3. The stapes should be present. A columella placed in front of the tympanic isthmus with the possibility of adhesion formation between the columella and the surrounding structures, especially the facial eminence, may obstruct the tympanic isthmus and hamper ventilation of the cavity.
4. There should be at least some mucosal lining of the medial attic wall, allowing rapid mucosal regeneration. This is perhaps the most important criterium, because the mucosa is often removed during cholesteatoma removal. If no mucosa is preserved, it has to regenerate from the tympanic cavity, which takes time. In the meantime, the denuded bone may become covered by granulations, blocking the attic, and causing the formation of adhesions between the attic and the newly formed ear canal wall, which is then pulled posteriorly — a mechanism similar to that seen in the formation of postoperative attic retraction after canal wall–up mastoidectomy (Chapter 8, Fig. 374).
In addition, mucociliary clearance from the antrum via the attic is eliminated, leading to the accumulation of secretions in the attic.
5. Technically, it should be possible to fix the graft material to the anterosuperior wall of the cavity and to the facial ridge, so that it “hangs” between these two structures, resulting in a wide and stable communication between the mastoid cavity and the tympanic cavity. A low facial ridge, and a large distance between the facial ridge and the anterosuperior wall of the cavity, are thus unsatisfactory conditions. It is best for the bony bridge, or at least part of it, to be present, providing some support for the new ear canal wall and ensuring connection between the drum and the facia.
6. The graft material, preferably autogenous, should be large enough to cover the entire posterior ear canal wall region, i. e., the temporalis muscle fascia should be at least 2×3 cm, with large plates of cartilage or cortical bone. This is not easy to achieve in an ear that has been previously operated on. The methods and problems of harvesting autogenous grafts are described in Vol. 1, Chapter 6.
Reconstruction with Fascia
Retroauricular Approach, with Palva Flap
Reconstruction with a Palva flap is possible only via the retroauricular approach. Reconstruction with temporalis muscle fascia is the basic method, with the fascia used to cover other grafts in combinedgraft reconstructions. The principle is to create a tight connection between the drum medially, the bony wall superiorly, the facial ridge inferiorly, and the meatal soft tissues laterally (Fig. 814). In addition, canal skin flaps must be placed on the meatal aspect of the fascia, and although theoretically this is easy to achieve, practically it is far more complicated, mainly because any pressure on the fascia must be avoided in order to maintain the opening between the tympanic cavity and keep the attic open to ventilate the cavity. For the same reason, any support for the fascia from the attic or from the cavity. e. g., by filling the cavity with Gelfoam balls, is not desirable, since this may obstruct the attic. However, sometimes this can not be avoided.
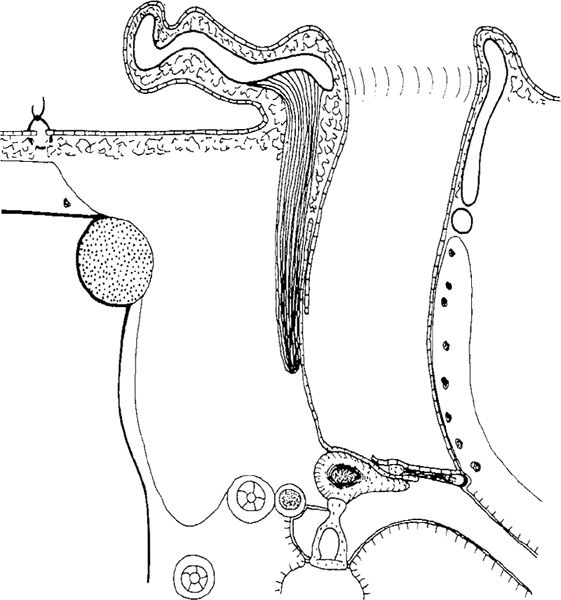
Fig. 814 Reconstruction of the ear canal with fascia and Palva flap, in a side view. A large fascia is placed under the drum remnant, covering the interposed incus. It then turns laterally to form the new ear canal. A Palva flap is placed behind the fascia. The epithelial flaps cover the meatal side of the fascia. The cavity is intended to be ventilated
After ossiculoplasty and preparation of the ear canal skin flaps used to cover the fascia, a few Gel-foam balls are placed in the attic temporarily to maintain the space for ventilation, as well as to support the fascia (Fig. 815). A 2×3–cm semi-dry and malleable sheet of fascia is placed onto the cavity walls and into the tympanic cavity. Semi-dry fascia is the easiest to handle during placement under the drum remnant; dry fascia has to become softer and malleable in order to be manipulated. The fascia is carefully adapted to the undersurface of the drum (Fig. 816). The epithelial flaps are replaced, fixing the fascia (Fig. 817), and the flaps are then fixed with Gelfoam balls. The Gelfoam is initially placed over the region of the bridge, to secure a connection between the fascia and the interposed incus (Fig. 818) and also to avoid lateralization of the fascia in this region. The ear canal is gradually packed with Gelfoam and small pieces of gauze moistened with cortisone and Terramycin ointment (Fig. 819), while the fascia is still being carefully adapted to the remaining bony structure of the ear canal. After the ear canal is packed, the fascia is gently pulled laterally and adapted to the canal wall, bringing it as far laterally as possible, so that the posterior ear canal skin flap can cover it from the meatal side (Fig. 820). Communication between the tympanic cavity and the mastoid cavity is thus secured, allowing removal of the Gelfoam balls from the attic region.
