17 Common symptoms include (1) visual field loss, often described as a “curtain” or “veil” coming down over a portion of the visual field; (2) abrupt loss of uniocular visual acuity, the hallmark of a detachment that involves the macula (Table 17–1); (3) floaters, objects in the visual field that originate in the vitreous; (4) photopsia, or light flashes; or (5) metamorphopsia, or image distortion. An approach to evaluating the symptoms of photopsias and floaters is outlined in Figure 17–1. All retinal detachments involve separation of the retina from the retinal pigment epithelium (RPE). On examination, it is important to define the shape of the retinal elevation as irregular, concave, or convex because these configurations both support the diagnosis of a retinal detachment and help point to its cause. Some findings associated with retinal detachments are outlined in Table 17–2.
Retinal Detachment
Evaluation of a Retinal Detachment
What are the Symptoms of a Retinal Detachment?
What Are the Signs of a Retinal Detachment?
Loss of visual field |
If from macular detachment, severe loss of visual acuity is described. |
If due to peripheral detachment, the loss in visual field is usually described as a “veil” or “curtain” over the affected portion of the visual field. |
Metamorphopsia |
Image distortion |
Floatersa |
Objects that move with eye movement in the visual field, usually associated with posterior vitreous detachment, blood, cellular, or inflammatory debris |
Photopsiaa |
An abnormal perception of light (typically lasting less than 1 second if due to retinal disease) |
a These are also symptoms of retinal breaks
Binocular indirect ophthalmoscopy is the best method to diagnose and characterize a retinal detachment. Scleral depression must be used to explore the peripheral retina for possible retinal breaks. In the absence of clear media, B-scan ultrasonography can indicate the presence of a retinal detachment, determine its shape, and identify shifting fluid in the case of an exudative detachment. A more detailed description of retinal detachment types can be found in Table 17–3. General shapes of retinal detachments are depicted in Figure 17–2, and photographs are shown in Figure 17–3.
How Do You Categorize a Retinal Detachment?
A retinal detachment can be categorized as rhegmatogenous, exudative, or tractional. A rhegmatogenous retinal detachment is associated with a retinal break (Fig. 17–2). The detached retina has an irregular surface associated with surface wrinkling caused by intraretinal edema (Fig. 17–2). Fluid can move through the break, causing the detachment to change size or shape as the eye moves. Pigmented particles can move through the break into the anterior vitreous. These particles are called tobacco dust, or the Schaeffer sign, and are seen with slit-lamp examination.
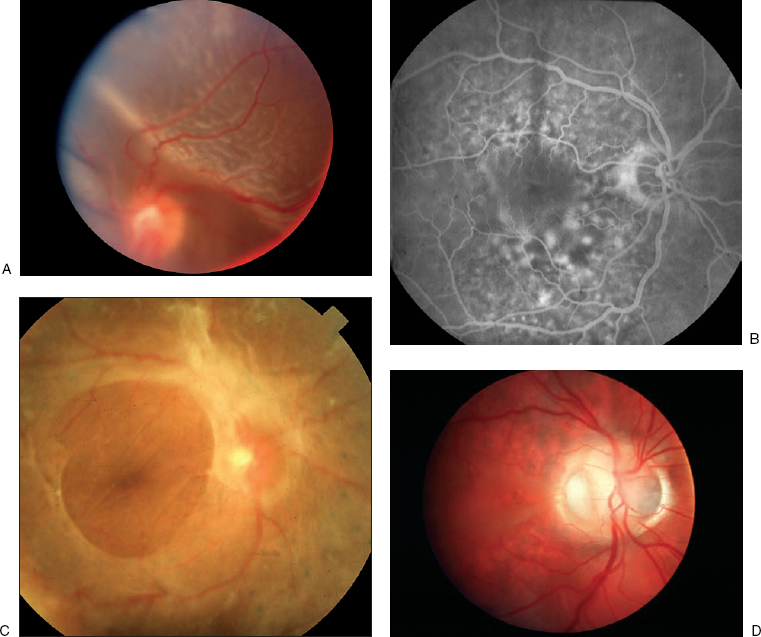
An exudative retinal detachment is the result of a damaged RPE pump or increased leakage from retinal or choroidal vessels, usually the result of inflammation (Figs. 17–2 and 17–3B). Typically, the detachment margins are less well defined than with other retinal detachments. These detachments are generally smooth on the surface and convex shaped. Most patients will exhibit “shifting” of subretinal fluid with changing head position as heavier subretinal fluid moves to a new gravity dependent position.
