and Yi Ning J. Strube2
(1)
Wright Foundation for Pediatric Ophthalmology and Adult Strabismus Medical Center, Los Angeles, CA, USA
(2)
Queen’s University, Kingston, Ontario, Canada
Keywords
Fornix surgeryLocking biteTwist knotLimbal surgeryHang-back techniqueVertical rectus muscle recessionLower lid retractor disinsertionThis chapter gives a detailed description of the rectus muscle recession procedure. Two conjunctival approaches are presented: fornix and limbal.
11.1 Fornix Surgery
The fornix incision is somewhat difficult to learn but, when mastered, it provides an excellent approach to the extraocular muscles. Unlike the limbal approach, the fornix incision is tucked away under the lid, and patients are very comfortable postoperatively. Because the limbal conjunctiva is intact, dellen formation is eliminated and cosmetic results are excellent. The fornix approach facilitates reoperation, especially when the first operation was a limbal surgery, because the fornix incision is behind the muscle insertion. This location avoids an anterior conjunctival scar and permits direct access to the muscle. Dr. Marshall M. Parks developed the very elegant fornix approach described in this chapter.
The strategy for obtaining proper exposure with the fornix approach is to rotate the muscle into the incision while stretching the incision towards the muscle insertion. Once the surgeon and assistant establish their team approach, the fornix approach provides excellent exposure. Fornix incisions should usually be avoided in patients older than 40 years of age because the conjunctiva is thin and friable. (See Chap. 10 for more on conjunctival incisions).
The fornix approach gives access to at least two muscles with a single incision. An inferior nasal incision provides access to the inferior and medial rectus. An inferior temporal incision provides access to the inferior rectus, lateral rectus, and the inferior oblique. A superior temporal incision provides access to the superior rectus, the lateral rectus, and the superior oblique tendon. A superior nasal incision provides access to the medial rectus, the superior rectus, and the nasal aspect of the superior oblique tendon. For horizontal rectus surgery, it is advisable to place the incision in the inferior fornix.