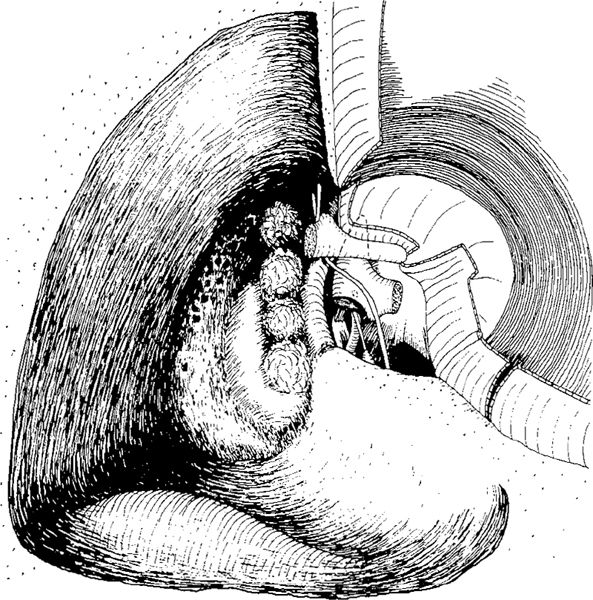
Fig. 815 A canal wall–down mastoidectomy cavity with low facial ridge, prepared for reconstruction and ventilation. The stapes is present, the incus is interposed, the epithelial flaps are elevated, and Gelfoam balls have been temporarily placed in the attic to support the fascia during reconstruction. They are removed after fixation of the fascia to the bone
The self-retaining retractor that held the auricle anteriorly during the retroauricular approach, is now removed. The previously prepared Palva flap is gradually pushed into the cavity, strengthening the posterior canal wall as the auricle is replaced in its original position (Fig. 821). Some further packing of the ear canal is required, but this should not be too firm in order to avoid displacement of the fascia posteriorly. The auricle is placed in its proper position (Fig. 814), and the postauricular wound is sutured.
The ear canal pack is not touched until three weeks after the operation, when is it removed. The patient is asked to perform the Valsalva maneuver from the fourteenth postoperative day, as long as the Valsalva is positive preoperatively; if not, he or she should start after one week. The final situation after a successful operation resembles Figure 814.
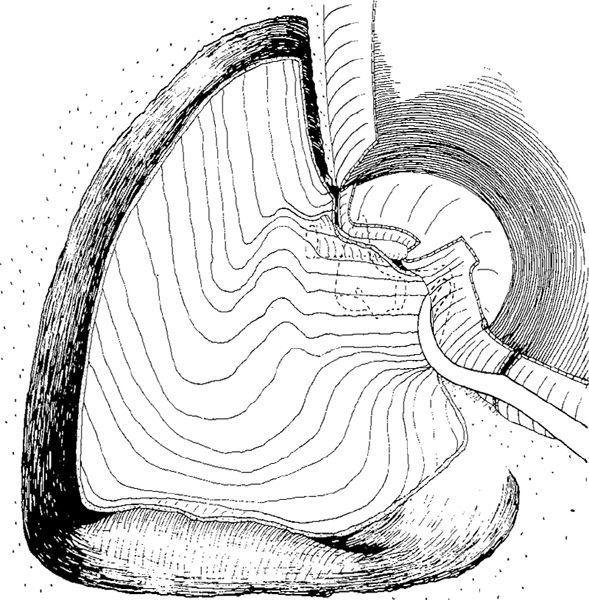
Fig. 816 A large piece of fascia is placed on the cavity walls. It is adapted to the drum remnant as an underlay graft, both anteriorly and posteriorly
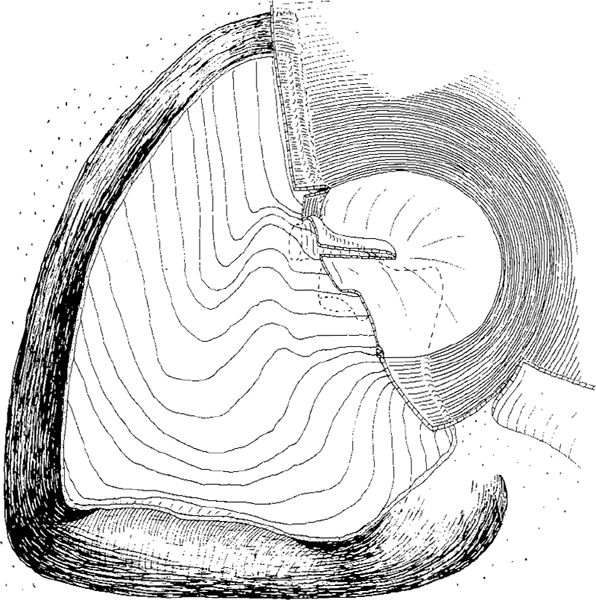
Fig. 817 The epithelial flaps are replaced, and will be fixed with Gelfoam balls. The fascia will be turned laterally to form the ear canal
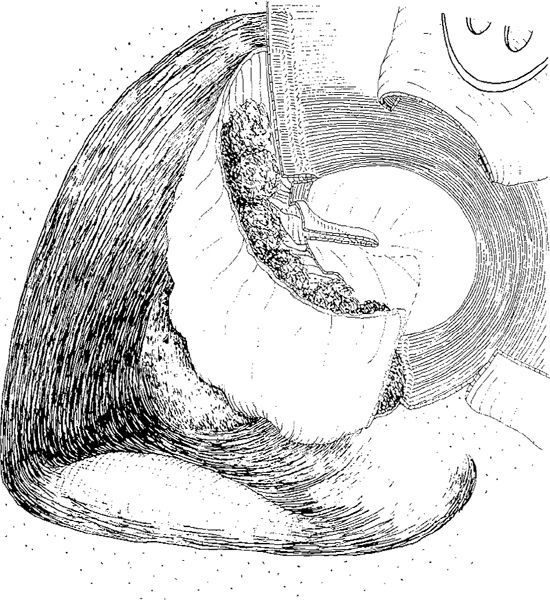
Fig. 818 The fascia has been turned laterally, and the ear canal is gently packed with Gelfoam balls to maintain the upper part of the ear canal and secure contact to the incus
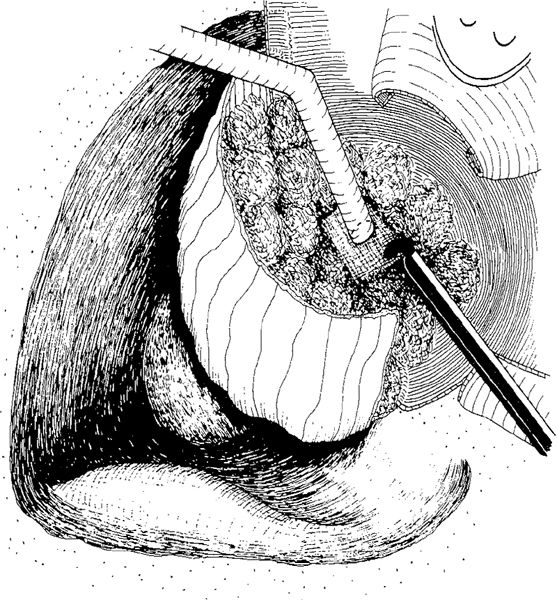
Fig. 819 Further packing of the ear canal and adaptation of the fascia to the superoanterior wall of the cavity and the facial ridge