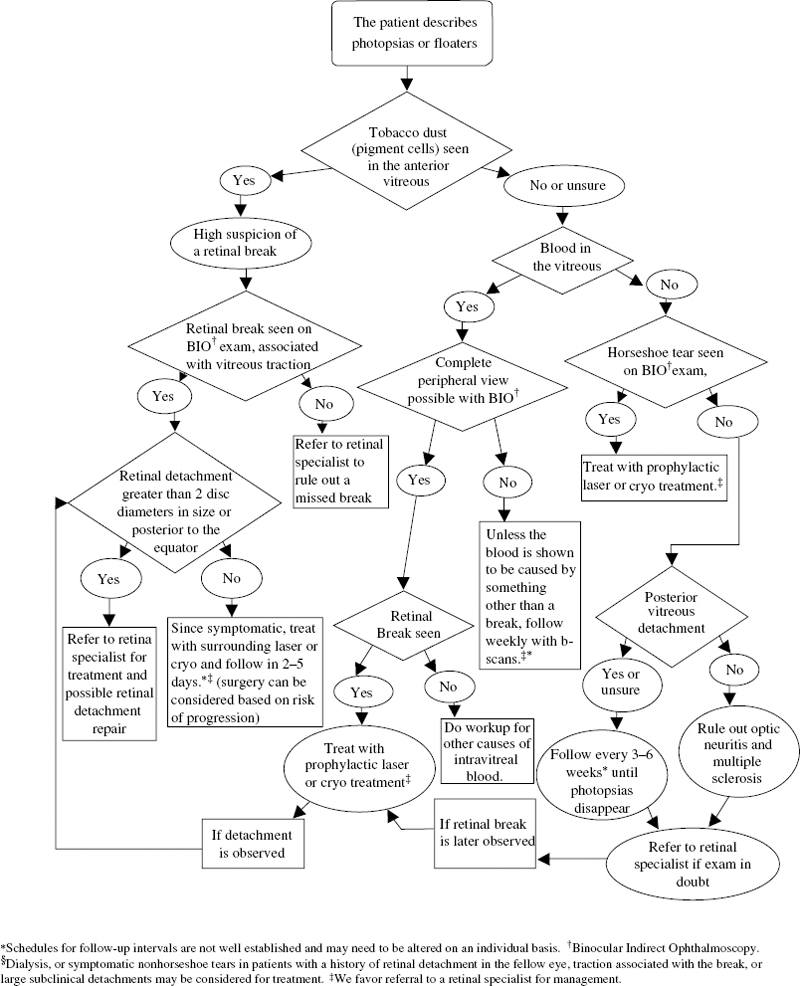
FIGURE 17–1. Management of the patient with flashes or floaters.
| Findings | Type of Detachment Typically Associated with the Findings |
|---|---|
Retinal elevation | Rhegmatogenous, traction, exudative |
Tobacco dust (anterior vitreous pigment cells) | Rhegmatogenous |
Vitreous hemorrhage | Rhegmatogenous, traction, exudative (less commonly) |
Inflammation | Rhegmatogenous, exudative |
Ocular hypopnea (acute) | Rhegmatogenous, exudative |
Ocular hypertension (chronic) | Rhegmatogenous |
Traction retinal detachments are typically the result of cicatricial (scarring) processes caused by systemic disease states, such as diabetes (Fig. 17–3C) or nonsystemic disease, states such as proliferative vitreoretinopathy (Fig. 17–2). A pure traction detachment does not shift with head movement, and its surface typically is altered to a flat or a concave appearance.
