and Yi Ning J. Strube2
(1)
Wright Foundation for Pediatric Ophthalmology and Adult Strabismus Medical Center, Los Angeles, CA, USA
(2)
Queen’s University, Kingston, Ontario, Canada
Keywords
Full tendon tuckIatrogenic Brown’s syndromeHarada-Ito ProcedureIntraoperative adjustment of torsionFull tendon superior oblique tuckSuperior oblique tendon plication18.1 Physiology of Superior Oblique Tendon Tightening Procedures
The superior oblique tendon can be functionally divided into the anterior one third, which is responsible for intorsion, and the posterior two thirds, which is responsible for depression and abduction (Fig. 18.1). Superior oblique tightening procedures are based on this physiologic division and either tighten the whole tendon (i.e., full tendon tuck) or tighten the anterior tendon fibers (i.e., the Harada-Ito procedure).
Fig. 18.1
The anterior fibers of the left superior oblique tendon (shaded) course close to the equator of the eye and are responsible for intorsion. The posterior fibers are behind the equator and lift the back of the eye toward the trochlea, bringing about abduction and depression
18.1.1 Full Tendon Tuck
A full tendon tuck, which tightens both anterior and posterior fibers, enhances all three functions of the superior oblique muscle. This operation is useful for correcting extorsion, hyperdeviation that increases in the field of action of the superior oblique, and convergence in down gaze. Tightening of the entire superior oblique tendon can lead to limited elevation in adduction, however, or an iatrogenic Brown’s syndrome. Care must be taken to balance the superior oblique tightening against an induced Brown’s syndrome by performing intraoperative forced ductions of the superior oblique tendon after tucking.
18.1.2 Harada-Ito Procedure
There are clinical circumstances that require selective correction of extorsion without a significant change in vertical or horizontal alignment. A full tendon tuck in this situation is not appropriate because it would induce a hypotropia, and possibly cause an iatrogenic Brown’s syndrome. The Harada-Ito procedure is designed to selectively correct extorsion by tightening only the anterior superior oblique fibers. The “Harada-Ito plus” procedure incorporates a few millimeters of the more posterior tendon, and improves posterior tendon function. This procedure can correct small hypertropias in addition to extorsion.
