Chapter 133 Retinal Metastases
Introduction
Retinal metastases represent a small percentage of intraocular malignancy secondary to systemic cancers, even though 10% of patients who die of cancer have been found to have intraocular metastases.1–4 While relatively rare, the diagnosis of retinal metastases can be challenging, as its presentation can mimic other etiologies. High clinical suspicion and use of appropriate diagnostic techniques are vital in order to successfully diagnose and manage these challenging cases. This chapter provides a review of the literature of this rare clinical entity and management recommendations.
Metastatic cascade
Metastases are responsible for most cancer deaths.5 The understanding of metastases is limited due to the “hidden” nature of this process, as it occurs inside the body and is difficult to observe.5 Although many tumor cells are shed daily into the bloodstream or lymphatic system in those with cancer, the evidence is unclear on the fate of these tumor cells.6,7 Some models suggest that the majority do not survive in the circulation, while others suggest that most can survive and extravasate.5,6,8–10 For tumor metastasis to develop, a series of biological steps must be completed for a tumor cell to grow at a different site.5,6,10–15
Dissociation, invasion, and intravasation
For tumor cells to invade the circulation, they must dissociate from the primary tumor.5,6,10–14 On a molecular level, the dissociation is initiated by an array of motility factors11,12 and requires modulation of the expression of cadherins and integrins.5,6,13–16 Degradation of the extracellular matrix by proteolytic enzymes (primarily matrix metalloproteases and the plasminogen activator system) facilitates invasion of the surrounding connective tissue components.5,6,13,15,17–23 Metalloproteases also modulate cell adhesion in their local environment and help release growth factors from their stores.18,19,21 Then, tumor cells must penetrate the basement membranes of endothelial cells to enter the blood and lymphatic circulation.5,6,15 This step again requires well-coordinated proteolysis, as well as mechanical deformation and locomotion of the tumor cells.5,6,14,15 If this complex interaction is regulated successfully, certain populations of cells can break through the matrix and endothelium to reach the blood stream.
Hematogenous dissemination
The destination within the eye of circulating tumor cells may depend on several factors. Tumor size, vascular circulatory patterns and organ-specific factors which encourage tumor growth (so-called seed and soil factors) all may play a role in the location of metastases.5,6,15 Reese emphasized that, although tumor emboli are more prominent in the uvea, more than 90% of infectious emboli involve the retina.24 Because large emboli (e.g., tumor emboli) travel along the vessel wall in the slower-moving part of the blood stream, they are more likely to enter vessel branches, such as the short ciliary arteries. Small emboli (e.g., bacterial emboli) travel in the central, faster-moving part of the blood stream towards the terminal vessels, such as the central retinal artery.25 The marked vascularity of the posterior choroid relative to that of the retina (as noted above) could also contribute to more frequent choroidal involvement as metastatic tumors to the retina and optic disc, supplied by the central retinal artery, are rare.3,4
Extravasation and angiogenesis
Although circulation patterns and tumor size may play a role in implantation, metastatic growth may require organ-specific factors which facilitate tumor cell survival.5,15,16,26–28 Animal models of metastases support the role of both vascular flow patterns and organ compatibility factors in the development of metastases.5,29–31 Tumor cell anchorage at a target organ site depends on shear-resistant attachment to local endothelium. Various integrins and selectins have been identified which appear to mediate such specialized tumor cell adhesion under dynamic flow conditions.5,16,32,33
The delivery of the tumor cell to the site of metastasis depends on mechanical flow, but the growth or survival can depend on organ specific molecular interactions. These interactions can encourage tumor cell growth via expression of growth factors, and altering the gene expression of tumor cells.5,6,34–37 Expression of specific chemokine receptors by tumor cells may also target tumor cells to specific organs which express the specific ligands for these receptors.5,15,38–41 This match could lead to chemokine signal activation of genes which would encourage tumor cell growth.5,15 Specific interactions unique to retinal metastasis to this point have not been identified.