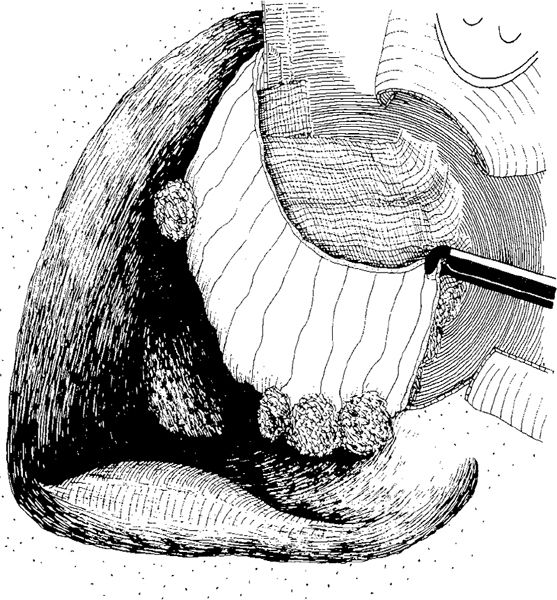
Fig. 820 After the ear canal is packed, the fascia is pulled out with a forceps, elongating the ear canal wall and further adapting the fascia. The reconstructed ear canal wall is now ready to be strengthened with a Palva flap
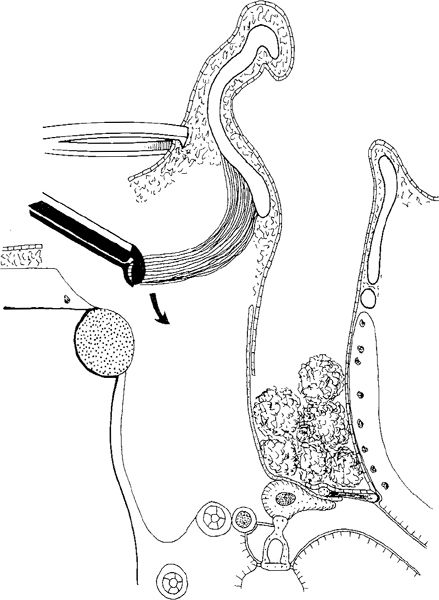
Fig. 821 The self-retaining retractor is removed. The Palva flap, prepared at the beginning of the procedure, is freed and brought down (arrow) onto the posterior aspects of the fascia, while the auricle is replaced in its original position. The ear canal will be packed with Gelfoam balls and a gauze strip moistened with oxytetracycline and hydrocortisone ointment (Terra-Cortril) for three weeks
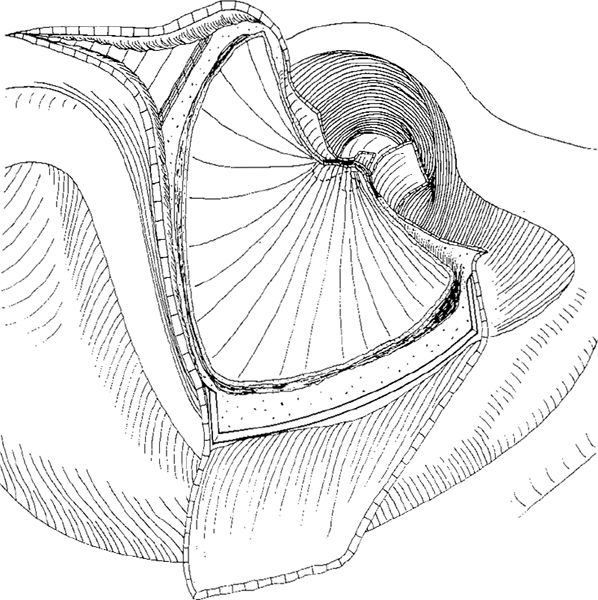
Fig. 822 Reconstruction of the ear canal wall in an endaural approach. After ossiculoplasty with an incus interposed between the malleus handle and the stapes, a large piece of fascia is placed under the edges of the posterior perforation as an underlay graft. Fascia covers the facial ridge and the superoanterior and posterior edges of the cavity. A small Körner meatoplasty, with resection of a strip of conchal cartilage, is performed
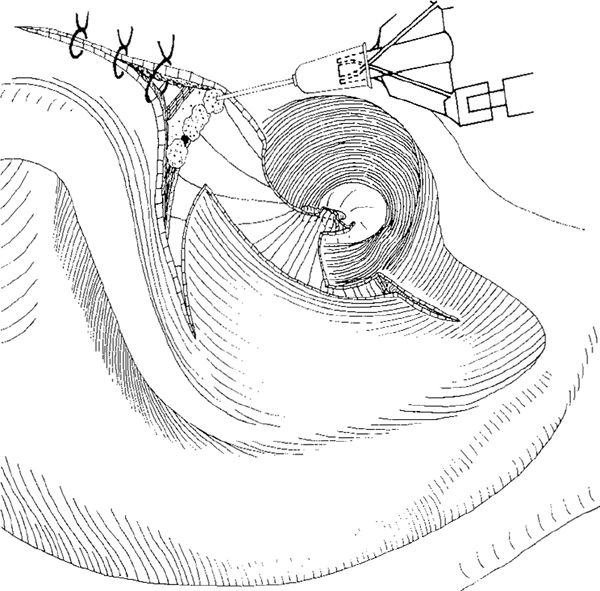
Fig. 823 The epithelial flaps are replaced; first, the tympanomeatal flap, and then the superior and the lateral flaps, fixing the fascia. The fascia is laterally fixed with fibrin glue placed between the bone and the fascia
One to six years after reconstruction of the ear canal wall using a Palva flap in 12 prognostically favorable ears with old radical cavities, 19% were dry, and 66% had a ventilated cavity (Tos 1977).
Smith et al. (1986) performed canal wall reconstruction using a large piece of fascia and a Palva flap, totally obliterating the cavity behind the flap with Gelfoam, with relatively good results: of 30 patients operated upon, the reconstructed ear canal wall was intact in 53% of cases two years postoperatively, and was within the position normally occupied by the bony posterior canal wall. In the remainder, a variable degree of retraction of the membranous posterior canal wall was noted. This indicates that a significant amount of Gelfoam can be placed in the cavity.
