(1)
Department of Ophthalmology, St. Thomas’ Hospital, London, UK
6.1 Introduction
6.1.3 Natural History
6.2.1 Anterior Segment Signs
6.2.2 Signs in the Vitreous
6.2.5 Macula Off or On
6.3 Surgery
6.3.1 Flat Retinal Breaks
6.3.2 Retinal Detachment
6.3.3 Pars Plana Vitrectomy
6.3.4 The Non-drain Procedure
6.3.6 Pneumatic Retinopexy
6.4 Success Rates
6.9.1 Diplopia
6.9.3 Infection
6.9.4 Cosmesis
6.9.5 Irritation
6.10 Summary
Abstract
Strictly speaking, ‘retinal detachment’ is a misnomer. The term denotes separation of the neuroepithelium from the pigment epithelium (rather than detachment of the retina, which consists of the neuroepithelium and the RPE, from the choroid) and therefore implies re-establishment of the space between the original layers of the embryonic optic cup. The incidence is approximately 10/100,000 (Saidkasimova et al. 2009), and presentation is more common in affluent populations and possibly males. Black races are probably less affected than white (Day et al. 2010).
Electronic supplementary material
The online version of this chapter (doi:10.1007/978-3-642-31872-6_6) contains supplementary material, which is available to authorized users.
6.1 Introduction
Strictly speaking, ‘retinal detachment’ is a misnomer. The term denotes separation of the neuroepithelium from the pigment epithelium (rather than detachment of the retina, which consists of the neuroepithelium and the RPE, from the choroid) and therefore implies re-establishment of the space between the original layers of the embryonic optic cup. The incidence is approximately 10/100,000 (Saidkasimova et al. 2009), and presentation is more common in affluent populations and possibly males. Black races are probably less affected than white (Day et al. 2010).
The most common cause of retinal detachment is the formation of a ‘break’ or full-thickness discontinuity in the neuroepithelium with recruitment of fluid from the vitreous cavity into the subretinal space via the break, creating ‘rhegmatogenous retinal detachment’. Classically, breaks are subdivided into ‘tears’ (secondary to dynamic vitreoretinal traction) and ‘holes’ (secondary to localised retinal disintegration or atrophy).
6.1.1 Tears with Posterior Vitreous Detachment
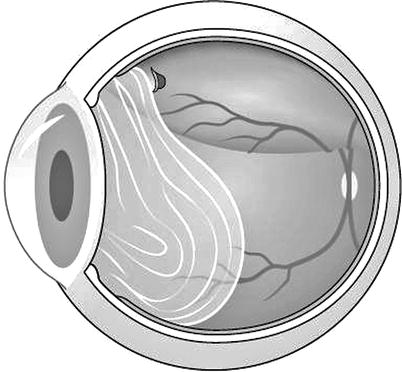
Fig. 6.1
A retinal tear occurs when the vitreous separates from the retina posteriorly. The vitreous produces traction on its attachments to the retina thereby tearing the retina, producing a retinal break
Most retinal tears occur in association with posterior vitreous detachment by the operation of ‘dynamic vitreous traction’ Fig. 6.1). This term denotes the transmission of rotational energy (generated by saccadic contraction of the extraocular muscles) to the vitreous gel through the coats of the eye (sclera, choroid and retina). Whilst the vitreous remains attached to the retina, this energy transmission is dispersed throughout the total area of vitreoretinal contact. After posterior vitreous detachment, however, the forces produce considerable movement in the posterior gel. The vitreous base provides the centre of energy, whilst the posterior vitreous responds to the energy by accelerating into a violent movement.
If there is any area of ‘abnormal’ adhesion of the retina to the gel, the movement of the gel exerts considerable dynamic traction on the retina sometimes producing a U-shaped tear of the retina. The base of the tongue of retina, which produces the ‘U’, is anteriorly placed because the vitreous separates first posteriorly tearing the retina at a point of adhesion and the action of the vitreous extends the tear anteriorly towards the vitreous base. If the flap of the tear separates completely from the retina, the piece of avulsed neurosensory retina is seen attached to the posterior vitreous membrane as an operculum and a round tear is produced. Ninety percent of tears are present at the initial examination after a symptomatic PVD. Approximately 10 % are not seen at the initial presentation or develop later therefore a follow-up examination is recommended (Sharma et al. 2004b).
If the symptoms are of a few days’ duration, review in 1 week; if longer, review at 4–6 weeks.
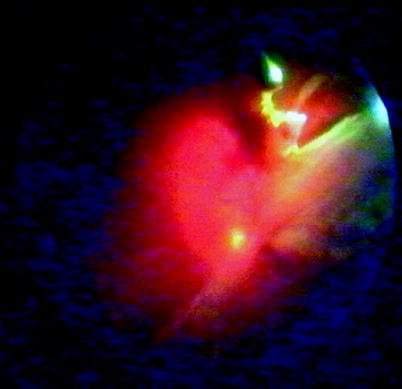
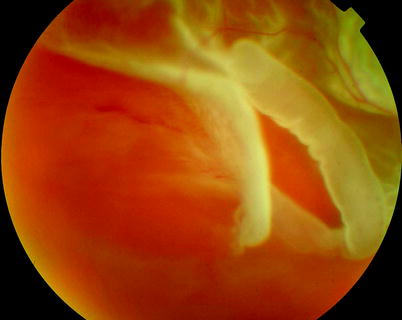
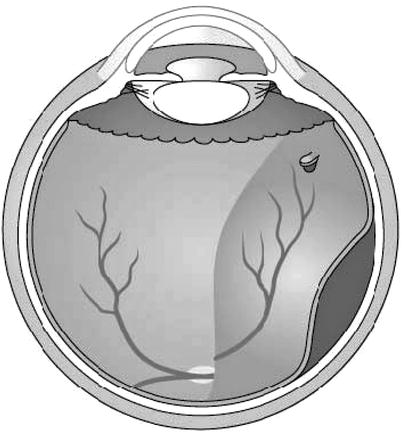
Fig. 6.2
A clot of fibrin can be seen extending from an artery torn by the action of PVD in tearing the retina
Fig. 6.3
A large retinal tear
Haemorrhage from rupture of a blood vessel that crosses a U tear may produce a ‘tadpole’ floater or shower of floaters. Floaters may also be seen from the posterior vitreous detachment and photopsia (flashing lights) from traction on the retina.
The vitreous is adherent to the rim of lattice lesions. U tears in lattice therefore tear along the posterior border of the lattice and then extend anteriorly around the edge of the lesion.
Multiple tiny flap breaks at the posterior border of the vitreous base are particularly associated with aphakia or pseudophakia. The reasons for this are not clear, but cataract extraction alters the architecture of vitreous through loss of the posterior bulge of the crystalline lens into the anterior vitreous.

