Fig. 4.1
Three genetic forms of retinoblastoma. The vast majority of familial and sporadic heritable retinoblastomas are bilateral. However, 10–15 % are unilateral. Arrow indicates the index child or proband, with the indicated form of retinoblastoma. Males are indicated as squares and females as circles. A horizontal line connects the mother and father and a vertical line connects parents and offspring. The sex of the affected individuals is shown, although it is not relevant. Changing the sex of each affected individual would not change the accuracy of this figure
4.1.1 Familial Retinoblastoma
Ten percent of children with retinoblastoma inherit a RB1 gene mutation from a parent. In this circumstance, the condition is referred to as familial retinoblastoma. Every cell in the body of these children contains a RB1 gene mutation, the “first hit.” [6] The mutation to the other copy of the RB1 gene, the “second hit,” occurs in a retinal cell sometime after conception. The inherited gene mutation is highly penetrant and nearly all, about 95 %, of such children develop retinoblastoma.
4.1.2 Sporadic Heritable Retinoblastoma
Another 30 % of children with retinoblastoma also harbor a RB1 mutation in all of their cells and are at the same risk for developing retinoblastoma as children who inherit a mutation. However, these children do not have a parent with the mutation. Rather, their RB1 mutation occurred as a new germ line mutation. Although these children did not inherit the gene from an affected parent, they will be able to pass the mutation onto their children. This is called sporadic heritable retinoblastoma.
4.1.3 Nonheritable Retinoblastoma
The remaining 60 % of retinoblastoma patients have nonheritable disease. Their retinoblastoma develops as the result of two somatic RB1 mutations that occur in a single cell sometime after conception.
4.2 Incidence Rates
4.2.1 Unilateral and Bilateral Retinoblastoma
The vast majority of children with familial or sporadic heritable retinoblastoma develop bilateral disease but 10–15 % have unilateral disease [7]. All nonheritable retinoblastomas are unilateral. Incidence rates would be most informative if they were available for the three subtypes of retinoblastoma. However, incidence rates are generally available only for retinoblastoma overall with rates by laterality available only for selected countries. As explained above, bilateral retinoblastoma includes most instances of familial and sporadic heritable disease, while the vast majority of unilateral disease is nonheritable retinoblastoma. Therefore, bilateral rates can be interpreted as reflecting the incidence of heritable retinoblastoma familial and sporadic heritable combined and unilateral rates as reflecting nonheritable disease. In the only report of international variation in incidence by laterality, the incidence of unilateral disease was observed to vary markedly, much more so than bilateral disease [8].
4.2.2 Expression of Incidence Rates
Because 95 % of cases are diagnosed under the age of 5 years, incidence rates are better expressed as “per million children 0–4 years of age” than as “per million children 0–14 years of age,” as is common for other childhood cancers. In the graphs and discussion that follow, we present rates for children ages 0–4 years of age whenever the data are available.
4.3 Geographic Variation in Incidence
Variation in incidence among countries, regions, and ethnic groups or over time can provide clues to etiology. Environmental (defined here as nongenetic) factors are implicated in cancers that show great variation in incidence.
The rates of retinoblastoma vary about 50-fold across the continents [9], a degree of variability higher than that for several adult cancers, namely, stomach, colon, cervical and pancreatic cancer, and lower than that for lung and esophageal cancer, among others. Incidence in North America and in much of Europe is relatively uniform, somewhat higher in Central and South America, and varies more widely in Asia and Africa [9]. Overall, the rates are higher in less industrialized countries than in more industrialized countries. In addition, there are enormous variations within some countries. The data suggest variation by economic development, with higher rates in poorer regions of countries such as Brazil and Mexico [10]. Clearly the differences in the incidence rates of retinoblastoma between regions of higher and lower incidences may be due to other factors such as ethnic origin, genetic susceptibilities, and cultural and behavioral practices. A closer examination of the differences in incidence may identify specific risk factors for development of retinoblastoma.
