Leukocoria or cat’s eye reflex
45 %
Strabismus
25 %
Inflammatory symptoms (preseptal cellulitis)
10 %
Poor vision
10 %
Screening due to family history
5 %
Incidental detection
5 %
For several reasons discussed elsewhere in developing nations, retinoblastoma tends to be more advanced at presentation with extraocular disease (Chap. 5). One of the major limitations to prompt treatment of retinoblastoma worldwide is access to health care. As retinoblastoma care providers, it is important for us to increase accessibility for our patients into a system that is equipped to treat this condition adequately. Community education and awareness and training of ancillary staff that are able to triage and arrange prioritized evaluations are some of the important components of this approach (Chap. 5).
1.3 Misdiagnosis
Histopathological studies of enucleated eyes report misdiagnosis rates from 11 to 40 %, and clinical studies of referral patterns report misdiagnosis rates from 16 to 53 % [3]. This may be attributed to many factors including rare incidence of retinoblastoma, multiple conditions that simulate retinoblastoma, the unfamiliarity of the primary health care providers, the age of presentation, and the difficulty in examining children (Chap. 2). Consequently, a thorough and detailed assessment should be done on patients suspected of having retinoblastoma.
1.4 Stepwise Evaluation for Retinoblastoma
A practical stepwise approach specifically to evaluate a child suspected to have retinoblastoma includes detailed history taking, initial office examination, and focused ophthalmic ultrasonography, followed by examination under anesthesia and neuroimaging if necessary (Fig. 1.1). This approach is merely a guide that can be modified as needed based upon clinical setting.
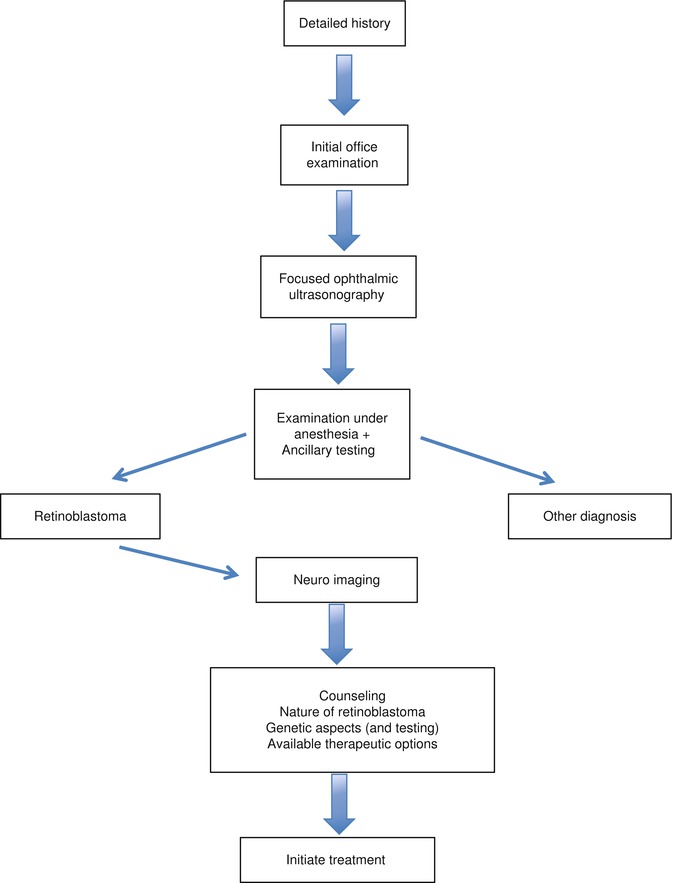
Fig. 1.1
Stepwise evaluation for retinoblastoma. This approach is merely a guide that can be modified as needed based upon clinical setting
1.4.1 History
For a child suspected of having retinoblastoma, it is important to examine the patient and family promptly upon referral, and the initial consultation may be performed in an office setting (Table 1.2, Box 1.1). The story of how and over what time course the condition was noted, the health care professionals that saw the patient, and what was done to the child before they arrived must be recorded. A birth history including the pre- and perinatal history is important. Typically the gestational age at birth, type of delivery, birth weight, and any delivery or pregnancy complications, including infections or medications taken during the pregnancy, are noted. It is also important to inquire if any abnormalities were noted on the eye screening exam after birth or if there were any unusual birthmarks or malformations. The current history should include the child’s health, any medical conditions, and environment including pets, recent trauma, or illness. For retinoblastoma suspects, the family history should include number of siblings, their health and ocular history, and any family medical disorders. It should be noted if there was any poor vision, blindness, or loss of an eye in the family. Both parents should be questioned about their ocular health and examined if no recent dilated exam has been preformed. A small subset of parents of children with RB will have evidence of retinoma/retinocytoma and even unknown treated retinoblastoma (Chap. 7) [4].