Fig. 6.4
A large U-shaped tear
6.1.2 Breaks Without Posterior Vitreous Detachment
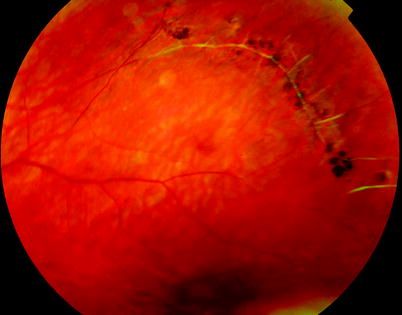
Fig. 6.5
Lattice degeneration
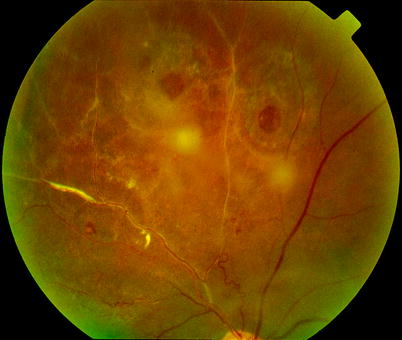
Fig. 6.6
These round breaks have overlying opercula of retina (seen out of focus) suggesting previous vitreal traction; these breaks are at low risk of causing retinal detachment

Fig. 6.7
Round holes are present in an inferior retina in this patient. These can be ignored if they are asymptomatic as the chances of their progression to retinal detachment are probably less than 1/200
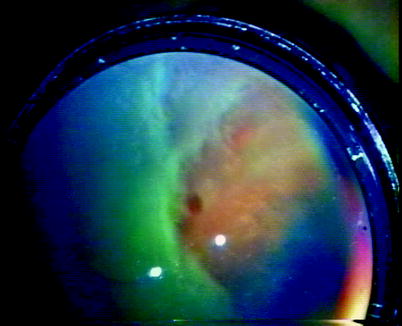
Fig. 6.8
A round hole is visible on indentation of this eye

Fig. 6.9
A round hole seen on a slit-lamp camera
Rhegmatogenous retinal detachment may be produced without posterior vitreous detachment by atrophic retinal holes often in young myopic patients (these patients are more likely to be female, 64 %, with bilateral pathology in 83 % (Ung et al. 2005)) or by retinal dialysis at the ora serrata (see Chap. 6). Both conditions usually produce a slow onset of retinal detachment which may only be noticed during coincidental examination of the eye or symptomatically by the patient when the fovea detaches. Atrophic holes are often equatorial, associated with lattice degeneration, myopia and found in 20–40-year-old patients. The vast majority will not cause retinal detachment, and prophylactic therapy is generally regarded as unnecessary. Recruitment of fluid in round hole detachment probably occurs by connection of the hole to lacunae in the vitreous. This may cause a stepped increase in the detachment with multiple pigmentary demarcation lines in a chronic-looking retinal detachment.
Retinal dialyses are ellipsoid separations of the retina at the ora serrata that are usually situated inferotemporally. They differ from U tears because the gel is attached to the posterior rather than the anterior margin of the break and posterior vitreous detachment is absent.
6.1.3 Natural History
Most retinal detachments if untreated will progress to totality or near totality. The visual loss is profound, and potential recovery of vision by surgery reduces as the weeks go by.
The accumulation of SRF in the periphery seems to be important for the development of loss of vision as patients with RRD lose more vision in comparison to CSR for the same foveal.
Initially, the retina is thickened and less transparent than normal.
If the retina remains detached for many months, it becomes progressively atrophic.
The longer the retina remains detached, the higher the risk of a scarring response, proliferative vitreoretinopathy (see PVR, Chap. 8).
Chronic RRD
In a long-standing subtotal retinal detachment a ‘high-water mark’ or pigment demarcation line of retinal pigment hyperplasia may appear, which sometimes limits further extension of the detachment. Multiple high-water marks in detached retina indicate recurrent extension of the detachment and are more often seen in slower onset detachments associated with round holes or dialyses. Other indices of long-standing detachment include retinal cysts (secondary retinoschisis) (Marcus and Aaberg 1979), oxalate crystals on the macula (Ahmed et al. 1998) and peripheral neovascularisation.
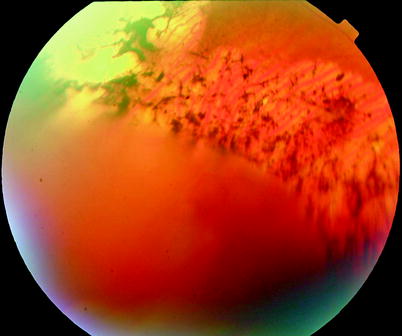
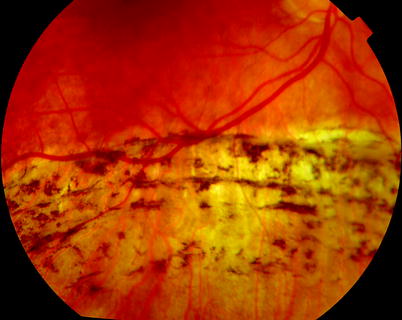




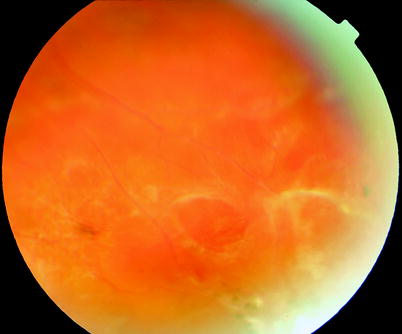


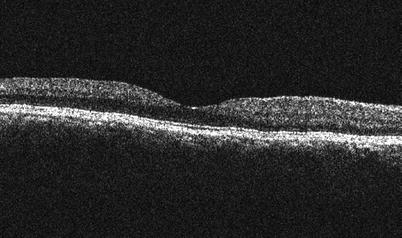



Fig. 6.10
A demarcation line is shown around this retinal detachment which has been chronic in nature. It is unlikely that the retinal detachment will extend through this demarcation, and therefore surgery is not required
Fig. 6.11
A RRD may spontaneously reattach leaving RPE hypertrophy and atrophy. The arcs of pigment hyperplasia in this patient suggest that the RRD advanced, stopped and advanced again a phenomenon seen in vitreous-attached RRD. One theory for this observation is that lacunae of fluid vitreous empty through a retinal hole providing fluid for the subretinal space and advancement of the RRD edge. The RRD does not move again until another lacunae form and empty through a hole. In the meantime, RPE hyperplasia occurs at the juncture of the detached and attached retina creating arcs of pigmentation. Spontaneous reattachment may occur when vitreous gel plugs the retinal hole and the RPE is able to clear the SRF
Fig. 6.12
A retinal cyst is a sign of longevity of retinal detachment, usually over 1 year. In this eye, two retinal cysts are inferiorly placed
Fig. 6.13
A retinal cyst has formed in the macular area in this patient with chronic RRD
Fig. 6.14
Subretinal bands in a chronic RRD, these are commoner in vitreous-attached RRD, e.g. retinal dialysis or round hole (young myope) RRD
Fig. 6.15
The fovea was in place in this chronic RRD with subretinal bands. The retinal hole appeared to be plugged with vitreous perhaps preventioning further fluid vitreous entry through the break and further spread of the RRD (see Fig. 6.16)
Fig. 6.16
See previous figure
Fig. 6.17
If a RRD spontaneously reattaches, retinal pigment epithelial changes may occur
Fig. 6.18
Tiny white flecks can be seen in the fovea in patients with chronic retinal detachment. These are signs of oxalosis, a secondary complication from the chronicity of the retinal detachment
Fig. 6.19
A tiny speck of oxalate can be seen on the foveal surface on OCT (greyscale image)
Fig. 6.20
Some long-standing RRDs, e.g. from retinal dialysis, will show white spots on the outer retina. These fade after reattachment of the retina (see Fig. 6.21)
Fig. 6.21
See previous figure
Fig. 6.22
The arrow indicates a point of adhesion which appears to have stopped the progress of a chronic inferior RRD
Very rarely, the retina reattaches spontaneously sometimes leaving pigmented chorioretinal changes, but most often surgery is required to reattach the retina. After successful surgery, the rods recover their function surprisingly well, and any visual field defect disappears. If the fovea has been involved, recovery of function of the cones is good if the detachment is treated quickly (within 1 week of onset). After prolonged detachment of the fovea, central vision may be permanently impaired.