18.2 Surgical Techniques: Isolation and Exposure of the Superior Oblique Tendon
Figures 18.2, 18.3, 18.4, 18.5, and 18.6 illustrate the technique for the isolation and exposure of the superior oblique tendon—specifically, the surgeon’s view of surgery on the left eye.
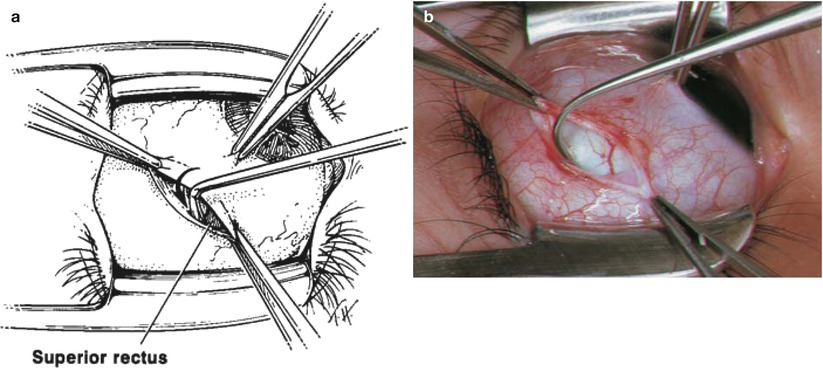
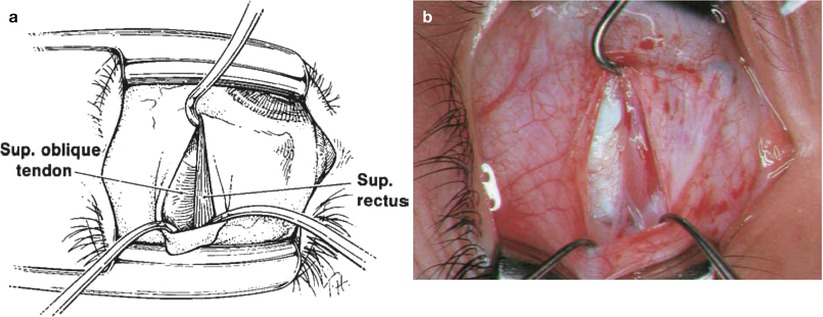
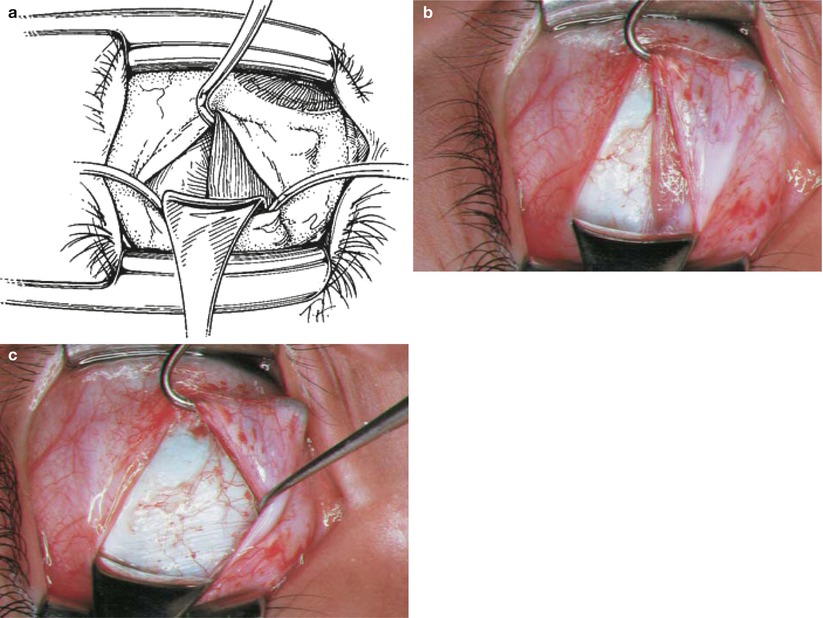
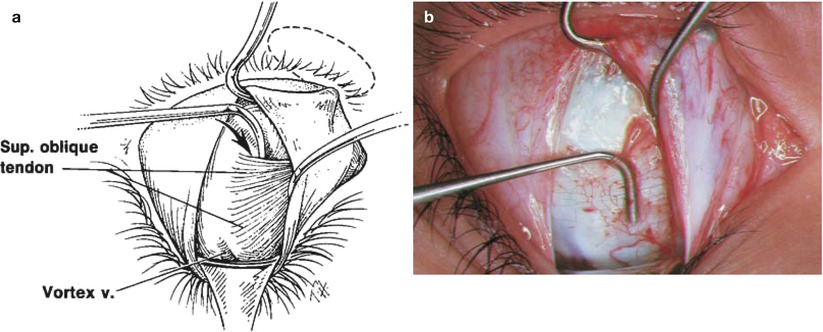
Fig. 18.2
With the eye depressed and adducted by the assistant, a superior temporal fornix incision is made approximately 8 mm posterior to the limbus, as described in Chap. 11. LR lateral rectus, SR superior rectus
Fig. 18.3
(a) The temporal border of the superior rectus muscle is identified visually and hooked at the insertion, first with a small Stevens hook, and then with the larger Green or Jameson hook. Do not sweep posteriorly when hooking the superior rectus muscle, as the anterior fibers of the superior oblique tendon insertion will be inadvertently hooked or even disinserted. The idea is to preserve the integrity of the entire superior oblique insertion. (b) The Stevens hook on bare sclera ready to hook the lateral pole of the left superior rectus muscle insertion. A small triangle of the right superior rectus muscle is seen between the tip of the hook and the forceps to the right
Fig. 18.4
(a) Using the Jameson hook to retract the superior rectus, the globe is maximally depressed, and the incision is opened with two small hooks to expose the temporal border of the superior rectus muscle. A limited dissection of check ligaments overlying the temporal third of the superior rectus muscle may be necessary to gain posterior exposure. Stay on top of the muscle, being careful not to dissect fascial tissue off the temporal sclera. (b) The temporal border of the superior rectus muscle with a large hook retracting the superior rectus muscle to rotate the globe inferiorly. The temporal border of the superior rectus muscle can be seen. The fine tissue overlying the sclera just temporal to the superior rectus muscle represents the fanned-out portion of the superior oblique tendon covered with a thin layer of intermuscular septum. Do not clean the temporal aspect of the superior rectus muscle and do not excise the temporal intermuscular septum. Because it is closely adherent to the fanned-out portion of the superior oblique tendon, removing the intermuscular septum in this area often inadvertently removes the superior oblique tendon