This reconstruction of the ear canal is an important element of several obliteration techniques.
Endaural Approach
Reconstruction of the ear canal using fascia in the endaural approach after a canal wall–down mastoidectomy is technically much easier than in the retroauricular approach. After canal wall–down mastoidectomy and after ossiculoplasty, a large piece of fascia is placed as an underlay graft to cover the perforation (Fig. 822). The fascia covers the facial ridge laterally, and is then placed over the posterior edge of the cavity and laterally over the mastoid tegmen. The canal skin flaps are replaced superiorly, carefully fixing the fascia. The laterally based ear canal skin flap (Körner flap) is pulled back, covering as much of the fascia as possible, and sutures are placed, partially closing the Heermann B incision. The fascia is fixed in position with Gelfoam balls. Some surgeons fix the fascia with fibrin glue (Pannis et al. 1979) placed at the junction between the bone and the fascia, preferably under the fascia (Fig. 823). In the endaural approach, however, the ear canal wall is not strengthened with a Palva flap, which cannot be harvested.
It is wise to perform a Körner meatoplasty with resection of conchal cartilage (Fig. 822) in case of future retraction of the fascia, which often occurs, resulting in an open cavity situation.
Reconstruction with Autogenous Cartilage
In total reconstruction of the ear canal wall, autogenous tragal cartilage, allogenous septal cartilage, and allogenous knee cartilage have been used. In contrast to scutumplasty, large pieces of cartilage are needed to reconstruct the entire ear canal wall.
Tragal Cartilage
Even though tragal and conchal cartilage are the most commonly used graft materials in scutumplasty (Chapter 6, Figs. 349–359), only small series have been published using tragal cartilage.