Descriptive statistics for a north European population (Laatikainen and Tolppanen 1985)
Mean age | 53 years |
Bilateral | 10 % |
Lattice degeneration | 15 % |
Total detachment | 17 % |
More than one break | 41 % |
No break found | 11 % |
More dialyses | <20 years old |
Tears = atrophic holes | 20–40-year-olds |
Predominantly tears | >40-year-old |
Bilateral simultaneous (Krohn and Seland 2000) | 2.3 % |
Risk to the Other Eye
Chance of RRD in the fellow eye later on is 12 % with a 12 % chance of requirement for retinopexy to a tear (Gonzales et al. 2004).
6.2 Clinical Features
The patient may experience symptoms of flashes and floaters (indicating posterior vitreous detachment with or without vitreous haemorrhage) followed by visual field loss. Some slow-onset retinal detachments will produce the symptom of a slow flashing light (often moving like a slow comet tail) lasting a few seconds and situated in the visual field appropriate to the leading edge of SRF. When the fovea detaches, there is loss of central vision, with the fovea just off the visual acuity may vary from 20/40 to 20/200. As the fovea lifts, the patient may experience distortion of vision. When the macula is fully detached, the vision may be 20/200 to hand movements.
6.2.1 Anterior Segment Signs
A few cells and some flare can be seen in the anterior chamber. Rarely a severe anterior uveitis occurs perhaps indicating a high risk of PVR. IOP is often lower than the fellow eye. Occasionally, a high IOP can be produced by blockage of the trabecular meshwork by the remnants of receptor outer segments (Schwartz’s syndrome) (Netland et al. 1994; Schwartz 1972). Iris neovascularisation has been described which reverses after resolution of the RRD (Tanaka et al. 1991).
6.2.2 Signs in the Vitreous
Retinal tear formation is usually associated with the release of retinal pigment epithelial cells into the vitreous cavity (see Chap. 3). The presence of pigment cells in the retrolental gel (Shafer’s sign) (Shafer et al. 2005) in a phakic eye strongly implies the presence of a retinal break. Differentiation of these cells into fibroblast-like cells and synthesis of new collagen within the gel and on the posterior hyaloid interface results in retraction and immobilisation of the gel. An early sign of this process is seen when the cells change from diffuse single cells to groups or ‘clumps’ of cells in the gel. Such changes are frequently associated with the proliferation and contraction of cellular membranes on the retinal surface in proliferative vitreoretinopathy (PVR). Vitreous haemorrhage may obscure the view of the retina and breaks. Suspect that any patient with vitreous haemorrhage of unknown aetiology has a retinal tear or detachment.
6.2.3 Subretinal Fluid Accumulation
Fig. 6.23
Fluid currents (arrows) from the vitreous cavity may contribute to the lifting of the retina in rhegmatogenous retinal detachment
Fig. 6.24
A break at 12 o’clock causes a total bullous RRD
Fig. 6.25
The retinal break in a bullous RRD is usually located 1–2 clock hours from the superior edge on the highest side
Fig. 6.26
The break in a non-bullous RRD is usually inferior and on the side of the highest retinal detachment upper edge
Fig. 6.27
Occasionally, a small anterior break will cause an inferior RRD by tracking SRF down the anterior retina
Separation of the neuroepithelium from the pigment epithelium occurs first in the immediate vicinity of the break. Progressively more subretinal fluid is recruited from the vitreous cavity (from the retrohyaloid space or from syneretic gel) increasing the area and elevation of retinal separation. Progression has been estimated at 1.8 disc diameters/day (Ho et al. 2006) so that fovea on patients can become fovea off by the time of surgery. If the globe is completely immobilised at an early stage, the retina may partially or even completely reattach suggesting that three mechanisms may be implicated.
Movement of the eye (and the resultant vitreous gel movement) causes extension of the retinal detachment through the action of dynamic vitreoretinal traction.
The movement of the gel induces fluid currents in the retrohyaloid space, which forcefully elevate the neurosensory retina (Hammer et al. 1986).
Gravity encourages spread of the subretinal fluid.
The last mechanism causes a pattern of spread of subretinal fluid first described by Lincoff that may be used by the surgeon to aid localisation of a retinal break (Lincoff and Gieser 1971).
A tear between the 11 and 1 o’clock causes a retinal detachment, which becomes total soon after its onset.
Tears above the horizontal meridian (3 to 9 o’clock) produce subtotal detachments. Fluid is recruited progressing downwards on the same side as the tear at first and then upwards on the opposite side of the disc (but to a level lower than that on the side of the tear).
Inferior subretinal fluid from a superior tear tends to separate partially into two bullae with a cleft or ‘cleavage’ of less elevated retina in the 6 o’clock meridian.