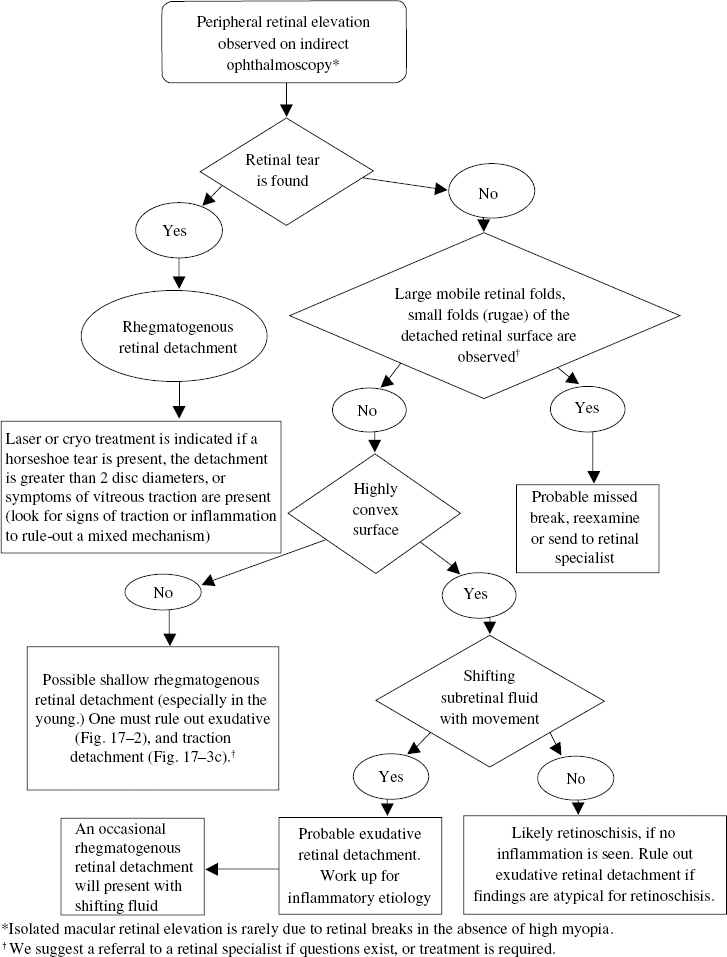
Detachments also may have mixed mechanisms that combine characteristics of more than one type, such as a traction detachment with a retinal tear or an exudative detachment with a tractional component. The characteristics associated with the individual types of retinal detachment as well as the predisposing conditions are outlined in Tables 17–3 and 17–4. A method for determining the type of retinal detachment and its basic management is outlined in Figure 17–4.
