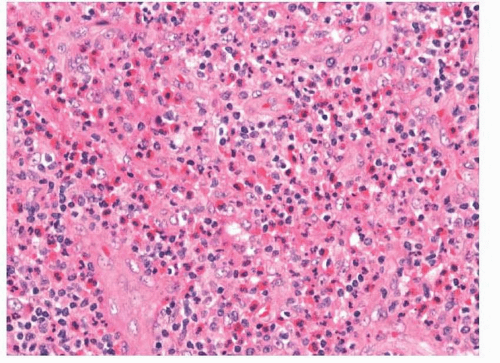 FIGURE 14.7 Eosinophils with occasionally large lymphocytes seen in a traumatic ulcerative granuloma. |
Because of their growth pattern and histologic features, traumatic eosinophilic granulomas must be distinguished from malignancies. Most often, anaplastic large cell lymphomas or Langerhans cell histiocytosis is considered in the differential diagnosis. Aside from the clinical presentations, these lesions can usually be distinguished by immunohistochemistry. The atypical mononuclear cells do not react with antibodies to S100 protein or CD1a as would the neoplastic cells of Langerhans cell histiocytosis. They also do not react with antibodies to anaplastic lymphoma kinase (ALK1).
Gingival fibromatosis or hyperplasia can result from the use of certain drugs, including phenytoin, cyclosporine, and nifedipine.21,22 These apparently reactive conditions develop within a few months of therapy with the inciting medication and may be related to individual patient’s dental hygiene. Clinically, the lesions begin with enlargement of the interdental papillae. These growths eventually become lobular and extend both labially and lingually. In advanced disease, teeth are often covered and displaced by the lesions. Histologically, the squamous epithelium is hyperplastic, with some degree of keratosis and elongated rete pegs. Fibroblasts proliferate within the underlying connective tissue and produce abundant collagen.
Patients who receive allogeneic bone marrow transplants or, uncommonly, those who receive solid organ transplants or even blood transfusions can develop graft-versus-host disease.23 Acute graft-versus-host disease develops within days to weeks of bone marrow transplantation. Clinically, patients present with variable amounts of erythema that can progress to a widespread blistering disease. The lesions progress histologically from focal basal cell vacuolar change to basal cell dyskeratosis to subepithelial cleft formation to the formation of bullae. A mononuclear perivascular infiltrate of variable degree is seen within the upper lamina propria and exocytosis is usually present, especially as the histologic changes worsen.
Chronic graft-versus-host disease develops in about half of adults and about 20% of children months to years after bone marrow transplantation.23,24 and 25 Clinically, the lesions often appear similar to those of oral lichen planus with linear white stria or ulcers. Patients also typically are noted to have xerostomia. A lichenoid infiltrate of mononuclear cells is present with exocytosis, basal cell vacuolization, cell death, and, in worse cases, bullae (Fig. 14.8, e-Fig. 14.8). The seromucinous glands have prominent chronic inflammation, with degeneration and fibrosis. They are sometimes cystically dilated.
Other traumatic or iatrogenic lesions have also been reported. Some authors have shown that adipose tissue from the buccal pad can herniate
into the mouth with trauma and erroneously be diagnosed as a lipoma (traumatic pseudolipoma).26 Mucositis secondary to chemotherapy or radiation therapy is rarely biopsied and is instead usually diagnosed clinically.27 It is associated with ulceration and nonspecific histologic features (see Chapter 4). Thermal injury of the mouth is common but rarely sampled. The histology is similar to that seen with burns of other squamouscovered surfaces and depends on the severity of the burn. Necrosis of the epithelial and subepithelial tissues can be seen with the formation of subepithelial bullae.
into the mouth with trauma and erroneously be diagnosed as a lipoma (traumatic pseudolipoma).26 Mucositis secondary to chemotherapy or radiation therapy is rarely biopsied and is instead usually diagnosed clinically.27 It is associated with ulceration and nonspecific histologic features (see Chapter 4). Thermal injury of the mouth is common but rarely sampled. The histology is similar to that seen with burns of other squamouscovered surfaces and depends on the severity of the burn. Necrosis of the epithelial and subepithelial tissues can be seen with the formation of subepithelial bullae.
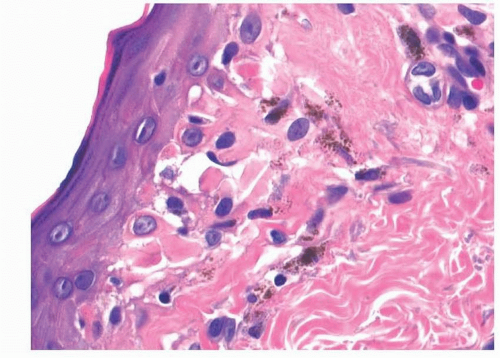 FIGURE 14.8 Chronic graft-versus-host disease with basal cell vacuolization and necrosis. |
INFECTIOUS DISEASE
The mouth can be affected by a great variety of infectious diseases, especially in patients who, for one reason or another, are immunocompromised. Infectious lesions may appear inflammatory or ulcerative. They can also mimic neoplastic masses or neoplastic intraepithelial proliferations (e.g., leukoplakia). Ancillary testing is usually helpful for identifying causative agents. The role of human papillomavirus in oral pathology is discussed in the chapters dealing with squamous neoplasia (Chapters 2, 3, 4 and 5).