A break located below the horizontal meridian tends to accumulate fluid more slowly compared with that descending from above. The upper limits of the detachment form convex-curved edges on each side, the higher edge indicating the side of the break. Bullae are not seen with inferior breaks.
Occasionally, a small anterior and superior tear leaks fluid down the post-oral retina causing an inferior retinal detachment. Therefore, inferior retinal detachments can occur from both superior and inferior tears.
Subretinal fluid accumulates more quickly if fluid is recruited from the retrohyaloid space (e.g. via a U tear after posterior vitreous detachment) compared with breaks occurring without posterior vitreous detachment (e.g. atrophic holes and dialyses). In the latter, potential recruitment of fluid from syneretic gel may be limited by the size of the lacuna in the gel. As a retinal detachment progresses, the patient notices an increasing field defect corresponding to the detached area. Central vision is distorted and diminished as the fovea detaches.
6.2.4 Retinal Break Patterns in RRD
Breaks are more common temporally and superiorly than nasally or inferiorly in PVD-related RRD. See Chap. 7 for more details.
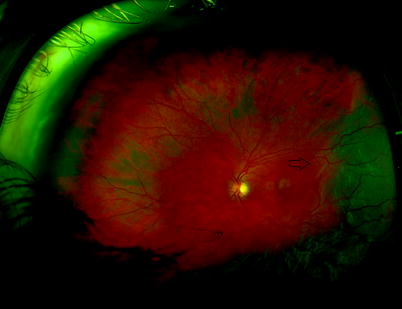
Fig. 6.28
A wide-angle view of the retina with an inferotemporal RRD, leading edge (arrow) close to the fovea
6.2.5 Macula Off or On

Fig. 6.29
A composite picture shows an RRD passing through the macula
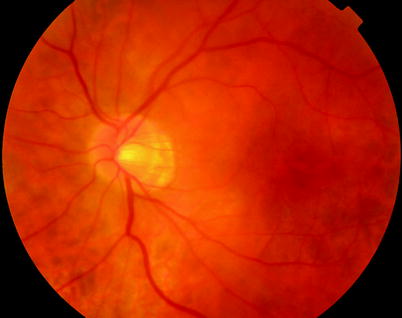
Fig. 6.30
It may not be obvious that the fovea is detached in which case OCT is useful (see Fig. 6.31)
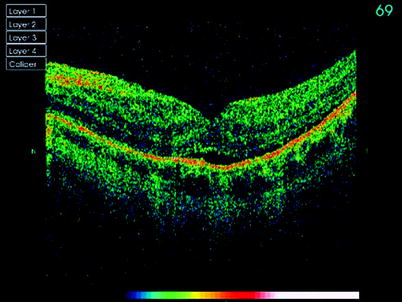
Fig. 6.31
See previous figure
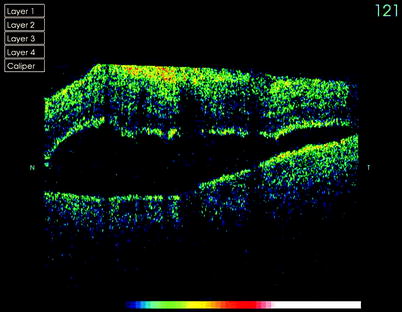
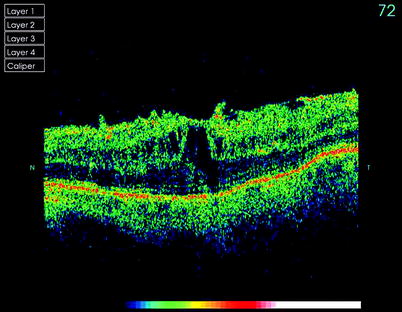
Fig. 6.33
Changes in the macula may be seen in association with inferior retinal detachment such as this with ERM and CMO. Ask the patient if the vision is worse in the morning or on lying supine in which case SRF may be moving into the subfoveal space (see Fig. 6.32)
When the fovea of the macula detaches (usually called macula off), the chances of return of full central vision are reduced particularly after the first week of detachment. As a ‘rule of thumb’, the number of days the fovea has been detached is the same as the urgency for performing the surgery; for example, if the fovea has been off for 1 day, perform the surgery within 1 day; if off for 2 days, perform surgery within 2 days. Of course the sooner, the better, but this rule helps the scheduling of surgery and appropriate use of theatre sessions.
Referral procedure for RRD
Condition | Characteristics | Referral | Why? |
|---|---|---|---|
RRD with PVD | Macula on | Immediate | Prevent macula detaching |
Macula off less than 1 week | 1–3 days | Macula should recover fully | |
Macula off 1–2 weeks | 1 week | Macula should recover well | |
Macula off 2–6 weeks | 1–2 weeks | Macula will show moderate recovery | |
Macula off >6 weeks | 2–3 weeks | Macula unlikely to recover well | |
RRD without PVD | 1–2 weeks | Slow progression |
Chance of 20/40 or better after fovea off retinal detachment (Hassan et al. 2002).
10 days or less | 71 % |
11 days to 6 weeks | 27 % |
More than 6 weeks | 14 % |
Macula off retinal detachment is more likely to suffer subtle changes in vision such as distortion postoperatively; therefore, it is preferable to avoid the detachment of the fovea by performing surgery on ‘macula on’ retinal detachment promptly, for example, within 24 h. Chronic retinal detachments (e.g. when the vitreous is attached) in which there is slow accumulation of subretinal fluid can be left longer before surgery. By posturing, a retinal break to the dependant portion of the eye accumulation of SRF can be reduced or even reversed, whilst the patient is waiting for surgery.
For a temporal hole in the left eye or a nasal hole in the right eye, the patient would be asked to lie with their left cheek down to the ground.
For a nasal hole in the left eye or a temporal hole in the right eye, the patient would be asked to lie with their right cheek down to the ground.
For a superior hole, the patient lies supine with no pillows and the foot of the bed raised.
For inferior holes, sit the patient upright.
6.3 Surgery
6.3.1 Flat Retinal Breaks
Retinopexy
If a patient presents with a retinal break which is at high risk of producing a retinal detachment (U tear, paravascular tear, operculated tear or dialysis) but has no subretinal fluid, then retinopexy is applied to prevent accumulation of fluid underneath the neurosensory retina (Gonin 1930). This can be applied as laser therapy around the break (usually in two rows around the circumference of the break) or by trans-scleral cryotherapy. Both methods produce damage to the neurosensory retina, to the retinal pigment epithelium and perhaps to Bruch’s layer and the choroid. The resultant reparative scar formation occurs in approximately 5–10 days and seals the layers of the retina together preventing fluid accumulation.