Rhegmatogenous retinal detachment |
These detachments are the result of a retinal break, usually a horseshoe tear (Fig. 17–5A) |
Typically, folds or “rugae” are observed on the surface (Fig. 17–2) |
The retinal surface moves with eye movement or scleral depression (it does not “shift”) |
Exudative retinal detachment |
Subretinal fluid clearance mechanisms are overwhelmed by excessive vascular exudation |
Inflammation is usually the cause |
No breaks are present |
A convex “dome” configuration to the retina is characteristic, often with shifting subretinal fluid (Fig. 17–2) |
Traction Retinal Detachments |
The underlying disease processes create fibrous or fibrovascular membranes that pull the retina away from the retinal pigment epithelium |
These detachments typically assume a flat, concave (Fig. 17–3C), or “funnel”-shaped retinal contour (Fig. 17–2) |
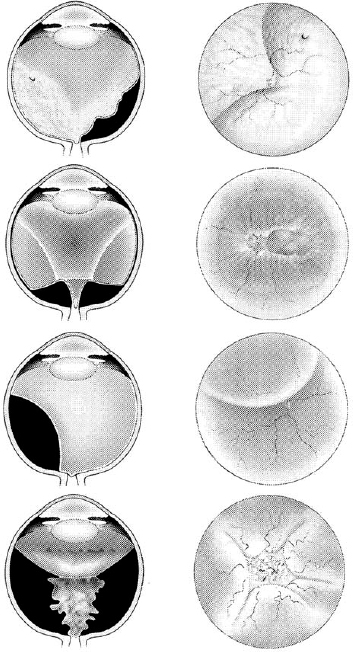
FIGURE 17–2. Various configurations of retinal detachments, with the side view on the left and front view on the right. (Top row) Rhegmatogenous retinal detachment with horseshoe tear and wrinkled retinal surface due to intraretinal edema. (Second row) Diabetic traction retinal detachment with elevation of the retina at the major vessels caused by vitreous traction. (Third row) Exudative retinal detachment with dome shaped contour that shifts with head movement. (Bottom row) Traction detachment associated with proliferative vitreoretinopthy, in a funnel configuration.
Rhegmatogenous Retinal Detachment
What Clinical Features Are Suggestive of Retinal Detachment with Retinal Breaks?
A rhegmatogenous retinal detachment is a retinal detachment with an associated break in the retina. It takes on a whitened appearance and develops a characteristic wrinkled pattern of folding. This wrinkling is the result of intraretinal edema, not membrane formation. For a break to lead to a retinal detachment, there usually must be accompanying changes in the vitreous gel, such as an increase in vitreous liquefaction, vitreous contraction, or sudden shifting of the vitreous from eye movement. Vitreous liquefaction, also referred to as syneresis, often occurs before development of a posterior vitreous detachment (PVD).
Myopia |
Lattice degeneration |
New cataract surgery or yttrium–aluminum–garnet (YAG) laser capsulotomy |
Trauma |
Positive family history |
Posterior vitreous detachment |
Previous retinal detachment in the fellow eye |
A Weiss ring is the portion of the cortical vitreous attached to the optic nerve that dislocates after a PVD. It is later seen as a floating ring in the central vitreous cavity. As the posterior vitreous starts to detach, traction at sites of abnormally strong vitreoretinal adhesion develop and are a common cause of development of a horseshoe tear. Tractional forces acting on the retina may create photopsias often described as “flashes.” Horseshoe tears are commonly associated with single or clumped pigment cells in the anterior vitreous called tobacco dust. This finding is seen only with careful examination of the anterior vitreous using a slit lamp. If a patient describes the new onset of flashes or floaters, it is prudent to note that tobacco dust was not observed if breaks are not found.
Choroidal melanomas often cause a “collar-button” formation observed on B-scan ultrasonography. This mushroom-shaped extension of the melanoma under the retina is caused by constriction at the point of its entrance through the Bruch membrane, resulting in a detached retina, which becomes elevated and draped over the surface of the melanoma. Choroidal detachments may be caused by many conditions but are most commonly caused by ocular surgery, such as glaucoma filtering surgery, cataract surgery, and scleral buckling procedures. They are typically smooth and solid appearing with a brown–red color. They do not move with eye movement and commonly are associated with exudative detachments. Choroidal detachments may be hemorrhagic or serous in origin and, unlike retinal detachments, they do not respect the anterior boundary of the ora serrata, often elevating the pars plana.
What Features Help to Differentiate between Types of Retinal Breaks?