Regardless of the incision, posterior dissection or “cleaning” of the intermuscular septum and check ligaments is not indicated and does not enhance the recession. Recessions of the superior and inferior rectus muscles require some posterior dissection of fascial attachments to prevent secondary lid changes. (See Sect. 11.4 at the end of this chapter.)
11.1.1 Surgical Technique
Figures 11.1, 11.2, 11.3, 11.4, 11.5, 11.6, 11.7, 11.8, 11.9, 11.10, 11.11, 11.12, 11.13, 11.14, 11.15, 11.16, 11.17, and 11.18 demonstrate the fornix approach for a left medial rectus recession (surgeon’s view).
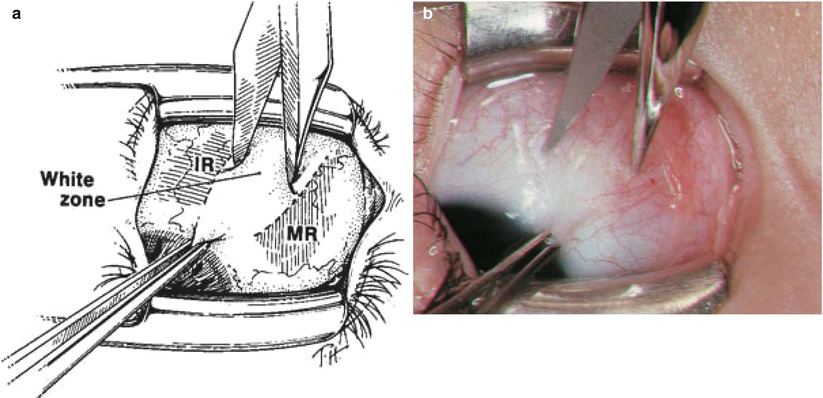
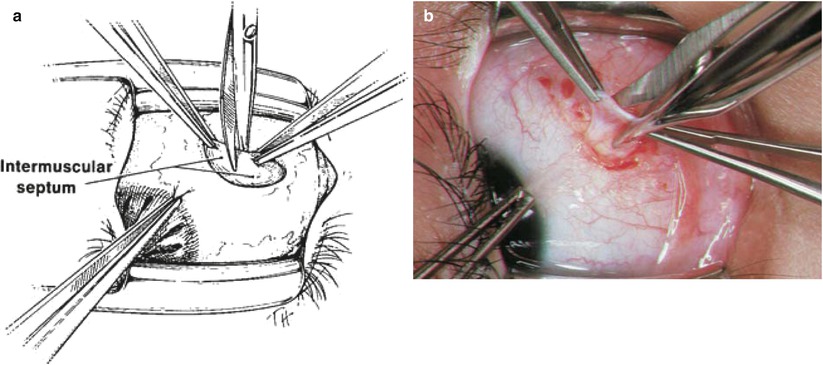
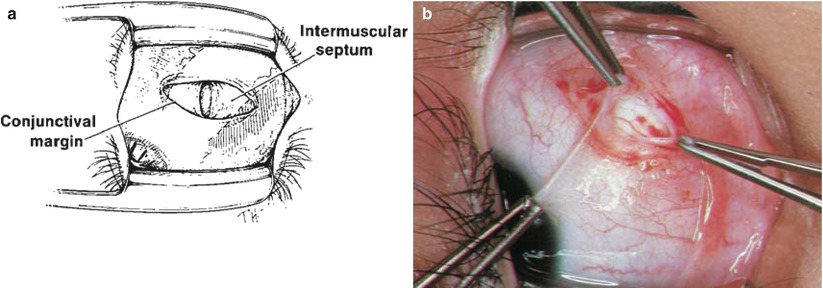
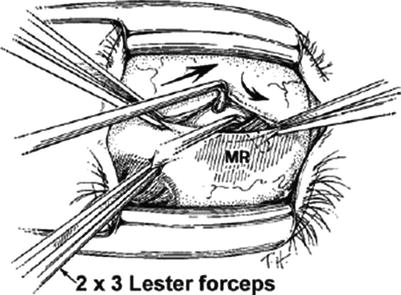
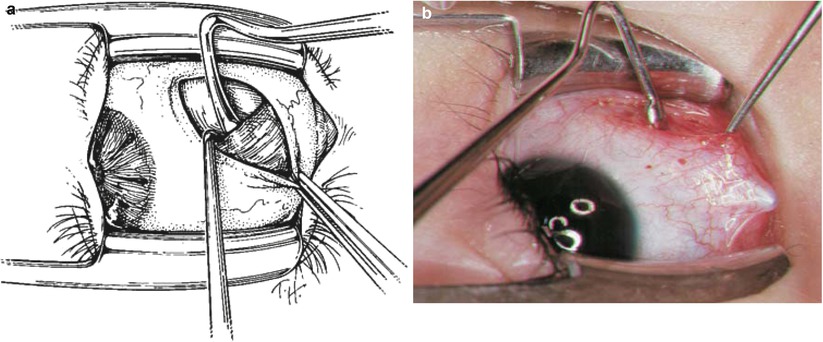
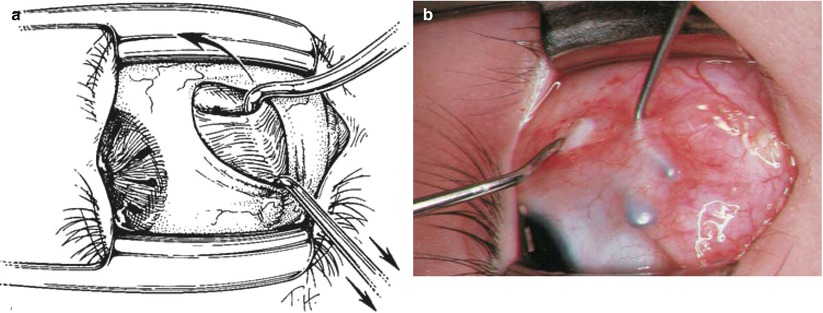
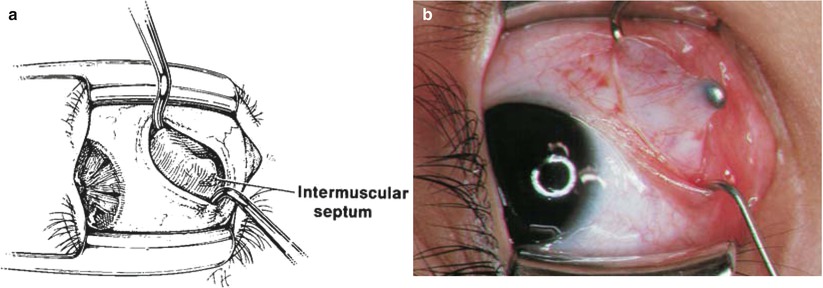
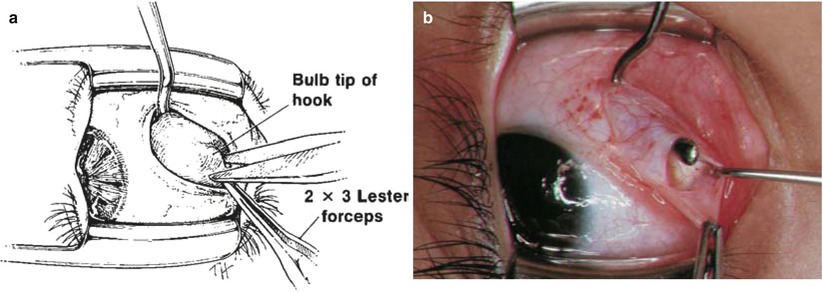
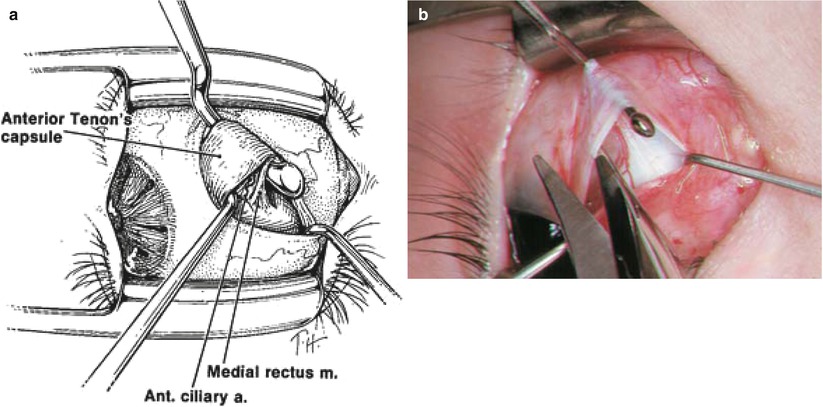
Fig. 11.1
(a) A 2 × 3 Lester forceps rotates the eye up and out to expose the inferior nasal quadrant and stabilize the eye. The incision is made by cutting straight down through the conjunctiva in the white zone between the inferior rectus (IR) and medial rectus (MR) muscles, approximately 8 mm posterior to the limbus. Extend the conjunctival incision from the inferior rectus muscle to within 1–2 mm of plica. (b) The location and alignment of the initial incision. Notice that the incision line is parallel to the lid speculum and just anterior to the orbital fat pad. Avoid cutting into the orbital fat and plica
Fig. 11.2
(a) With the eye drawn up and out, two 0.3 Castroviejo forceps pick up the intermuscular septum to form a tent, parallel to the conjunctival incision. Blunt Westcott scissors incise the intermuscular septum by cutting down over the tent, keeping both tips firmly against the sclera. This technique produces an incision in the intermuscular septum, perpendicular to the conjunctival opening. By keeping the scissors tips firmly on the sclera, a single snip will cut through all layers of intermuscular septum and gain immediate access to bare sclera. Only the blunt Westcott scissors are used for cutting through intermuscular septum on to sclera. (b) The blunt Westcott scissors making an incision through the intermuscular septum
Fig. 11.3
(a) The locations of the horizontal conjunctival incision and the vertical incision through the intermuscular septum. It is important to cut down through full-thickness intermuscular septum to expose bare sclera. (b) The fornix incision, exposing bare sclera. The two forceps are grasping intermuscular septum