4.3.1 North America
The incidence of retinoblastoma in the United States has not changed significantly from 1975 to 1995 [11]. The rates by race/ethnicity and region generally range from 10 to 14 per million children ages 0–4 per year (Fig. 4.2). Incidence rates were generally higher for African-Americans than for their white neighbors [9]. For African-Americans in Los Angeles, the incidence was lower and for native Hawaiians, incidence was higher, but these rates are based on small numbers of affected children and therefore are imprecise [9].
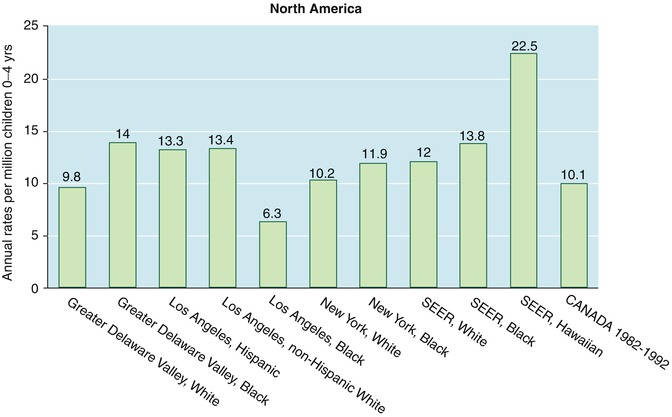
Fig. 4.2
Incidence of retinoblastoma in the North America in children ages 0–4 years (Data derived from Parkin et al. [9])
4.3.2 Europe
Within Europe, there is some variability in incidence (data not shown). Most countries have incidences in the range of 6–12 per million per year in children ages 0–4. However, there are a few notable exceptions. Bulgaria has a very low incidence (3.4 per million per year), while the province of Valencia in Spain (but not other regions in Spain) has the highest incidence for all of Europe, followed by Norway, Denmark, and Scotland (but not England and Wales) [9]. Although many of the registries have small numbers of cases, these differences within Europe are intriguing and do not appear to follow an easily discernible pattern.
4.3.3 Central and South America
Population-based registries do not exist for all countries in Central and South America, and for some countries, rates are only available within select cities (Fig. 4.3). However, even with these limitations, there appear to be two groups in Central and South America, those regions with incidence under 9.5 per million per year in children ages 0–4 and those with an incidence greater than 15 per million per year [9].

Fig. 4.3
Incidence of retinoblastoma in Central and South America in children ages 0–4 years (Data derived from Parkin et al. [9])
4.3.4 Asia
Incidence also varies greatly in Asia (Fig. 4.4) [9]. The highest rate is found in Madras, India, while rates in the rest of India are much lower. The lowest incidence in Asia is found among Malays in Singapore, while Chinese in Singapore have the third highest rates in the continent. Notably, Chinese living in China have the second lowest incidence in the region.
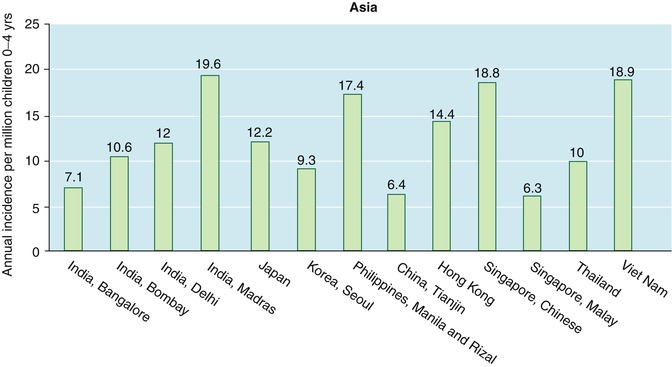
Fig. 4.4
Incidence of retinoblastoma in Asia in children ages 0–4 years (Data derived from Parkin et al. [9])
4.3.5 Africa
In Africa, where there are few population-based registries, incidence is also quite variable (Fig. 4.5) [9]. Incidence in sub-Saharan Africa is much higher than in Northern Africa. In the Middle East (including Israel) and North Africa, incidence is low and fairly uniform, ranging from 1.4 to 5.2 per million per year in children ages 0–4. However, even within the higher rates of sub-Saharan Africa, there is wide variability with the highest rates in West Africa and generally lower rates in the central and southern regions of the continent. It is noteworthy that the highest rate worldwide is in Bamako, Mali, one of the least economically developed urban centers in Africa.
