and Yi Ning J. Strube2
(1)
Wright Foundation for Pediatric Ophthalmology and Adult Strabismus Medical Center, Los Angeles, CA, USA
(2)
Queen’s University, Kingston, Ontario, Canada
Keywords
Intermittent exotropiaHigh hypermetropia with exotropiaBasic X(T)True divergence excess X(T)Pseudodivergence excess X(T)Patch testConvergence insufficiencyV-patternA-patternX-patternSensory XTCongenital XT5.1 Intermittent Exotropia
Intermittent exotropia—X(T)—is a large exophoria that intermittently breaks down to an exotropia. Occluding one eye breaks fusion and will manifest the exotropia (Fig. 5.1). When fusing, the eyes are straight and stereo acuity is excellent, usually 40 s of arc. When tropic, there is large, hemiretinal suppression of the deviated eye. It is common for patients to show a preference for one eye, but the clinician should resist the temptation to label the deviation as a right or left exotropia, as the deviated eye can easily be changed by covering the dominant eye. Patients with late onset of exotropia during late childhood or adulthood may experience diplopia when tropic. The exotropia is typically manifest when the patient is fatigued, daydreaming, or ill. Approximately 80 % of intermittent exotropia patients will show progressive loss of fusion control and an increase in the exotropia over several months to years. Adult patients can have extremely large deviations. The patient in Fig. 5.2 has alternating intermittent exotropia but is able to fuse intermittently.
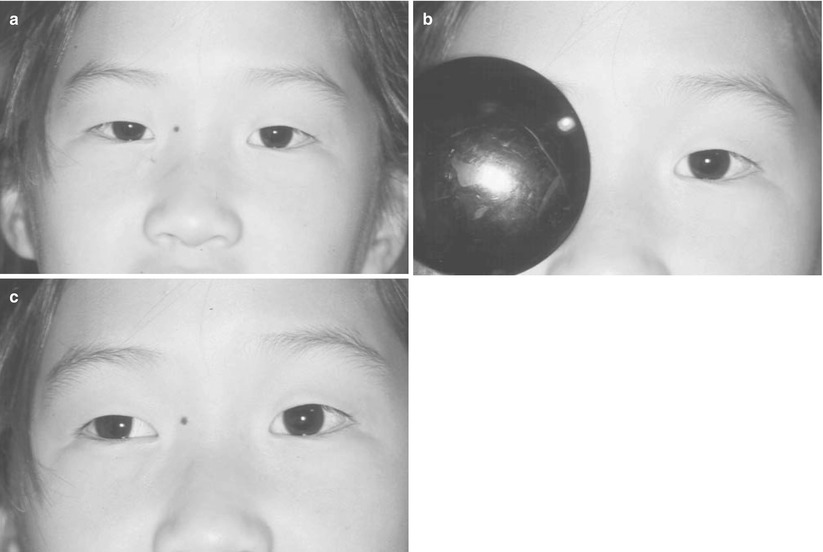

Fig. 5.1
Child with an intermittent exotropia. (a) The patient is fusing with straight eyes. (b) Covering the right eye dissociates the eyes and breaks fusion. (c) Fusion is broken and patient manifests the latent exotropia
Fig. 5.2
Adult patient with childhood intermittent exotropia that increased over time to a large-angle, constant exotropia. Despite the large-angle exotropia, she was able to fuse intermittently. (a) Patient is fixing with the right eye; the left eye is deviated. (b) Patient is fixing with the left eye; the right eye is deviated
5.1.1 Clinical Features
Most common form of exotropia
Usually presents after 1 year of age
Large exophoria (usually 25–40 PD) that spontaneously becomes manifest
High-grade stereo acuity when fusing (40 s arc); suppression when tropic
Squints one eye to bright light
High hypermetropia with exotropia (rare subtype of intermittent exotropia)
5.1.2 Etiology
The cause of the underlying exotropia is unknown, but the control of the deviation and the high-grade stereo acuity can be explained on the basis of strong fusional convergence. Fusional convergence is naturally strong (25–30 PD), so exodeviations are better controlled than esodeviations, as divergence amplitudes are small (6–8 PD).
