Fig. 7.1
The ophthalmoscopic appearance of retinocytoma. Note translucent grayish retinal mass, calcification, retinal pigment epithelial alteration and chorioretinal atrophy (a). Chorioretinal atrophy may not be present in the early stages (b).
Box 7.1 Salient Features of Retinocytoma
Retinocytoma is a benign manifestation of RB1 gene mutation. |
The ophthalmoscopic appearance resembles the spectrum of retinoblastoma regression patterns observed after irradiation. |
Presence of a translucent grayish retinal mass, calcification, retinal pigment epithelial alteration, and chorioretinal atrophy with or without associated staphyloma are four diagnostic features. |
Retinocytoma is not associated with retinal exudation or prominent feeder vessels but may be associated with tortuous sclerosed feeder vessels. |
Retinocytoma lacks growth over short periods of observation (weeks to months). |
Retinocytoma can undergo malignant transformation into retinoblastoma. |
The areas of chorioretinal atrophy closely resemble retinoblastoma regression after irradiation, suggesting tumor regression. Photographic regression of retinocytoma with increasing chorioretinal atrophy over prolonged follow-up has been observed [3, 17]. The mechanisms of tumor regression in retinocytoma are unknown but might involve apoptosis [18] rather than ischemia or immune-mediated necrosis [19]. Calcification is not limited to the retinal mass and may be observed as seeding in the vitreous [20]. Intratumoral cyst, a feature of presumed well-differentiated retinoblastoma, is sometimes observed in retinocytoma [21, 22].
7.3.3 Risk of Second Malignant Neoplasms
A review of the large published series of patients with retinocytoma suggests that second malignant neoplasms are rare in patients with retinocytoma [1, 4, 8, 23]. It is possible that mechanisms that play a protective role in inducing retinocytoma also protect the extraocular cells from the development of second malignant neoplasms [24, 25].
7.4 Relationship with Retinoblastoma
Retinocytoma is considered to be a benign counterpart of retinoblastoma (Fig. 7.2) [2, 4, 7, 10]. The majority of retinocytomas are diagnosed when the parents of a child who has retinoblastoma are examined [1, 4, 8]. The examination of first-degree relatives, especially parents, when a new case of retinoblastoma is diagnosed is extremely important as it has major implications in genetic counseling [26]. The occurrences of retinoblastoma and retinocytoma are not mutually exclusive. In fact, retinoblastoma is now thought to be the final malignant result on a continuum of clonal progression from normal to benign to malignant cells after loss of RB1 [12–14].
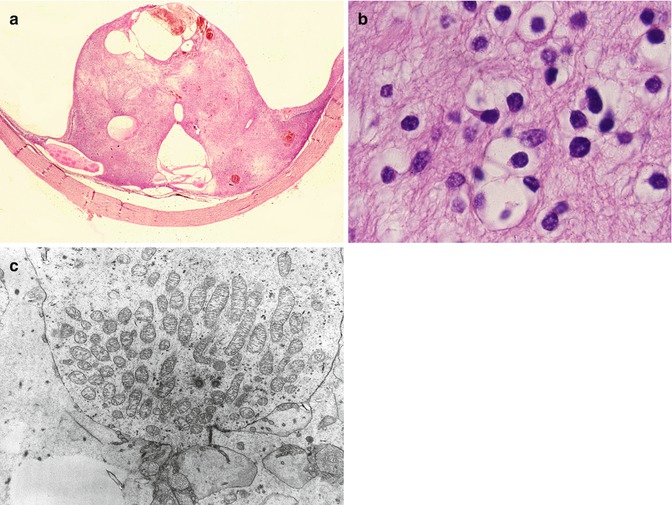
Fig. 7.2
Histopathology of retinocytoma. Macroscopic view showing pseudocystic appearance (a). On light microscopy the tumor is composed of benign cells (b). Note photoreceptor differentiation on electronmicrophotograph (c).
Histopathologic analysis of eyes enucleated for retinoblastoma reveals the presence of retinocytoma or retinoma adjacent to both normal retina and in up to 16 % of retinoblastoma tumors [12]. It comes as no surprise then that retinocytoma or retinoma and retinoblastoma can coexist as two separate tumors in the same eye [20] or between two eyes of the same patient [1, 4]. While many retinocytomas or retinomas remain benign for the lifetime of an individual, malignant transformation into retinoblastoma is well known [9, 27] and perhaps such occurrences account for cases of retinoblastoma in adults [28, 29].
Another scenario when diagnosis of retinocytoma can be retrospectively considered is when there is minimal initial response to chemotherapy in tumors presumed to be retinoblastoma. Moreover, the residual tumors fail to grow when all treatment has been discontinued. It is postulated that lack of response to chemotherapy is indicative of extreme differentiation (retinocytoma) rather than chemoresistance by an aggressive tumor [30].
7.5 Diagnostic Evaluation
In the majority of cases, the diagnosis of retinocytoma can be made with indirect ophthalmoscopy. However, fluorescein angiography, ultrasonography, and optical coherence tomography (OCT) can be useful ancillary studies.
7.5.1 Fluorescein Angiography
Fluorescein angiography of retinocytoma shows prominent superficial network of fine vessels in the arterial phase without significant leakage in the venous or late phase [9].
7.5.2 Ultrasonography
Ultrasonography is useful to demonstrate calcified lesions that show characteristic features including acoustic solidity and shadowing due to calcification within the mass on B-scan ultrasonography. A-scan ultrasonography shows a sharp anterior border, high internal reflectivity, and attenuation of orbital echoes posterior to the tumor.
7.5.3 Optical Coherence Tomography
OCT of retinal astrocytic hamartoma reveals full-thickness replacement of the retinal anatomic layers with the tumor and shadowing corresponding to the intralesional calcification. It can be useful in ascertaining areas of chorioretinal atrophy.
7.6 Differential Diagnosis
Despite characteristic ophthalmoscopic features of retinocytoma outlined above, certain entities can closely resemble retinocytoma. Retinoblastoma, astrocytic hamartoma, and myelinated nerve fibers can be difficult to differentiate ophthalmoscopically from retinocytoma (Table 7.1).
Table 7.1
Differential diagnosis of retinocytoma
Feature | Retinoblastoma | Retinocytoma | Astrocytic hamartoma | Myelinated nerve fibers |
|---|---|---|---|---|
Calcification | White, chunky | White, chunky | Yellow, spherical | Absent |
Chorioretinal atrophy | Absent | Present in older patients but absent in early retinocytoma | Absent | Absent |
RPE changes | Present | Present | Absent | Absent |
Feeder vessels | Present | Absent (except sclerosed and tortuous) | Absent | Vessels obscured |
Exudation | Absent | Absent | May be present | Absent |
Growth a | Present | Absent | Absent | Absent < div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|