Cryotherapy
Cryotherapy employs the Joule-Thomson effect whereby expansion of certain gases, such as nitrous oxide or carbon dioxide, results in a reduction in temperature. The gas is compressed and then released through a small hole in a cryotherapy instrument tip, causing a rapid expansion of the gas and reduction in the temperature. Cryotherapy has the advantage that it can be applied trans-scleral without discernible damage to the conjunctiva, Tenon’s layer and the sclera if not used excessively whilst creating a freeze and therefore a scar in the retina.
It takes effect and has maximum adhesion in approximately 10 days but causes dispersion of retinal pigment epithelial cells into the vitreous giving an increased risk of PVR especially in the presence of U tears with curled edges or tears greater than 180° (Bonnet et al. 1996). Apply cryotherapy sparingly, usually one freeze in the centre of the break. Although this may increase the chance of RPE dispersion through the break, it is preferable to multiple freezes around the tear, which increase the pro-inflammatory effects of the treatment (and the risk of PVR) and the discomfort to the patient. Cryotherapy is very useful for anterior breaks which are difficult to laser because it allows simultaneous indentation; a single cryotherapy application is often a less traumatic experience for the patient than a difficult laser session.
Cryotherapy in the Clinic Setting
1.
Insert topical anaesthesia.
2.
Insert a lid speculum if required, sometimes not necessary.
3.
Give a localised injection of anaesthesia in the fashion of a peribulbar injection in the quadrant of the orbit with the retinal break. Warn the patient that they may experience some photopsia.
4.
Always check that the tip will freeze and unfreeze before applying to the eye (these machines are notoriously unreliable).
5.
Apply the cryotherapy tip trans-conjunctivally and use the tip to indent whilst observing with the indirect ophthalmoscope. Make sure you are visualising the tip and not the shaft of the cryotherapy probe when producing the indent; otherwise, the freeze will be posterior to the site that you are attempting to treat.
6.
Once you are under the break, start the freeze commence until the break has been surrounded with ice crystals; do not overdo the freeze, it only needs to encompass the break by the equivalent of two rows of laser.
7.
Provide topical postoperative antibiotics for a few days.
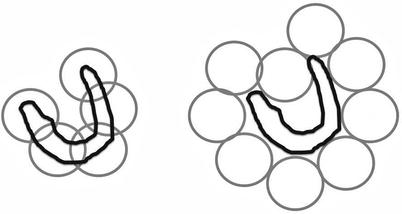
Fig. 6.34
Apply cryotherapy to a large tear as shown on the left, although this applies cryotherapy to the bare RPE in the tear; this is preferable to the increased number of burns required if the retina around the tear is treated as shown on the right
Complications:
Extraocular muscle injury causing diplopia, wait and the muscles will recover.
Eyelid injury, loss of pigmentation. Avoid freezing through the lid.
Subconjunctival haemorrhage or tearing of the conjunctiva.
An over-freeze causing a retinal tear and haemorrhage. You only need to see the retina freeze in the early stages not a severe freeze with massive ice crystal formation.
Never pull off a frozen tip as this may tear the sclera; be patient; before removing the tip, allow it to thaw.
Laser

Fig. 6.35
A tear has been treated with laser retinopexy
Argon, diode or visible spectrum diode laser induces tissue injury and therefore scarring, from thermal burns on the tissues (photocoagulation). Non-visible diode can cause a disproportionate injury to the choroid and must be used with care. The laser should extend anteriorly around the tear or if not possible should extend to the ora serrata. Argon laser therapy can be applied either by a contact lens with a slit lamp or by indirect ophthalmoscopy with indentation. Maximum adhesion is approximately 5 days and requires two rows of burns around a break for maximal adhesion. Trans-scleral diode laser has also been used (Haller et al. 1997).
Typical laser settings for argon green:
200–300-mW power
0.1–0.2-ms duration
Spot size 200–500 μm
Repeat interval 0.1 s
Laser in the Clinic Setting
Can be applied at the slit lamp using various contact lenses for posterior and equatorial tears (contact lenses have the advantage over noncontact fundus lenses of helping control eye movements during the laser session).
Can be applied with indirect ophthalmoscopy thereby allowing indentation for anterior breaks.
Apply laser of adequate power to produce a blanching spot.
Two rows 360° around the break or for very anterior breaks around the posterior and lateral borders of the break and up to the ora serrata.
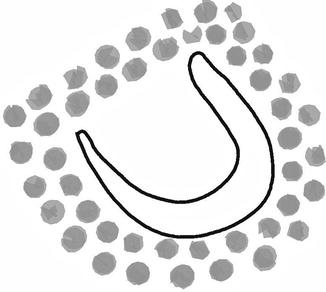
Fig. 6.36
Laser should be placed in two rows around a retinal tear as shown, laser the flat retina close to the edge of the tear
Fig. 6.37
If the retinal tear is close to the ora serrata, laser up to the ora serrata if you are unable to laser around the anterior edge of the tear
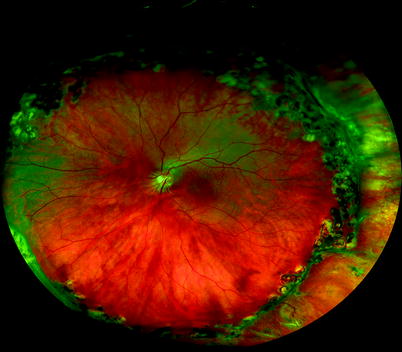
Fig. 6.38
360-degree laser has been applied to this RRD to try to prevent recurrence
Complications:
Retinal bleeding – Press on the eye to minimise.
Lens damage – Reduce the power.
Macular damage –Take care with three mirror lenses; keep the laser on standby when not in use.
Excessive burns – Only use laser powers which produce retinal blanching; take care when lasering during scleral indentation not to get an excessive burn.