Fig. 18.5
(a) A Desmarres retractor is placed into the incision, and the lid speculum is removed to improve posterior exposure. (b) The photograph shows the temporal border of the superior rectus muscle and superior oblique tendon covered with intermuscular septum. Note that it is difficult to visualize the fibers of the superior oblique insertion, and the tissue temporal to the superior rectus muscle easily can be mistaken for intermuscular septum. (c) A small hook is placed underneath the belly of the superior rectus muscle and is retracted nasally to expose the fibers of the superior oblique tendon. The superior oblique tendon fibers are identified by their parallel pattern and their white, glistening appearance. These fibers run under and perpendicular to the fibers of the superior rectus muscle
Fig. 18.6
(a) The anterior fibers of the superior oblique tendon are hooked with a small Stevens hook along the temporal border of the superior rectus muscle. The tendon is exposed and ready for surgical manipulation. (b) A small Stevens hook is shown behind the anterior fibers of the superior oblique tendon. The vortex vein can be seen as a purple coloration in the sclera, just under the Desmarres retractor, at the most posterior aspect of the incision
18.3 Harada-Ito Procedure
The Harada-Ito procedure tightens the anterior superior oblique tendon fibers, thus inducing intorsion without significantly affecting the posterior tendon functions of abduction and depression. Described below are two techniques for tightening the anterior fibers: the disinsertion technique and the classic Harada-Ito procedure (Fig. 18.7).
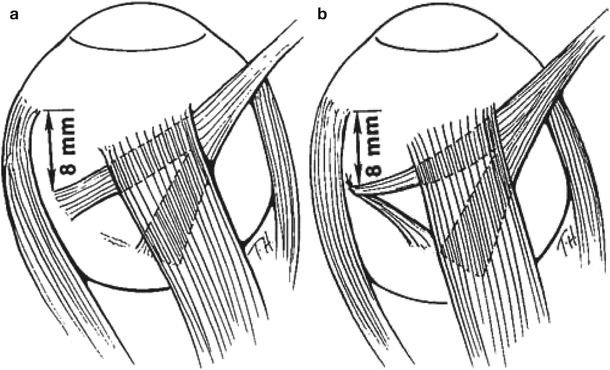
Fig. 18.7




(a) With the disinsertion Harada-Ito technique, the anterior fibers of the superior oblique tendon are sutured, then disinserted and moved anteriorly and laterally, to be secured to sclera at a point 8 mm posterior to the superior border of the lateral rectus insertion. Lateralizing the anterior fibers intorts the eye, thus correcting extorsion. (b) In the classic Harada-Ito procedure, the anterior superior oblique tendon fibers are looped with a suture and displaced laterally without disinsertion. The anterior fibers of the superior oblique tendon are sutured to sclera 8 mm posterior to the superior border of the lateral rectus muscle
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