5.1.3 Clinical Evaluation
5.1.3.1 Ductions
Adduction should be full.
5.1.3.2 Versions
Check for oblique dysfunction and “A” or “V” patterns.
5.1.3.3 Amblyopia
Amblyopia can occur but is rare, usually associated with anisometropia. If decreased vision is present, think about an organic cause (e.g., optic nerve disease).
5.1.3.4 Measure the Deviation
Use prolonged prism alternate cover testing for far distance fixation (at least 20 ft) and near fixating on an accommodative target, to measure the deviation. Prolonged cover testing helps to break down tonic fusion and reveal the full deviation. Consider the patch test for patients with a divergence excess pattern, discussed below.
5.1.3.5 Cycloplegic Refraction
A cycloplegic refraction is important, as high hypermetropia with hypoaccommodation can cause an intermittent exodeviation. The treatment is to prescribe the full hypermetropic correction.
5.1.4 Nonsurgical Treatment
In general, nonsurgical treatment does not work very well for intermittent exotropia. Indications for nonsurgical treatment include convergence insufficiency, small-angle exophoria, interim treatment prior to surgery, and high hypermetropia with exotropia. A few nonsurgical therapies can be considered for these patients:
Part-time monocular occlusion of the dominant eye, 3–4 h a day. This form of antisuppression therapy works by stimulating the nonpreferred eye. In patients with equal ocular preference, alternate eye patching is indicated.
Over minus: Prescribe −1.50 to −2.50 sphere more than required by cycloplegic refraction. The increased accommodative convergence may help to control the intermittent exotropia, but it is usually effective only for small deviations in myopic patients.
Orthoptics: Convergence exercises (pencil push-ups or base out prisms) are the treatment of choice for convergence insufficiency. Orthoptics are usually not helpful for correcting the distance exodeviation.
5.1.5 High Hypermetropia with Exotropia
Patients with hypermetropia (>+4.00 sphere OU) may present with a small exotropia. These patients have some degree of bilateral amblyopia and are hypoaccommodators. Their small exotropia is secondary to poor accommodation and deficient convergence. Treatment is to prescribe the full hypermetropic correction. By prescribing the full plus, vision and accommodation improve, thus improving convergence and control of the exotropia. Surgery is indicated if there is a residual exotropia after prescribing full hypermetropic correction. Do not be afraid to prescribe the full plus!
5.1.6 Preoperative Evaluation
Indications for surgery:
Increasing tropia phase with diminished fusion control
Poor fusion recovery on cover/uncover testing
Exotropia that is manifested more than 50 % of waking hours
The size of the deviation is of less importance but, in most cases, the exotropia should be >15 PD
Children under 4 years of age are at risk of developing postoperative amblyopia from a consecutive esotropia. It is probably best to postpone surgery until 4 years of age unless the patient demonstrates progressive loss of fusion control. A consecutive esotropia in these young children must be followed closely to check for development of postoperative amblyopia.
5.1.7 Surgical Treatment
The procedure of choice for all types of intermittent exotropia (see classification later in this chapter) is bilateral lateral rectus recessions. Symmetrical surgery is preferred over a monocular recession-resection procedure because the deviation is comitant, and bilateral surgery gives a comitant result. A recession-resection procedure, on the other hand, causes horizontal incomitance, inducing an esotropia and diplopia on gaze to the side of the recession–resection. The incomitance may partially dissipate over time, but adults often complain of persistent diplopia on side gaze.
Small hyperphorias (<5 PD) are commonly associated with intermittent exotropia. These small hyperphorias can be ignored if they are not associated with oblique dysfunction, as they disappear after correction of the exotropia with bilateral lateral rectus recessions.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