6.3.2 Retinal Detachment
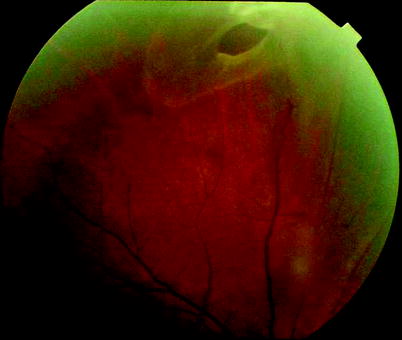
Fig. 6.39
This tear has SRF extending around its edge
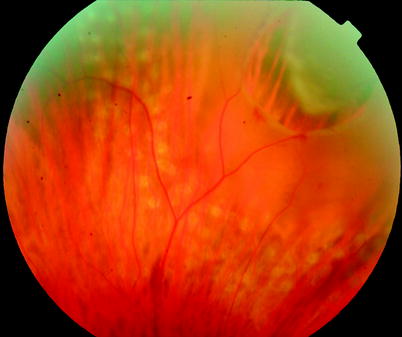
Fig. 6.40
The SRF around this tear is likely to lead to failure of the laser retinopexy
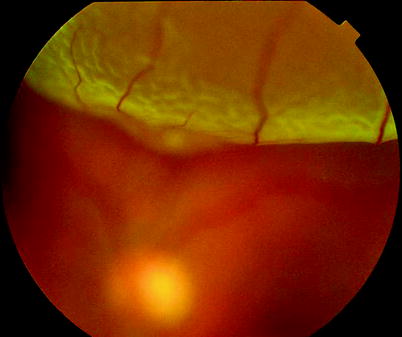
Fig. 6.41
The superior bulla of a RRD
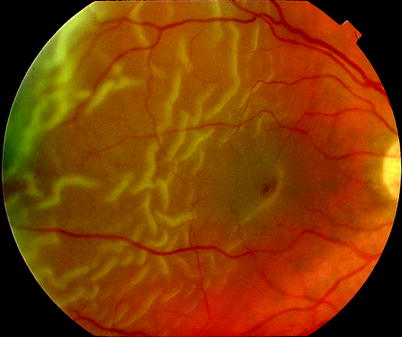
Fig. 6.42
Wrinkling of the retina in RRD
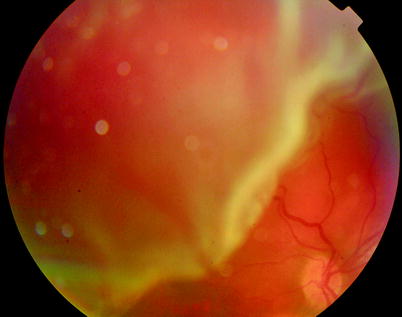
Fig. 6.43
A superior bullous RRD may overhang the macula blocking a view of the fovea. It is therefore difficult to judge whether the fovea is detached. Usually, the fovea is found to have this SRF peroperatively
The definition of rhegmatogenous retinal detachment is a retinal break with subretinal fluid. This may be as little as a small cuff of fluid or as much as total retinal detachment. Once the detachment has occurred, identification and closure of the retinal break or breaks is the primary aim of surgery.
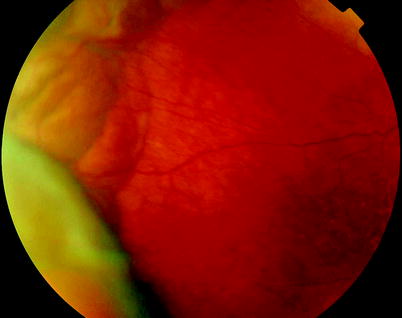
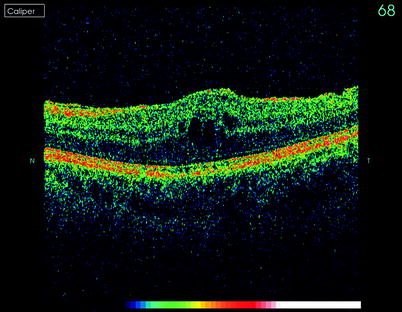
Fig. 6.44
Choroidal effusions should not be confused with retinal detachment; the appearance is of an immobile smooth elevation with a green or brown underlying colour due to the detachment of the RPE
Fig. 6.45
This patient had a persistent inferior retinal detachment postoperatively with CMO present. Some surgeons argue that peripheral RRD has secondary effects on the macular receptors
Attachment of a silastic explant to the sclera of the eye to create a dent in the sphere of the eye underneath the break or breaks allows the retina to reattach. This may occur because of relief of traction or because of an alteration in the fluid currents in the eye.
Alternatively, the vitreous can be removed by pars plana vitrectomy and a long-acting gas bubble, such as sulphahexafluoride or perfluoropropane, inserted into the vitreous cavity. The gas bubble contacts the rim of the break preventing the passage of fluid through the break (tamponade). Thereafter, subretinal fluid will be reabsorbed by the RPE and the retina will flatten.
The gas bubble is only temporary, and the indentation from an explant may gradually lessen; therefore, retinopexy is also applied to seal the tear and avoid re-accumulation of the subretinal fluid.
The shortening on the retina produced by proliferative vitreoretinopathy may prevent retinal reattachment unless the fibrous membranes are surgically removed or the retina cut to fit the inside of the eye (retinectomy). In this circumstance, silicone oil may be inserted into the vitreous cavity to provide long-term support to the retina allowing time for the proliferative vitreoretinopathy process to stop. Silicone oil in the vitreous cavity is associated with a number of complications including cataract, glaucoma, refractive changes and low-grade retinal toxicity.
This type of surgery requires a preoperative assessment of the patient, particularly determining whether the patient requires conventional surgery or vitrectomy.
Although it is possible to perform most of these operations by vitrectomy alone, this may be inconvenient for the patient in that they will often develop a cataract requiring further surgery later. They may also be required to position their heads for 1–2 weeks and will have delayed visual recovery for 2–8 weeks depending on the gas used. A conventional procedure, on the other hand, does not produce cataract and requires no posturing in most circumstances. However, it requires the development of additional surgical skills, and visualisation of retinal breaks can be more difficult via indirect ophthalmoscopy.
I treat most RRD with PVD by PPV, and those with attached vitreous are operated by non-drain; however, there is wide variation in methods worldwide, and, therefore, non-drain, DACE, pneumatic retinopexy and PPV are all described in this text.
Principles
The principles of surgery are break closure, relief of traction, alteration of fluid currents and retinopexy (Custodis 1952). Under normal circumstances, the retina is held in place by physiological forces such as hydrostatic and osmotic pressure, weak intracellular bonds and the intracellular matrix. If a break appears in the retina, these forces are not sufficient to prevent the accumulation of subretinal fluid, which usually comes from fluid vitreous behind the posterior hyaloid.
Break Closure
Any treatment of a retinal detachment depends primarily on identification of all the breaks in the patient. A small ‘pinprick’ break will quite easily result in a redetachment if it is missed and remains untreated. Therefore, careful inspection of the retina is of paramount importance. Once identified, the breaks can be closed in a number of ways. In conventional surgery, this is performed by placing an indent underneath the break or breaks (Goldbaum et al. 1975). In vitrectomy surgery, the break is apposed to the RPE by the action of a gas bubble (or silicone oil) on the retina.