Fig. 11.4
With the 2 × 3 Lester forceps stabilizing the eye in elevation and abduction, the medial rectus (MR) is hooked with a small Stevens hook. Place the Stevens hook directly perpendicular to sclera and pass the hook posteriorly and then superiorly, rotating the hook underneath the inferior border of the medial rectus muscle (arrows). Starting with the hook perpendicular to the sclera ensures that the tip of the muscle hook will remain in contact with the sclera and slide under the muscle
Fig. 11.5
(a) Once the muscle is hooked with the small hook, the 2 × 3 Lester forceps is released and a large Jameson hook is passed under the muscle to replace the Stevens hook. Make sure to keep the tip of the Jameson hook against the sclera and perpendicular to the muscle fibers to avoid splitting muscle. (b) A small Stevens hook behind the medial rectus, pulling the muscle straight up off the sclera. A large Jameson hook is poised to be passed directly under the Stevens hook, parallel to the muscle insertion. After the Jameson hook is passed, the Stevens hook is removed
Fig. 11.6
(a) Once the muscle is hooked, the conjunctival incision is reflected over the tip of the Jameson hook to expose the muscle. Place the small hook at the nasal end of the conjunctival incision and, keeping the hook flat on the surface of the muscle, pull the conjunctiva over the end of the Jameson hook. This is a bimanual technique, with the Jameson hook rotating inferiorly and temporally towards the incision while the small Stevens hook simultaneously pulls the conjunctiva superiorly over the tip of the Jameson hook (arrow). (b) A small Stevens hook underneath the conjunctiva, slowly slipping the conjunctiva toward the bulb tip of the Jameson hook. The Jameson hook simultaneously rotates inferiorly and temporally so that the bulb tip rotates toward the incision. Keep the tip of the Jameson hook up to prevent the muscle from slipping off the end of the hook
Fig. 11.7
(a) The small hook folds the conjunctiva over the bulb tip of the Jameson hook. Notice the perpendicular position of the tip of the small hook, which is now facing the end of the Jameson hook. The tissue over the end of the Jameson hook is superonasal intermuscular septum. (b) The conjunctiva reflected over the end of the Jameson hook. The Jameson hook is directed tip-up and rotated inferiorly into the area of the initial incision. The white tissue emanating over the bulb tip of the Jameson hook is superonasal intermuscular septum