Endaural approach. Eviatar (1978) reconstructed the ear canal wall in ten cases using tragal cartilage and perichondrium after conservative radical surgery. In the endaural approach, the canal skin is elevated and widely preserved (Fig. 824). A compound cartilage–perichondrium graft, with the perichondrium partially elevated from one side, is placed in the original position of the ear canal wall, in contact with the head of the malleus. The perichondrium is then placed as an underlay graft under the drum remnant, closing the perforation (Fig. 825). The skin flaps are replaced, and the ear canal is thus partially reconstructed. Laterally, there is still a defect that needs to be covered (Fig. 826). In Eviatar’s method, it is evident that the tragal cartilage cannot reach from the superior to the inferior cavity wall, and additional tissue, e. g., a large piece of fascia, is required to cover the defect between the tragal cartilage and the facial ridge.
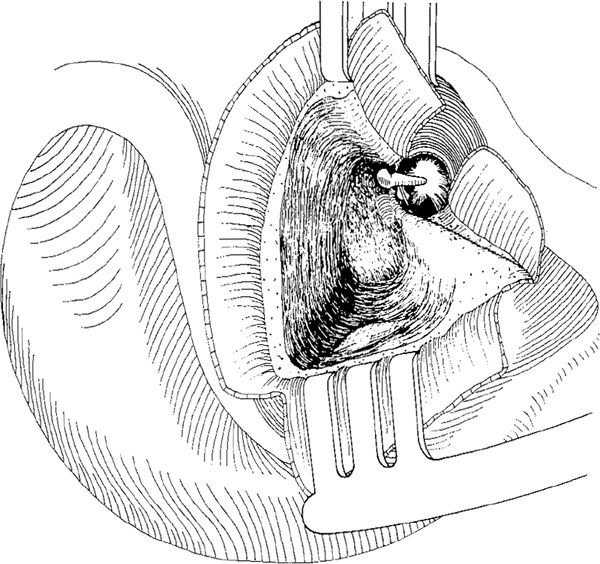
Fig. 824 Ear canal wall reconstruction with tragal cartilage (Eviatar). In the endaural approach, the epithelial lining of the canal wall–down cavity is elevated, and large skin flaps are created: inferior, anterior, lateral, and posterior
Retroauricular approach. The present author has used tragal cartilage as a compound graft in reconstruction of the ear canal wall when performing obliteration of old radical cavities (Tos 1977, Siim and Tos 1987), but in some cases the author has reconstructed the ear canal with tragal cartilage in order to ventilate the cavity in the following way: A tragal cartilage of maximum size is harvested, and the perichondrium is elevated from the concave meatal side, so that perichondrium is still connected to both edges of the tragal cartilage (Fig. 827). This perichondrium fixes the tragal cartilage to the meatal side of the remaining ear canal wall and cavity wall. Perichondrial flaps are similarly elevated, from the outer aspect of the tragus, and are used to fix the cartilage inferiorly onto the mastoid side of the facial ridge and to the cavity wall (Figs. 827, 828). After the tragal cartilage has been placed between the facial ridge and the anterosuperior wall of the cavity, and after perichondrial flaps have been placed and adapted onto the meatal sides of the ear canal, the perichondrium fixes the tragal cartilage to the mastoid side of the facial ridge (Fig. 829). Fascia covers the drum perforation and the entire ear canal wall. The epithelial flaps are replaced (Fig. 830), and the upper edge of the tragal cartilage is further secured by placing a small Palva flap into the cavity (Fig. 831).