The retinal tear most commonly associated with retinal detachment is the horseshoe tear (Figs. 17–2 and 17–5A). The tear is caused by vitreous traction on the anterior retinal surface producing a torn flap of elevated retina that is drawn into the vitreous cavity. Horseshoe tears often are seen in conjunction with lattice degeneration (Fig. 17–5B). Traction at the edge of lattice lesions is thought to predispose to break formation; however, tears can form anywhere in the fundus of patients with lattice degeneration. The operculated retinal tear (Fig. 17–5C) is a piece of retina that previously tore away from the retina as a result of abnormal vitreoretinal attachment and traction. The portion attached to the vitreous gel is left floating freely above the retinal surface, and the retinal defect takes the form of a round hole. Atrophic retinal holes pose little threat of causing a symptomatic retinal detachment, even if retinal elevation or PVD develops.1 These holes are the result of degenerative disease and usually are not associated with abnormal vitreous attachment.
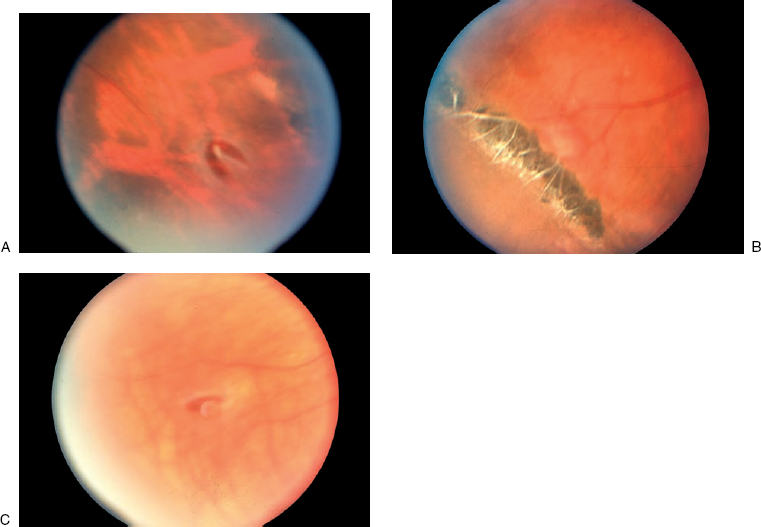
FIGURE 17–5. Types of retinal breaks. (A). Horseshoe tear. (B). Lattice degeneration and round atrophic holes. (C). An operculum in the center of the photograph overlying an associated retinal hole.
A retinal dialysis (Fig. 17–3A) is a peripheral break, usually at the ora serrata. The vitreous base spans the defect and is adherent to the anterior and posterior edge of the break. It may be many clock hours in size. It carries a better prognosis than the giant tear, which forms posterior to the vitreous base. Because a giant tear does not have vitreous base attachment to the posterior tear edge, the edge is prone to fold and gape. This makes the giant tear likely to cause retinal detachment.
Does Myopia Predispose to Retinal Detachment?
More than half of nontraumatic retinal detachments occur in myopic eyes. In one study, the risk of detachment for myopia ranging from —1 to —3 diopters was four times that of emmetropic controls.2 The risk was 10 times greater for eyes with myopia of more than 3 diopters. Myopia is also a significant risk factor for retinal detachment following cataract extraction. For this reason, some ophthalmic surgeons do not recommend removal of the clear lens as a means of correcting myopia.
What Is the Role of Lattice Degeneration in Retinal Detachment Development?
Lattice degeneration is found in 6 to 8% of the general population and in 30% of eyes with retinal detachments.3 Given these statistics, it may seem dangerous to leave these lesions untreated; however, the literature has not reported clear benefit to their prophylactic treatment. For example, Byer found lattice lesions to be responsible for retinal detachments in only 3 of 423 eyes over an 11-year period.4 If a patient with bilateral lattice degeneration has had a retinal detachment in one eye, and if the eyes are highly myopic, the chances of subsequent retinal detachment in the fellow eye are compounded by these multiple factors.5 Prophylactic therapy of non-horseshoe breaks appears warranted only in cases where multiple risk factors exist, such as (1) pseudophakia with high myopia, (2) a history of a fellow eye retinal detachment; (3) tears with expanding retinal elevation; or (4) extensive vitreous traction.6
What Is the Association of Cataract Surgery to Retinal Detachment?