After the colony at the secondary site is established, angiogenesis will again play a key role in the continued growth of the tumor. The onset of angiogenesis involves an alteration in the balance between positive and negative regulators. In vivo experiments with human tumor cell lines have shown that both vascular endothelial growth factor (VEGF) and basic fibroblast growth factor (FGF) have direct roles in tumor-associated angiogenesis,42 and FGF-2 also are the two major angiogenic factors in the retina and increased expression of both has been identified in retinal tumors.43–47 VEGF not only regulates tumor-associated angiogenesis in response to local hypoxia and various cytokines, but may regulate breakdown of the blood–ocular barrier in ocular melanoma and other tumors.43,47–50 FGF-2 is a potent mitogen of choriocapillary endothelial cells, and FGF acts synergistically with VEGF to stimulate tumor angiogenesis.44,51–53
Review of case reports
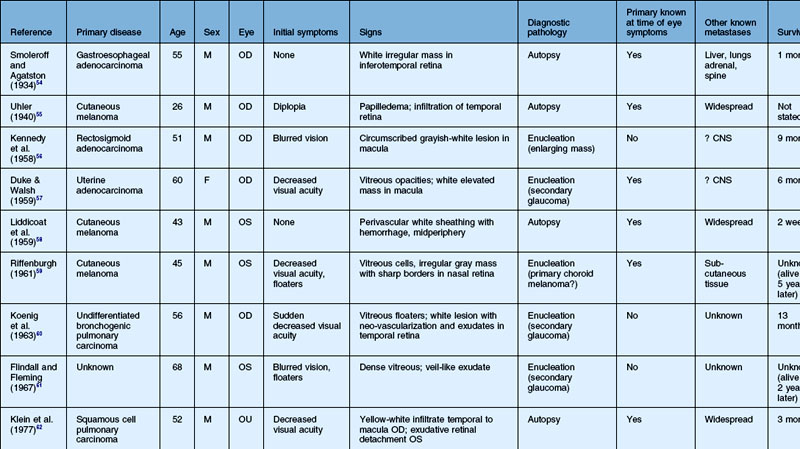
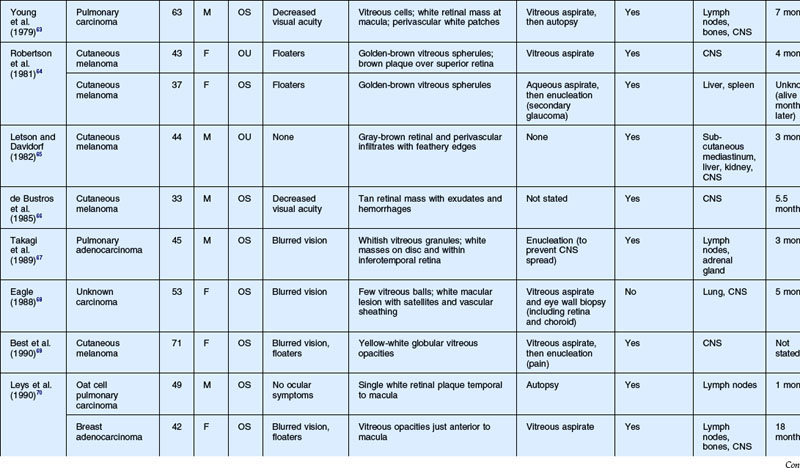
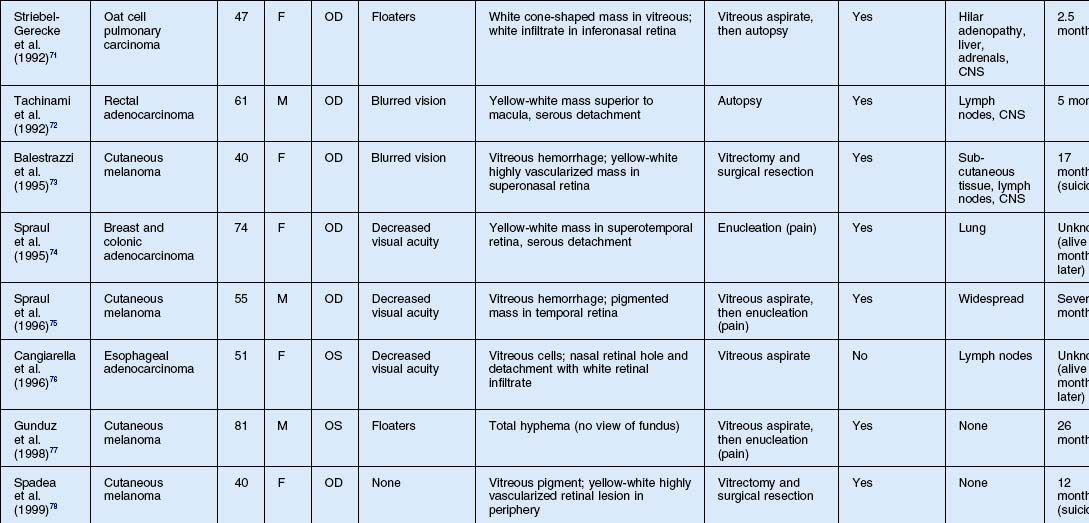
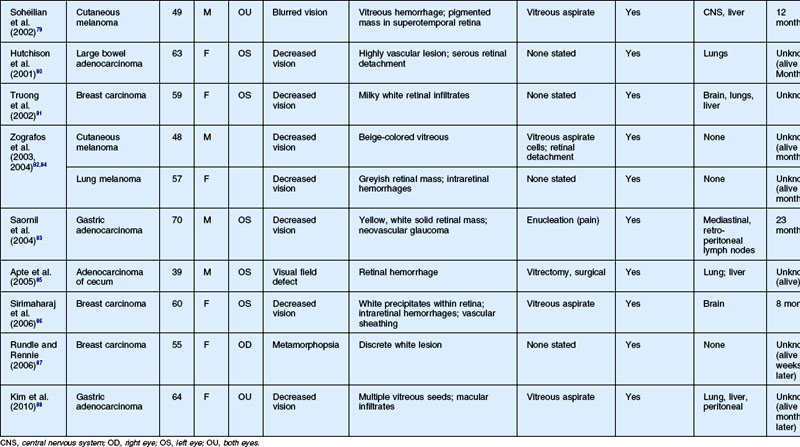
As noted above, retinal metastasis represents a small percentage of intraocular metastasis. Thus, no large single-center review has been published detailing outcomes associated with retinal metastasis. Publications in the literature have been limited to case reports.54–88 The first was published in 1934 and was diagnosed at autopsy.54 Until 1979, the