Relief of Traction
The placement of a plombage may also have the effect of relieving traction by shortening the distance to the centre of the eye if vitreous traction is present. However, it is likely that vitreous traction is already relieved by production of the retinal detachment. The traction of the vitreous on the retina is negated by the removal of the vitreous in vitrectomy. Traction becomes important when this is adjacent to a retinal break, for example, in PVR, (proliferative vitreoretinopathy) when the break is prevented from closing onto an indent or onto the back of the eye with gas. Traction by scar tissue is removed during membranectomy in PVR surgery.
Alteration of Fluid Currents
Fig. 6.46
Application of an indent under a tear alters the fluid currents (arrows); by increasing the velocity of fluid flow, the pressure is dropped drawing the retina to the sclera (Bernoulli’s principle)
Fig. 6.47
If fluid passes over a membrane with a hole in it, the fluid enters through the hole (a). If an indentation is inserted under the hole (b), the space the fluid must go through narrows (double arrow); for the same flow, the velocity of the fluid increases. According to Bernoulli’s principle, this drops the pressure at this point, causing the membrane to move towards the indent eventually closing the hole on the indent (c) and preventing any other fluid entering
Fluid currents are present in the retina in the presence of PVD, which help lift the retina through their action on a retinal break. The effect of currents can be seen in the non-drain retinal detachment repair where appropriate placement of a plombage will allow resolution of SRF and closure of the break onto the indent, even if at the end of the operation, the break is not flat onto the indent itself. Although it is not necessary to close the break onto the indent at the end of surgery, it is important that the indent is in the correct position to modified fluid currents to produce break closure over the next 24–36 h. The indent produces an increase in the velocity of the fluid over the indent because the cross-sectional area through which the flow of fluid can pass through the break has been reduced. This in turn induces a pressure drop by Bernoulli’s principle (velocity of a fluid increases causing a decrease in pressure in the fluid) causing the retina to move onto the indent. For this reason, it is not necessary to perform drainage of SRF in all patients.
Bernoulli’s principle states that as the speed of a moving fluid increases, the pressure within the fluid decreases.
Retinopexy
Retinopexy is important because the means of closing the break is often temporary, such as with absorption of a gas bubble or when a plombage gradually loosens with ageing or becomes adrift from loosening of the sutures. Once retinopexy has taken effect, it is entirely appropriate to remove a plombage at 10 days. This has been exploited by Lincoff and his balloon indent procedure (Oge et al. 2001) whereby a balloon is inserted into the orbit to produce an indent of the eye and is later deflated and removed. Similarly, internal tamponade is only necessary until the retinopexy has sealed the break.
Table 6.1
Proportion of methods used for RRD in my team
Operations for RRD (n = 1,528) | % |
|---|---|
Pneumatic retinopexy | 0.7 |
Non-drain | 22.8 |
DACE | 1.6 |
PPV | 74.9 |
The percentages of operations performed in my team for RRD between 1998 and 2006.
Surgical Pearl of Wisdom
‘Although rare, it occasionally happens that an expansive concentration of gas is incorrectly injected at the end of surgery (e.g. 30 % C3F8 instead of 30 % SF6). Postoperatively, the patient is in acute pain, with a shallow AC, no meniscus below the gas, and a very high IOP. The management is to remove some gas, but how much to remove? How to do it in such a way that the pressure does not crash catastrophically?
Putting a needle through the pars plan could result in a sudden egress of gas, hypotony and choroidal haemorrhage.
The following method allows a controlled and predictable removal of exactly the right amount of gas.
First, measure the IOP, which we will assume for the sake of this example is 80 mmHg. Then, convert this value into a height of water. Atmospheric pressure is about 760 mmHg, which corresponds to 10,330 mm of water, a conversion factor of 14. Hence, 80 mmHg is equivalent to 1,087 mm of water.
Take a 27-gauge needle and put it on the end of a giving set, run through with Hartmann’s solution. Sit or lie the patient down, and adjust the height of the top of the fluid to roughly 1,087 mm above the eye.
Pass the needle through the pars plana and turn on the drip. Nothing happens! That is because the pressure of the fluid is exactly the same as the IOP.
Now get an assistant to lower the height of the bag slowly (say over the course of 1 min) to a height corresponding to the target pressure (210 mm water is equivalent to 15 mmHg).
As the bag is lowered, you will see the gas coming slowly out through the needle and up the giving set. Once the pressure is normalised, the needle can be removed.
By using this method you can achieve exactly the target pressure you desire, but in a controlled way with no sudden changes in IOP’.
(Bill Aylward, Moorfields Eye Hospital, London, UK)
6.3.3 Pars Plana Vitrectomy
Table 6.2
Difficulty rating of PPV for RRD
Difficulty rating | Moderate |
|---|---|
Success rates | High |
Complication rates | Medium |
When to use in training | Early |
Additional surgical steps:
1.
Search for breaks with deep scleral indentation.
2.
Apply cryotherapy.
3.
Drain subretinal fluid (SRF).
4.
Drain SRF and insert air.
5.
Drain residual vitreous cavity fluid off disc.
6.
Apply cryotherapy or laser retinopexy as required.
7.
Exchange long-acting gas.
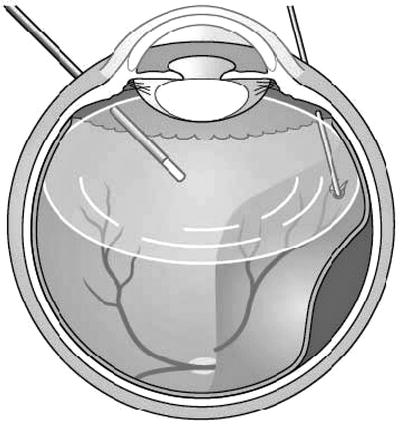
Fig. 6.48
The eye is orientated with the lens superiorly for PPV
Introduction
PPV is becoming more popular for RRD repair because of the ease of application and good visualisation of the retina with wide-angle viewing systems. Examination of Medicare data for fees in the USA shows a 72 % increase in the use of PPV for RRD and a 69 % reduction in the use of scleral buckles from 1997 to 2007 (Ramulu et al. 2010). In addition, cataract can easily be dealt with peroperatively or postoperatively by phacoemulsification and posterior chamber lens implant. Perform the PPV in the usual way. Take care if operating on a bullous RRD not to encourage incarceration of the retina into the sclerotomies or into the infusion cannula. So far, randomised studies support the use of PPV or scleral buckle in RRD surgery (Heimann et al. 2007).
To avoid this:
Try to drain some SRF internally early in the procedure from a break (this also aids removal of the gel without risk of biting the retina).
Remove as much vitreous as possible (vitreous incarcerates first then the retina) from around the infusion cannula and sclerotomies.
Use scleral plugs.
Use self-sealing sclerotomies or small-gauge surgery with stents with valves in situ.
Insert heavy liquid to splint the retina posteriorly.