Cataract surgery by any method increases the risk of retinal detachment six to seven times more than non-surgically treated patients.7–9 Additional studies suggested that retinal detachment after cataract surgery is more common in young myopic patients and more common after laser posterior capsulotomy.10,11 Posterior capsule tears at the time of cataract surgery add to the risk of retinal detachment.
What Is the Role of Trauma in the Development of Retinal Detachments?
Patients who undergo blunt or penetrating injury to the eye have increased risk for rhegmatogenous retinal detachment.12 The presence of blood increases the risk of retinal detachment to 73% after penetrating injury. Most surgeons delay vitrectomy following penetrating trauma for at least 72 hours to allow for healing, further diagnostic evaluation, decreased uveal congestion, and spontaneous separation of the posterior hyaloid. Typically, a scleral buckle is placed at the time of vitrectomy surgery.13
What Does a Retinal Detachment Mean for the Fellow Eye?
Patients with a history of retinal detachment are at increased risk of developing a retinal detachment in the fellow eye.14 The incidence of retinal detachment in the fellow eye, despite treatment, ranges from 1.8 to 6.8%.15 The risk is heightened after cataract extraction.16 In one study, the frequency of retinal detachment was four times higher with aphakic patients compared with phakic patients in one study.17
How Does a Positive Family History Impact on Retinal Detachment Development?
Hereditary vitreoretinal disease may predispose to retinal detachment. Stickler syndrome is the most common inherited cause of retinal detachment, and in type 2 Stickler syndrome, a specific gene mutation has been linked to the COL2A1 locus.18 Hereditary diseases that predispose to retinal detachment often include risk factors such as myopia, lattice degeneration, and vitreous syneresis. A partial list of ocular systemic conditions associated with retinal detachment is outlined in Table 17–5.
Posterior Vitreous Detachments and Retinal Detachment
A degree of PVD is seen with most rhegmatogenous retinal detachments. If posterior vitreous separation occurs without forming a tear, the risk of retinal detachment decreases significantly.17 The prevalence of retinal detachment increases with age,19 but it also may occur in younger patients with myopia, inflammation, or previous intraocular surgery.20 A retinal tear will be found in about 15% of patients with new flashes or floaters caused by a PVD.21–23 If vitreous hemorrhage or pigment cells are observed in the vitreous, the risk of a retinal tear increases substantially.22
Hereditary disorders |
Wagner–Jansen–Stickler syndrome |
Marfan syndrome |
Familial retinal dialysis |
Ehlers–Danlos |
X-Linked juvenile retinoschisis |
Goldman–Favre |
Retinal conditions |
Lattice degeneration |
Axial myopia |
Retinoschisis |
What Is the Significance of a Symptomatic Retinal Tear?
About half of the symptomatic horseshoe tears (flap tears) will cause a retinal detachment unless treated adequately.24–26 Treating the lesion with adequate laser or cryotreatment nearly eliminates the chance of retinal detachment.
How Are Suspected Retinal Breaks Evaluated?
Retinal evaluation for suspected breaks or retinal detachment requires indirect ophthalmoscopy combined with scleral depression. Often peripheral retina can be seen despite the presence of vitreous hemorrhage. In certain cases, bed rest with the head elevated and bilateral eye patching has been advocated by specialists to hasten settling of the blood and improve the retinal view.27 For situations where the peripheral retina cannot be evaluated adequately, consultation with a specialist in vitreoretinal disorders is recommended. Patients at high risk should be educated about the warning symptoms of PVD and retinal detachment and the value of prompt evaluations.28
If a retinal tear develops into a rhegmatogenous retinal detachment, vision will be lost unless the detachment is repaired. Visual acuity usually improves and stabilizes after successful retinal reattachment. In patients who develop detachment of the macula, reading vision may not be achieved even with successful attachment of the retina. An approach to evaluation of patients with suspected retinal breaks is outlined in Table 17–6. In general, any patient about whom there is a concern of a retinal tear or retinal detachment should undergo prompt evaluation by a retinal specialist or ophthalmologist skilled in indirect ophthalmoscopy and scleral depression.