diagnosis of retinal metastasis was made either by enucleation or at autopsy. Since 1979, diagnosis of retinal metastasis has been made via biopsy including vitreous, chorioretinal, retinal biopsies, clinical inspection or surgical removal.63 Although the case reports reviewed provide detail in presentation and treatment of retinal metastases, follow-up is limited for many of the publications. The clinical appearance, symptoms and outcomes from published case reports will be reviewed below and are displayed in Table 133.1.
Clinical findings
Symptoms
The most common visual complaint among those with retinal metastases is decreased or blurred vision (Table 133.1). Floaters are also a common complaint. Other symptoms include pain, diplopia, and red eye. Some cases presented without any specific visual symptoms.54,58,65 The underlying primary source of the metastases did not have a bearing on the type of visual symptom reported by the patient.
Signs
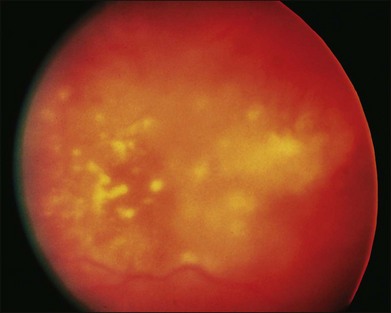
The clinical appearance of retinal metastases can vary based on the primary tumor and level of invasion of the tumor. Metastatic melanoma typically presents as a pigmented lesion within the retina with irregular borders and flat appearance (Fig. 133.1). Carcinomas tend to be non-pigmented, white or yellow in appearance and vary in size (Fig. 133.2). Some metastatic carcinomas can appear with significant mass and an elevated appearance with surrounding subretinal fluid.