Fig. 11.8
(a) The 2 × 3 Lester forceps is used to grasp the intermuscular septum (not the conjunctiva) at the end of the Jameson hook, and the small Stevens hook is removed from the conjunctiva. A hole in the intermuscular septum, between the bulb of the Jameson hook and the tip of the 2 × 3 Lester forceps, is cut with the Westcott scissors. The remnant of intermuscular septum is swept over the bulb of the Jameson hook to bare the end of the hook. (b) The bared bulb end of the Jameson hook. Notice that the 2 × 3 Lester forceps continues to pull intermuscular septum superiorly, opening the hole in the intermuscular septum. A small Stevens hook is placed within the hole onto sclera to maintain the opening in the intermuscular septum
Fig. 11.9




(a) A second Stevens hook is inserted into the hole in the intermuscular septum, down to bare sclera. With the tip of this hook firmly on the sclera, it is swept anteriorly around the superior pole of the medial rectus muscle insertion. This maneuver of sweeping around the superior muscle pole is called the “pole test.” If the muscle is inadvertently split, superior fibers of the medial rectus will snag the small hook as it sweeps anteriorly. A restricted pole test indicates that residual muscle is not on the hook and a split tendon is present (see Fig. 10.8). The Stevens hook pulls the anterior Tenon’s capsule so it can be excised with the Westcott scissors. (b) The Westcott scissors removing anterior Tenon’s capsule from the medial rectus tendon. The pole of the medial rectus tendon is identified by the presence of an anterior ciliary artery emanating off the tendon insertion. The blade of the Westcott scissors is slid between anterior Tenon’s capsule and medial rectus tendon to excise anterior Tenon’s capsule. Be careful not to inadvertently cut conjunctiva or tendon. The Stevens hooks are rotated together in front of the rectus muscle tendon to expose and excise the entire width of anterior Tenon’s capsule. This maneuver cleans the muscle insertion so that sutures will be passed through true tendon rather than through the anterior Tenon’s capsule, which could cause a slipped muscle
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