How Should the Patient with Retinal Breaks Be Managed?
Laser photocoagulation and cryotherapy are the standard treatments used in prophylactic management of retinal breaks. If symptomatic horseshoe breaks are found, treating them with these modalities is usually recommended. Nevertheless, not all reports suggest a high likelihood of horseshoe breaks developing into retinal detachments if they are chronic and asymptomatic. A study by Hyams and colleagues suggested that chronic horseshoe breaks generally do not benefit from prophylactic treatment.29 The use of judgment in choosing the correct management often requires experience and developed observational skills.
Treatment applied to a horseshoe tear should adequately surround the lesion, particularly around the horns (anterior extensions) of the tear. This will lead to development of a scar between the retina and adjacent tissues, stopping the movement of fluid through the hole. An inadequate treatment applied to horseshoe tears is the most frequent cause of subsequent retinal detachment.30–32 A cryoprobe offers the advantage of providing scleral depression and easily delivered treatment to the visualized lesion. It carries the disadvantage of requiring locally injected anesthesia. A horseshoe tear or a retinal dialysis should be treated by surrounding it with either cryotreatment or laser treatment. Laser is usually done at a slit lamp with a contact lens; however, laser applied by indirect ophthalmoscopic delivery also permits anterior treatment and makes the use of scleral depression possible. A method for determining the treatment of retinal breaks is outlined in Table 17–7.
What Is Done at the Follow-up Examination after a Posterior Vitreous Detachment Has Been Observed?
Patients who have an acute PVD should have the subsequent history and examination elements covered during follow-up examination. A change in visual symptoms or a new history of intraocular surgery should be documented. The visual acuity and the results of an evaluation of the status of the vitreous, macula, and peripheral fundus should be documented. If the patient has a vitreous hemorrhage or vitreoretinal traction, a reexamination should be scheduled within 3 to 6 weeks and generally requires the experience of a vitreoretinal specialist.33,34 A tear should be suspected in a patient who has a vitreous hemorrhage that obscures retinal details in the absence of conditions predisposing to hemorrhage, such as diabetes mellitus. A B-scan evaluation should be done and repeated at close intervals. No consensus of opinion exists regarding the optimal interval between visits in this situation. Frequent visits, for example, every 2 to 10 days, while the hemorrhage is settling or clearing help to determine whether the patient should be followed up or have treatment. This avoids missing a retinal detachment in a patient who has difficulty determining changes in vision. If any question regarding patient management develops, the skills of a vitreoretinal specialist should be sought.
| Topics and Elements to Include | Reason |
|---|---|
In the patient history: | |
Family history | It may reveal inherited vitreoretinal disease |
Prior eye trauma or surgery | Increased risk of retinal break formation |
Myopia | Increased risk of retinal break formation |
Lens status | Increased risk of retinal breaks with aphakia (no lens) and pseudophakia (lens implant) |
Symptomatic posterior vitreous detachment | Increased risk of retinal break formation |
In the examination: | |
Slit-lamp biomicroscopy | |
Status of the vitreous | To look for signs of a retinal break (hemorrhage/pigment cells/vitreous) |
Biomicroscopic macular examination | For visual prognosis: prognosis is poor if the evaluation macula is detached For plan formulation: to expedite retina consultation with a “macula on” retina detachment. Look for a Weiss ring (signifying a posterior vitreous detachment and increased risk of breaks) |
Confrontation visual fields | Detect a large retina detachment |
Peripheral indirect ophthalmoscopy | Look for breaks, or retinal detachment |
Measurement of refractive error | Evaluate for myopia (increased risk of retinal breaks) |
B-scan ultrasonography if the media is opaque | Define location and type of detachment, if present |
WHAT SHOULD BE DONE AT THE FOLLOW-UP EXAMINATION AFTER A RETINAL BREAK HAS BEEN TREATED?