Hairy leukoplakia secondary to infection due to Epstein-Barr virus (EBV) most frequently occurs in immunocompromised individuals; however, it can occasionally develop in patients who appear to be immunocompetent.28,29 and 30 Clinically, these lesions are white, broad, and flat to slightly raised. The surface typically appears corrugated or “hairy.” While the lesions most often involve the lateral or ventral surfaces of the tongue,
they can develop anywhere within the mouth. Unlike infections secondary only to Candida (i.e., thrush), abrasion will not dislodge the plaque material.29
they can develop anywhere within the mouth. Unlike infections secondary only to Candida (i.e., thrush), abrasion will not dislodge the plaque material.29
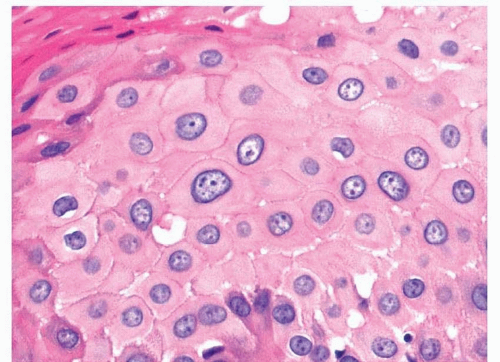 FIGURE 14.9 The cytoplasm of the squamous cells in hairy leukoplakia will appear glassy. |
Histologically, the squamous epithelium is acanthotic with parakeratosis (e-Fig. 14.9).29,30 Individual superficial squamous cells have optically clear cytoplasm with somewhat compressed, darkened nuclei (Fig. 14.9). Within these cells, the chromatin often appears marginated and intranuclear inclusions are commonly seen. The squamous epithelium is often not inflamed, and only mild chronic inflammation is present in the lamina propria. In situ hybridization for EBV-encoded RNA is helpful, as the affected squamous epithelium will contain virus. Staining for fungal or bacterial organisms may demonstrate secondary colonization of the superficial epithelium.
Other herpes viruses can infect the oral mucosa including the herpes simplex viruses (HSV-1 and HSV-2) and varicella zoster, as well as cytomegalovirus.31 Infections associated with simplex viruses and varicella cause painful vesicles that eventually ulcerate. Primary infections with HSV-1 manifest as a gingivostomatitis. Most reactivations in immunocompetent patients are labial, although intraoral recurrences also develop. Immunocompromised patients can have severe intraoral disease either at the time of primary infection or at the time of reactivation. The histology of these lesions is similar to that seen in other squamous epithelia. The mucosa will be eroded and ulcerated with a diffuse mixed inflammatory infiltrate. Telltale signs of herpes infection include single and multinucleated epithelial cells with Cowdry type A and B intranuclear
inclusions (Fig. 14.10).31 Ductal cells of the minor salivary glands can also be infected. Immunohistochemistry with antibodies to specific types of herpes viruses will confirm the diagnosis, if needed. The large intranuclear and intracytoplasmic inclusions of cytomegalovirus are typically found within lesional endothelial cells, as this virus does not usually infect squamous epithelium (e-Fig. 14.10).31
inclusions (Fig. 14.10).31 Ductal cells of the minor salivary glands can also be infected. Immunohistochemistry with antibodies to specific types of herpes viruses will confirm the diagnosis, if needed. The large intranuclear and intracytoplasmic inclusions of cytomegalovirus are typically found within lesional endothelial cells, as this virus does not usually infect squamous epithelium (e-Fig. 14.10).31
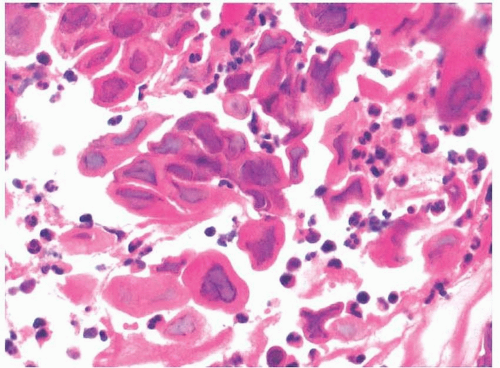 FIGURE 14.10 Characteristic intranuclear inclusions seen in lingual herpes. |
The oral cavity can be involved in all stages of syphilis.32




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