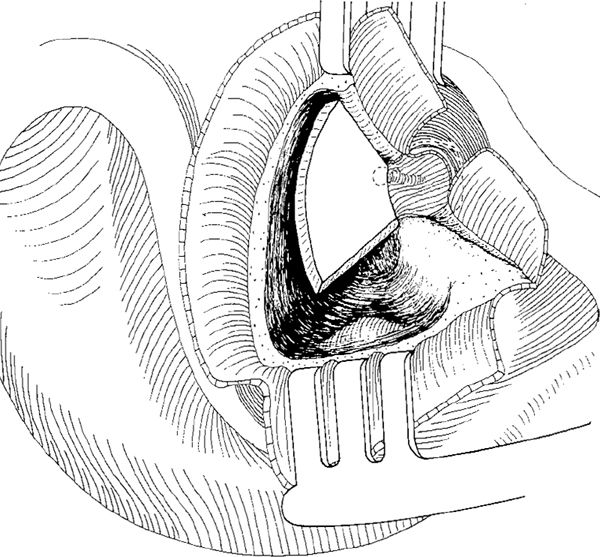
Fig. 825 A compound graft of tragal cartilage is placed at the side of the ear canal. The perichondrium, attached to the edge of the cartilage, covers the total perforation as an underlay graft
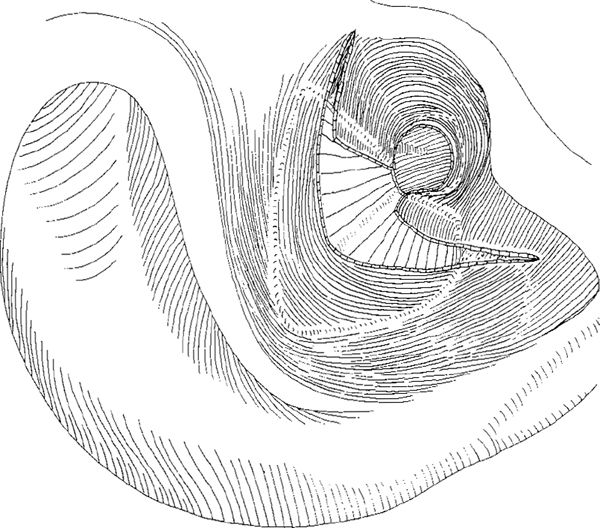
Fig. 826 The epithelial flaps are replaced, securing the position of the tragal cartilage
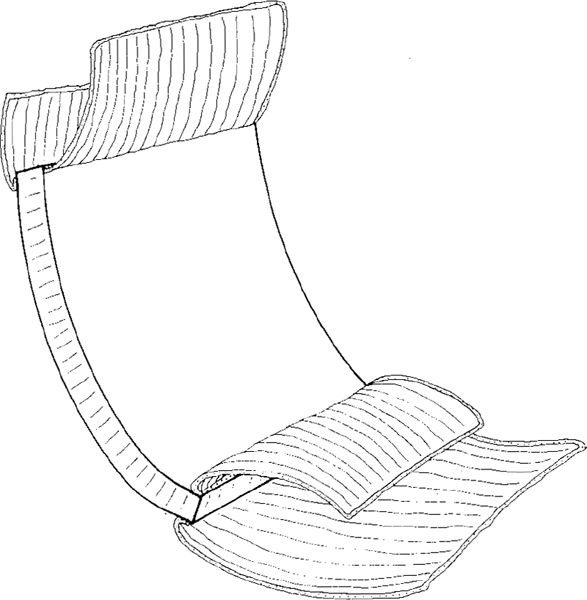
Fig. 827 Retroauricular reconstruction of the ear canal wall with a compound tragal cartilage–perichondrium graft (Tos 1977). The elevated perichondrium from the concave side of the cartilage is placed on the meatal aspects of the bone. On the convex side, a large perichondrium flap is elevated and placed on the mastoid aspect at the facial ridge. Superiorly, a small flap of the perichondrium is also elevated
In the present author’s opinion, this method of reconstructing the ear canal wall using autogenous cartilage, Palva flap, and fascia (Fig. 831) is an important element of several obliteration techniques, and can be applied to cover all allogenous material, even autogenous bone.
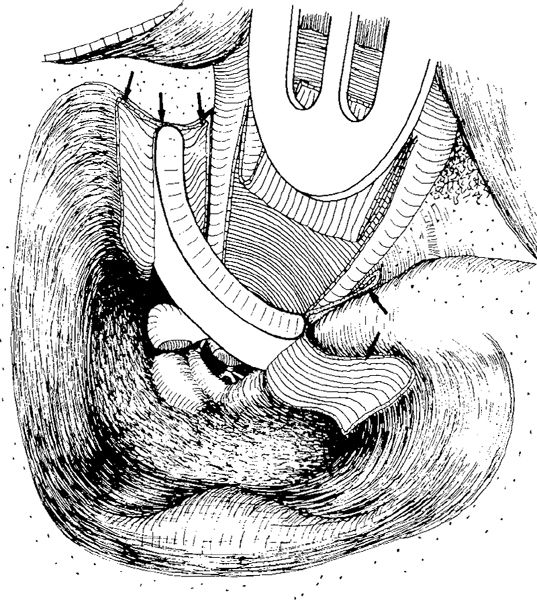
Fig. 828 The tragal cartilage–perichondrium compound graft in position. The cartilage is in contact with the superior wall of the cavity, and is fixed to it by the perichondrium flaps (arrows). Interiorly, the cartilage has some contact with the facial ridge, and is fixed to its meatal and mastoid sides with the perichondrium flaps (arrows)
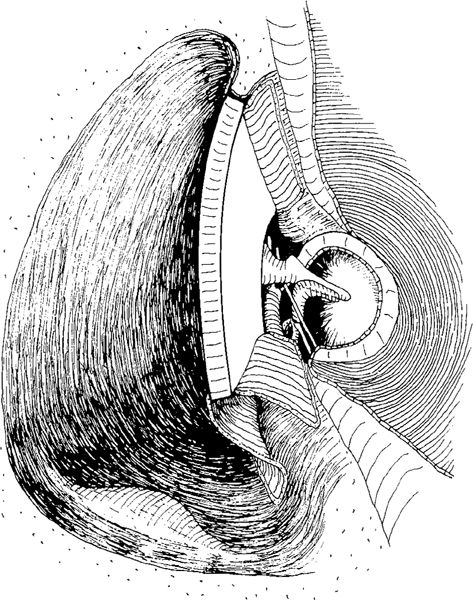
Fig. 829 The cartilage–perichondrium compound graft in position. The perichondrium flaps lie on the meatal side of the ear canal wall superiorly, and on the facial ridge inferiorly. An incus is placed on the stapes and along the malleus handle
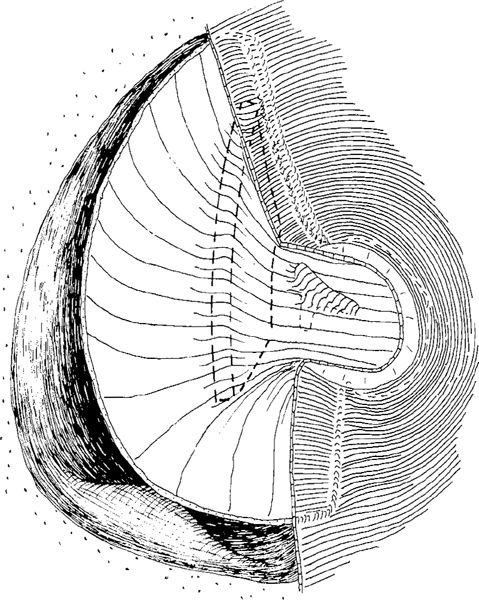
Fig. 830 The new ear canal wall is covered with a large piece of fascia, placed as an underlay graft under the drum remnant, and the epithelial skin flaps are replaced
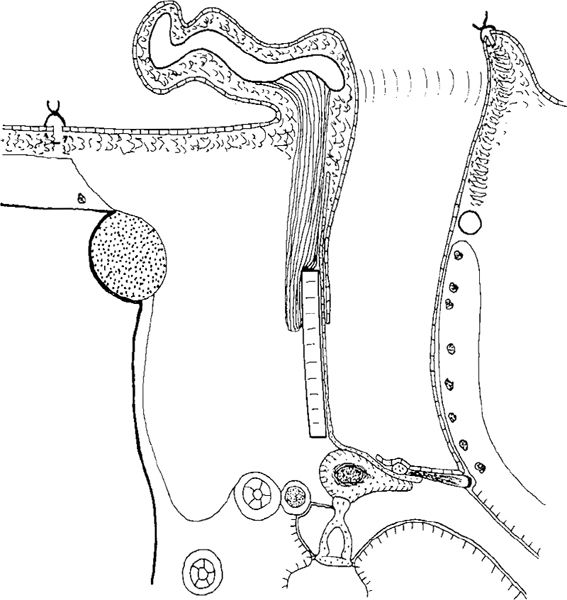
Fig. 831 Side view of the present author’s reconstruction of the ear canal. The tragal cartilage lies behind the fascia and anterior to the Palva flap