If a patient is treated for a horseshoe retinal break, he or she should be asked to report back to the treating ophthalmologist if new visual field loss or floaters are observed. Although optimal intervals for follow-up evaluation have not been established, we suggest that patients be seen within 2 days to a week of treatment because chorioretinal scarring may take more than 5 days to develop. Based on the size of the break, if tractional forces or other general risk factors for retinal detachment are observed, the patient should be seen again within 6 weeks to look for subretinal fluid accumulation beyond the edge of the treatment. If tractional forces are minimal or a low risk of detachment exists, the interval can be extended. At follow-up visits, it also is important to examine the retina for possible new breaks.
| Lesion | Suggested Treatment |
|---|---|
| Horseshoe tear | Always treat |
| Dialysis | Always treat |
| Operculated tear | Treat rarelya |
| Atrophic hole | Treat rarelya |
| Lattice degeneration | Treat rarelya |
Adapted from the American Academy of Ophthalmology Preferred Practice patterns.
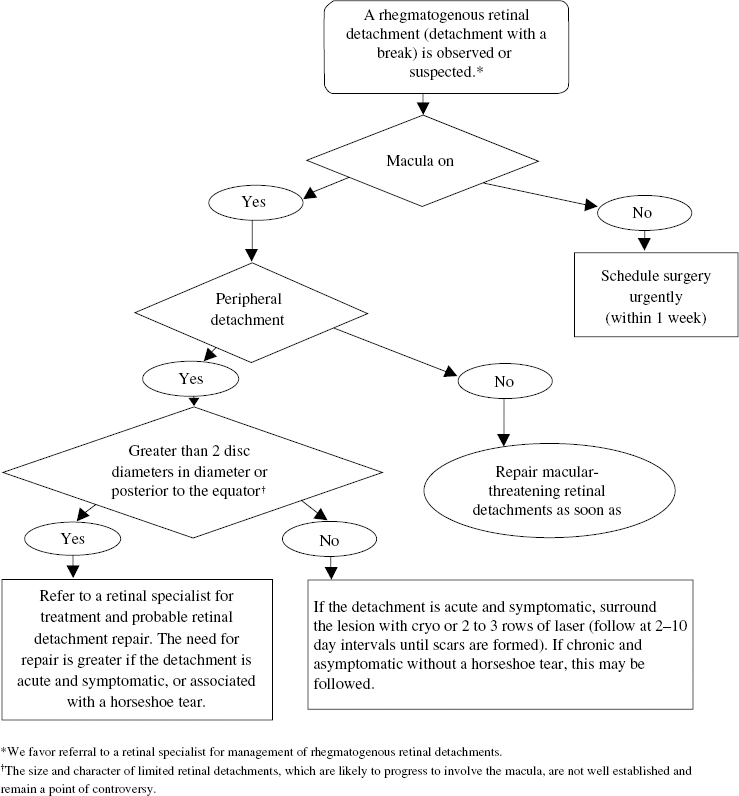
How Should a Rhegmatogenous Retinal Detachment Be Managed?
For the management of a rhegmatogenous retinal detachment, determining the timing of management requires knowing whether the event is chronic or acute and whether the macula is involved (Fig. 17–6). Chronic detachments produce slow changes in visual fields that the patient initially might not notice. In general, the patient with a large or posterior retinal detachment should be urgently sent to a vitreoretinal specialist for surgical evaluation. Timing of surgery may be important for improving final visual results. Some retinal detachments, such as shallow pediatric detachments, may be difficult to diagnose. If any question exists, especially in the face of decreased vision, one should err on the side of caution and refer the patient to a retinal specialist, even if the patient is inconvenienced by the time, travel, or distance involved in the referral examination.