Fig. 6.49
During vitrectomy, indentation is required to bring peripheral retina into view and to aid internal search for retinal breaks
Perform an internal search by indenting with a squint hook to locate all of the retinal breaks.
Finding the Breaks
Approximately 55 % of RRD have more than one break. Success of surgery requires finding and treating all the breaks. These manoeuvres can help:
Indentation dynamic movement of the retina.
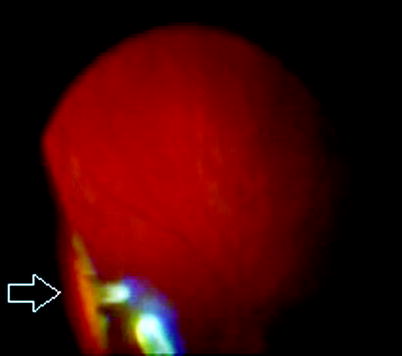
Fig. 6.50
The flap of a U-shaped tear can be seen on indentation during PPV (arrow)
Look out for small elevations of retina at the posterior border of the vitreous base (the posterior border can be seen as a faint white line on the retina), use the light pipe to engage the vitreous behind the elevation and lift the vitreous to see if you can open the break hidden behind it.
Use heavy liquid to force SRF out of the break (especially if small), thus making the break pout.
Watch for Schleren, the oily track of SRF exiting the retinal break.
Apply cryotherapy which makes the break ‘shine’ up inside the frozen retina.
Detect the release of circulating RPE cells into the vitreous cavity through the hole, which looks like a tiny volcano. This is especially helpful if cryotherapy has been applied and confirmation of the presence of a break is required.
Apply laser retinopexy which will blanch the attached retina around the break but not the bare RPE in the centre of the break.
Gently aspirate over the suspected break with the flute needle to see if SRF will drain through the suspected break; take care that you do not create a hole by doing this thereby fooling yourself that you have found the break.
If you have tried everything else use a 40-gauge needle to inject some Trypan blue dye into the subretinal space, heavy liquids can be inserted to move the dye towards the periphery, and egress of the dye through the break will allow location of the break (dye extrusion, DE-TECH, method) (Jackson et al. 2007; Wong et al. 2009).
Surgical Pearl of Wisdom
When performing an internal search for tears, it is important to use the right technique and apply some basic anatomy. Tears occur on the back edge of the vitreous base. This is usually 2 mm behind the ora, but this can be variable. One can often identify the vitreous base in attached retina by a white (or more realistically mild grey) with pressure reaction. This arises because the collagen strands in the vitreous base insert perpendicularly into the ora. In detached retina, there is often a transition line or fold visible at the back edge of the vitreous base. The combination of vitreous traction and a tear mean that the flap will often stand up when rolled. I use an empty plug forceps for this and roll in a posteroanterior then anteroposterior direction from ora posteriorly and then anteriorly. The aim is to create an indent with the surgeon’s line of sight tangential to the retina. As the indent moves posteriorly, the break rolls up and then down onto and off the indent and will frequently stand up in the process. Other people use a squint hook just as effectively. The important point is that it involves dynamic rolling as well as indentation. Granules of pigment in the peripheral vitreous close to back edge of the vitreous base should also be treated with great suspicion; they often mark the position of a tear.
D. Alistair, H. Laidlaw, Dept of Ophthalmology, St Thomas Hospital, London, UK
Apply cryotherapy or endolaser to any flat breaks and any which are indentable. Any breaks which are not can be treated with retinopexy after insertion of the air by cryotherapy or laser. Laser must be applied to flat retina and therefore is applied after air insertion or with heavy liquid in situ. Laser should be used if there are very large breaks or multiple breaks to help prevent overuse of cryotherapy which increases the risk of PVR. Many surgeons like to mark the edge of retinal breaks with a small burn from endodiathermy. This allows visualisation of the burn and therefore the location of the tear after the air insertion (unmarked breaks are difficult to see after air injection) to allow easy retinopexy. Alternatively, remember where the break is using anatomical landmarks such as blood vessels to direct you to the break.
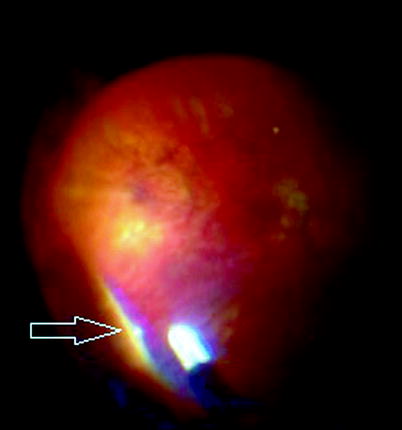
Fig. 6.51
If you see a tiny tag like this, there may be small U tear in its posterior edge (arrow). Lift up the vitreous frill to expose the break
Advantages and Disadvantages of Retinopexy Under Air
Advantages of retinopexy under air:
Breaks are flat allowing laser application.
Cryotherapy application is much quicker under air because of the insulating properties of the air.
Peripheral laser can be easier to apply because the air allows a wider field of view (but with reduced magnification) with the IVS in a phakic patient.
Disadvantages:
Breaks are more difficult to visualise.
Cryotherapy releases RPE cells which will not be removed (air fluid exchange has already been completed).
Condensation on the IOL in the presence of a capsulotomy reduces the view.
Posterior lenticular opacification in a phakic patient reduces the view.
Glare from the tip of the endo-illumination is increased. If you are using a bullet light pipe, cut off the exposed end to make it flush with the sleeve to reduce glare.
Fig. 6.52
Subretinal fluid can be drained by placing a ‘flute’ instrument just anterior to the posterior edge of the retinal break, thereby avoiding vitreous attached to the anterior edge of the break
Fig. 6.53
Injecting air during a vitrectomy whilst draining SRF through a retinal break. By flattening the retina extensively before insertion of air, complete SRF drainage is facilitated. Keep the flute needle over the break till a maximal air fill and SRF drainage have been achieved before draining any fluid from the back of the eye
Draining Subretinal Fluid
Drain the SRF internally with a flute needle placed over one of the breaks. It helps to drain as much SRF as possible by fluid/fluid exchange before going to air/fluid. With the retina as flat as possible, commence inserting air through the infusion (using the air pump of the vitrectomy machine). There will be a moment when the vitreous cavity is half filled when the view of the needle tip and the break is lost. Keep the needle over the break and advance very slightly into the eye to compensate for the flattening of the retina. Do not stop draining. The moment of poor visualisation will pass and the view will return, and the SRF drainage can be completed. When bubbling is heard from the flute needle, only air is being removed, and the needle tip should be advanced gently towards the break to drain more SRF.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