Reconstruction with Allogenous Cartilage
Reconstruction of the ear canal wall is also performed using allogenous septal or knee cartilage.
Septal Cartilage
Smyth and Dowe (1971) introduced allogenous septal cartilage as a method of reconstructing the ear canal wall in order to ventilate the cavity. An appropriately sized piece of allogenous septal cartilage, preserved in 70% alcohol for two to six weeks, is cut and shaped to fit exactly into the defect of the bony ear canal wall. This can be done most easily, and without wasting valuable cartilage, by first making a template from a piece of sterile metal foil such as that used in suture material packing. Once the cartilage is shaped, it then needs to be worked so that it adapts to form a curve matching the contour of the normal ear canal wail. This can be achieved by thinning and cross-hatching. The cartilage is then inserted into slots already cut into the superior cavity wall, along the zygomatic root and inferiorly along the facial ridge. The slots are made with a 2-mm diamond burr. The superior slot starts at the junction of the attic wall with the anterior meatal wall, and passes laterally. The inferior slot starts just lateral to the facial nerve, and continues along the facial ridge (Fig. 832). After ossiculoplasty and closure of the drum perforation with an underlay fascia graft, the previously trimmed septal cartilage is placed into the slots in such a way that it remains concave towards the meatus in the same way as the normal ear canal (Fig. 833). Sufficient communication between the tympanic cavity and the mastoid cavity — the artificial aditus — must be secured. Smyth lined the space with a thin silastic sheet in order to maintain its patency.
The fascia covers the perforation as well as the meatal surface of the septum. The lateral third of the cartilage can be covered with a small Palva flap, so that a situation similar to that illustrated in Figure 831, can be achieved, using tragal cartilage.
Of 10 cases operated on, the cartilage was displaced posteriorly into the cavity in two cases when a lateral periosteum–subcutis flap had not been used. A fistula developed through the septum in one case, and this was closed secondarily. In the remainder of the cases, the shape of the new ear canal appeared to have been maintained to a large degree at follow-up 2–2½ years after surgery.