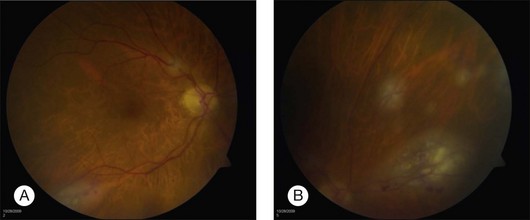
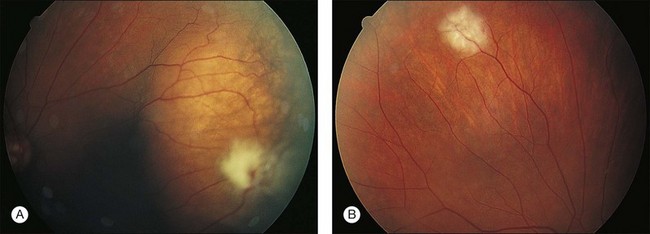
Intraretinal hemorrhage and exudates have been described in association with these lesions (Figs. 133.3, 133.4). Subretinal hemorrhage has also been described as a presenting feature of metastatic carcinoma.85 Perivascular infiltrates can also be seen in some cases (Fig. 133.2). Retinal hemorrhages and exudates are thought to occur secondary to damage to the retinal microvasculature. Additionally, subretinal fluid has been described in several cases of retinal metastases. The appearance of subretinal fluid or exudative retinal detachment warrants an evaluation for a choroidal lesion.
Vitreous cells are often seen in association with retinal metastases. These cells are usually pigmented in cases of metastatic melanoma and can be large. Vitreous cells in melanoma cases can be floating throughout the vitreous cavity (described as “brown spherules” or “globular vitreous opacities”).64,69 In contrast, vitreous cells associated with metastatic carcinoma tend to be white and confined to the area overlying retinal involvement.68,70
Other signs include secondary glaucoma from tumor invasion into the ciliary body, iris or anterior chamber angle.57
Differential diagnosis
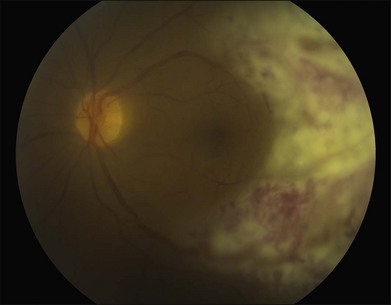
The differential diagnosis of a metastatic retinal lesion is varied, based on the initial appearance of the lesion. Choroidal metastasis with overlying retinal metastasis should be excluded initially (Fig. 133.5). For non-pigmented white retinal lesions seen in metastatic carcinoma, the differential includes inflammatory and infectious diseases such as toxoplasmosis chorioretinitis, cytomegalovirus (CMV) retinitis, herpetic-associated retinitis, syphilitic retinitis, endogenous endophthalmitis, sarcoidosis, multifocal choroiditis, birdshot choroidopathy, acute posterior multifocal placoid pigmentary epitheliopathy (APMPPE), intraocular lymphoma and other collagen vascular diseases. For pigmented lesions such as seen with metastatic melanoma the differential also includes choroidal tumors including melanoma and metastatic choroidal tumors, neovascular macular degeneration. Given the appearance of exudates and hemorrhages in some cases, retinal microvascular diseases such as hypertensive retinopathy, diabetic retinopathy, retinopathy secondary to anemia are also possible diseases. Finally, conditions that may simulate the vitreous floaters of retinal metastases include granulomatous uveitides, amyloidosis, asteroid hyalosis, or intraocular lymphoma.69,70
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