Table 1.2
Elements of medical history in a child suspected of having retinoblastoma
Time since onset | Duration |
|---|---|
Prior evaluation | Prior diagnosis |
Prior treatment | |
Prior surgical procedure | |
Prior biopsy | |
Perinatal history | Pregnancy complications |
Prematurity | |
Birth weight | |
Type of delivery | |
Use of oxygen | |
Personal history | Malformations |
Exposure to pets | |
Recent trauma | |
Systemic illness | |
Family history | Genetic disease |
Blindness | |
Enucleation | |
Amblyopia | |
Retinoblastoma |
Box 1.1 Elements of fundus examination in a child with retinoblastoma
Tumor size | ||
Tumor location | ||
Associated features | Subretinal fluid | Localized, diffuse |
Subretinal seeds | Localized, diffuse | |
Vitreous seeds | Localized, diffuse | |
1.4.2 Initial Examination
The initial examination of the child can be started in the office while taking the history, by observing the comfort and behavior of the child, and noting any size, proportion, or facial abnormalities (Table 1.3). It may be possible to observe leukocoria, strabismus, or periorbital swelling and visual behavior before initiating the formal examination. Assessing the vision is dependent on the age of the patient and the amount of cooperation; however, the condition of each eye should be assessed and recorded along with the pupillary response and the presence or absence of heterochromia of the irises. A brief observation of the periorbital tissues, cornea, conjunctiva, and sclera should be performed before administrating dilation drops. Using a direct ophthalmoscope, the pupillary light reflex can be noted in both eyes.
Table 1.3
Elements of initial examination (office) in a child suspected of having retinoblastoma
External examination | Facial abnormalities (13q deletion syndrome) | |
Strabismus | ||
Periorbital swelling | ||
Presence of heterochromia | ||
Visual acuity | ||
Pupillary response | ||
Pupillary light reflex | Normal | |
Abnormal | Leukocoria absent | |
Leukocoria present | ||
Anterior segment examination | May be limited | |
Indirect ophthalmoscopy | May be limited | |
Ultrasonography | Mass | |
Calcification | ||
Retinal detachment | ||
Other abnormalities | ||
Upon completion of this portion of the examination, drops for pupillary dilation can then be administered (tropicamide 0.5 % and ophthalmic phenylephrine 2.5 %). It is worth emphasizing that both eyes should be examined in equal detail. The examination of the posterior pole is best done with an indirect ophthalmoscope. Depending on the age, the child may cooperate or parents may be needed to help secure the patient while lying supine on a table or chair (Fig. 1.2). Younger children can be swaddled with a blanket or sheet. The goal of the indirect examination at this point is to confirm the suspicion of retinoblastoma and determine whether further evaluation is necessary with an exam under anesthesia (EUA). It may be necessary to place an eyelid speculum in for proper visualization of the posterior pole; appropriate topical anesthesia such as ophthalmic proparacaine 0.5 % solution should be administered before placing the speculum. A detailed fundus examination with scleral depression may be performed with an anesthetic, eyelid speculum, and restraint; however, this is fairly traumatic for both the child and the family and is generally unnecessary if a planned exam under anesthesia is possible.

Fig. 1.2
An indirect ophthalmoscopic examination being performed in an office setting with the mother helping to hold the child
1.4.3 Ophthalmic Ultrasonography
A limited ophthalmic ultrasonography can be done in A/B scan mode using a 10 MHz transducer to visualize the presence of a mass, calcification, retinal detachment, or abnormalities of the posterior pole. Intraocular calcification can be highlighted during the ultrasound in B scan mode by turning down the gain of the unit.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