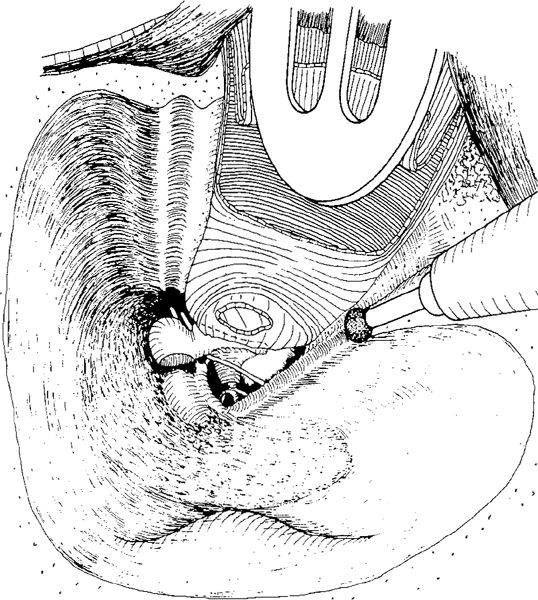
Fig. 832 Ear canal wall reconstruction with allogenous septal cartilage (Smyth and Dowe). After a canal wall–down mastoidectomy with removal of the bridge, a posterior perforation and interposition of a piece of cortical bone between the stapes and the malleus is performed. A groove is drilled with a 2-mm burr along the zygomatic root. A similar groove is drilled along the facial ridge
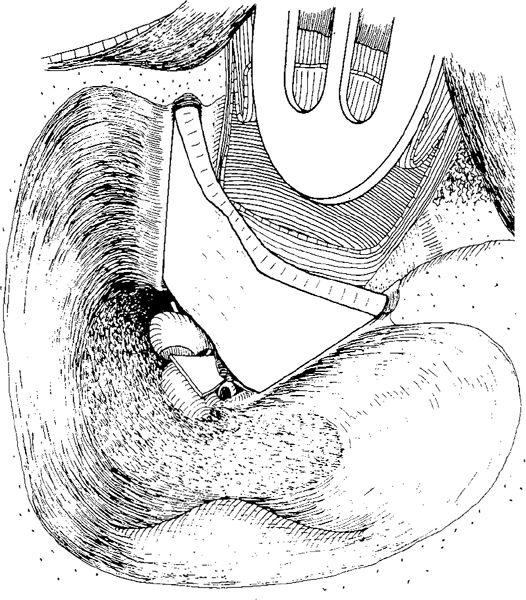
Fig. 833 The septal cartilage is trimmed to the exact size and shape, of the ear canal wall and placed in the grooves. The cartilage will be covered on the meatal side with the fascia. On the mastoid side, a Palva flap will cover the lateral part of the cartilage. A new tympanic isthmus is secured with a piece of thin Silastic
Pappas et al. (1981) used septal cartilage in the reconstruction of the ear canal and in scutumplasty. They advocate incision of the cartilage with several parallel-placed V-notched incisions through two-thirds of its thickness on the convex side, in order to increase its flexibility so that the cartilage will adapt to the curvature of the defect, as illustrated in Chapter 6 (Figs. 360–361).
Strauss (1974) used exactly the same technique as Smyth and Dowe, with superior and inferior grooves and a large septal cartilage graft, stored in Cialit (otimerate sedium). He performed small incisions on the mastoid aspect of the cartilage in order to achieve convexity. Using a Palva flap on the mastoid aspect of the cartilage and a large piece of fascia on the meatal aspect, the septal cartilage was extruded in only 5% out of 40 operated ears. In two patients, fistulas were found at the junction between the septal cartilage and the skin, and this could be avoided by using a Palva flap behind the septal cartilage.
Information is needed on the late results of ear canal reconstructions using allogenous septal cartilage.
Knee Cartilage
Wehrs (1972, 1978) used allogenous knee cartilage together with allogenous tympanic membrane with the malleus. The advantage of homograft knee cartilage should be its natural, concave shape and thin lower edge. The thin lower edge exactly matches the shape of the bony annulus in previous radical canal wall–down operations. Wehrs cuts grooves along the superior cavity wall and along the facial ridge, similar to the method illustrated previously for septal cartilage (Fig. 832). Additionally, he shapes the knee cartilage in a special way, creating a thin strip of cartilage to overlap the meatal sides of the facial ridge and the zygomatic root (Fig. 834). Using a thin foil template, the defect in the posterior ear canal wall is evaluated as to size and shape. The template is then trimmed so that it overlaps the facial ridge and dural plate, but does not block the mastoid antrum. Using this template, a block is cut from a selected specimen, and this block is then grooved at each end, so that a thin sheet of the cartilage will overlap the meatal plate and the facial ridge, to prevent formation of retraction, while the thicker posterior sheet is supported by the bony grooves (Fig. 834). The tympanic cavity is then reconstructed with allogenous tympanic membrane and attached malleus, and the ossiculoplasty is performed. The drum is placed on the annulus, and fascia is used to cover the entire allogenous drum and the septal cartilage (Fig. 835).
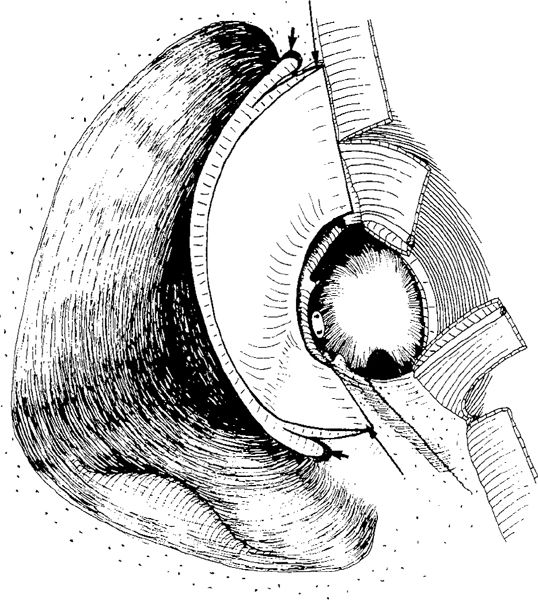
Fig. 834 Ear canal wall reconstruction with allogenous knee cartilage and allogenous drum (Wehrs) In a case with total perforation and no ossicles, grooves are created along the superior wall of the cavity and along the facial ridge (short arrows). The knee cartilage is trimmed in such a way that the thin slice covers the meatal side of the ear canal wall anteriorly, and the facial ridge inferiorly (long arrows). The thicker part of the cartilage fits into the grooves. Ear canal skin flaps are elaborated
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