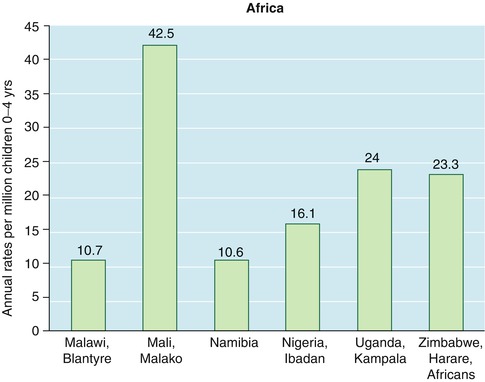
Fig. 4.5
Incidence of retinoblastoma in Africa in children ages 0–4 years (Data derived from Parkin et al. [9])
4.3.6 Oceania
The incidence in Australia is similar to United States and Canada (Fig. 4.6) [9]. The incidence in New Zealand, although higher than that in Australia, is similar in Maori and non Maori populations.
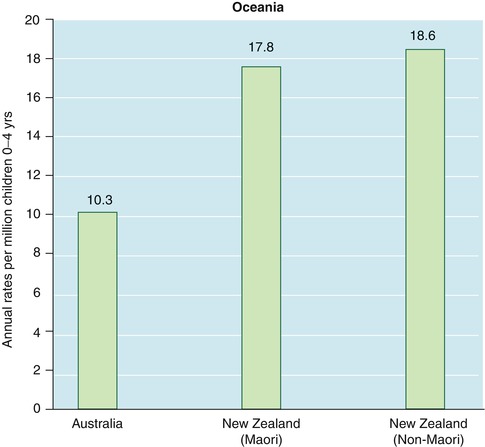
Fig. 4.6
Incidence of retinoblastoma in Oceania in children ages 0–4 years (Data derived from Parkin et al. [9])
4.4 Incidence by Sex
Males and females in most countries of the world have similar incidence rates (Figs. 4.7 and 4.8). Interestingly, in almost every Central and South American country, girls have an elevated incidence when compared to their male counterparts [9].
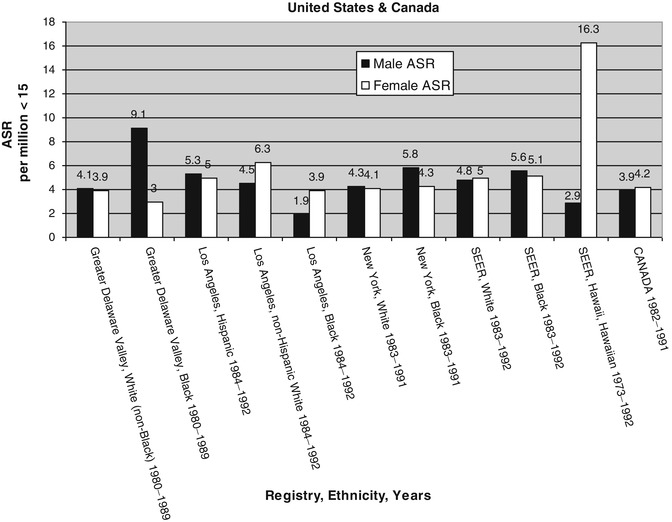
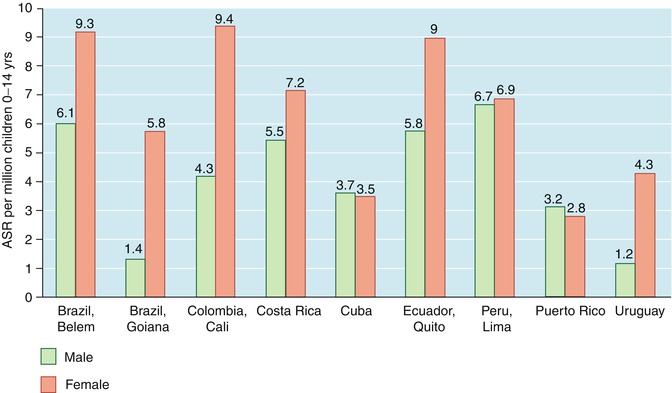
Fig. 4.7
Comparison of age standardized rates (ASR) for boys and girls ages 0–14 years in United States and Canada (Data derived from Parkin et al. [9])
Fig. 4.8
Comparison of age standardized rates (ASR) for retinoblastoma for boys and girls ages 0–14 years in Central and South America (Data derived from: Parkin et al. [9])
4.5 Environmental and Behavioral Risk Factors
To summarize the extent of variation, it is useful to consider the areas with the highest incidence worldwide [9]. The highest incidence of retinoblastoma is noted in Mali (Bamako), followed by (in descending order) Uganda (Kampala), Zimbabwe (African ancestry), Hawaii (native Hawaiians), India (Madras), Vietnam (Hanoi), the Chinese population of Singapore, New Zealand (essentially equal rates among non-Maoris and Maoris), Spain (Valencia), the Philippines, Colombia (Cali), Ecuador (Quito), Nigeria (Ibadan), Costa Rica, Peru (Lima), Norway, Brazil (Belem), and Denmark (Table 4.1). All of these populations have annual incidences above 15 cases per million children ages 0–4 years. Some global differences are particularly intriguing or paradoxical, given expected similarities in ethnicity and presumed shared environmental exposures: for example, Australia and New Zealand have very different rates which cannot be explained by ethnic differences (Fig. 4.6); one province in Spain has rates much higher than the rest of Europe, higher even than Spain’s former colonies (i.e., the Philippines, Latin America), many of whom also have high rates; some Scandinavian countries (but not Sweden) have rates equivalent to those of Northern Brazil (where a large proportion of the population is of African not European ancestry); and the Chinese in Singapore have a much higher rate than Malays in Singapore or Chinese in China or Hong Kong. There is no clear pattern, but there is a suggestion that environmental factors may play a role, though genetic susceptibility to particular environmental and behavioral risk factors may explain some of the differences.
Table 4.1
Regions with the high incidence of retinoblastoma
Country (Registry/Ethnicity) | Incidencea |
|---|---|
Mali (Bamako) | 42.5 |
Uganda (Kampala) | 24.0 |
Zimbabwe (African ancestry) | 23.3 |
Hawaii (native Hawaiians) | 22.5 |
India (Madras) | 19.6 |
Vietnam (Hanoi) | 18.9 |
Singapore (Chinese) | 18.8 |
New Zealand (non-Maoris) | 18.6 |
New Zealand (Maoris) | 17.8 |
Spain (Valencia) | 17.8 |
Philippines | 17.4 |
Colombia (Cali) | 17.1 |
Ecuador (Quito) | 16.6 |
Nigeria (Ibadan) | 16.1 |
Costa Rica | 15.7 |
Peru (Lima) | 15.5 |
Norway | 15.4 |
Brazil (Belem) | 15.4 |
Denmark | 15.3 |
4.6 Etiological Factors for Sporadic Heritable Retinoblastoma
Sporadic heritable retinoblastoma results from a new germ line mutation that is of paternal origin in over 90 % of patients [12, 13]. By virtue of being a new germ line mutation, the mutation occurs before the child’s conception. Based on these two facts, it seems logical that the search for genetic and nongenetic risk factors for sporadic heritable retinoblastoma should focus on the father’s genes and his exposures before the child’s conception [14]. However, associations with mother’s exposures have been observed as well. Although these associations may turn out not to be real, our understanding of retinoblastoma genetics and etiology is still evolving and we should not dismiss the possibility of effects of maternal exposure. It would be reasonable to hypothesize preconception exposure to mutagens, variants of metabolizing genes that prolong the duration or increase the level of a mutagen in the body and variants of DNA repair genes that result in less efficient repair of DNA damage as possible risk factors.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


