(1)
Department of Ophthalmology, St. Thomas’ Hospital, London, UK
3.1 Gases
3.1.1 Principles
3.1.2 Complications
3.2 Silicone Oil
3.2.1 Properties
3.2.4 Silicone Oil Removal
3.2.5 Heavy Silicone Oils
3.2.6 Heavy Liquids
3.2.7 ‘Light’ Heavy Liquids
3.3 Summary
Abstract
(also see Appendix: Useful formulae and rules)
3.1 Gases
3.1.1 Principles
(Also see Appendix: Useful formulae and rules)
It is important to understand Fick’s diffusion equation; that is, that two gases on either side of a semipermeable membrane will pass across the semipermeable membrane until their concentrations are equal on both sides. If one gas travels across the membrane at a slower speed than the other, then this causes a difference in size of the gas bubbles on either side of the membrane. For example, if a large molecule gas like sulphahexafluoride (SF6) is placed within the eye, this passes slowly into the blood stream, to the lungs and out into the atmosphere. However, nitrogen from the atmosphere is highly soluble and passes rapidly through the lungs, blood and into the eye causing the SF6 gas bubble to enlarge within the eye. For this reason, after a vitrectomy, SF6 and perfluoropropane (C3F8) must be mixed with air to prevent a volumetric increase, which would then cause a rise in intraocular pressure.
Additional surgical steps:
1.
Attach the air pump tubing to the three-way tap on the infusion line and switch on the air pump at 30–40 mmHg.
2.
With a flat retina, place the tip of a flute cannula close to the optic nerve head to drain the vitreous cavity fluid.
3.
Turn the three-way tap to allow insertion of the filtered air.
4.
Fill the cavity.
5.
Close one sclerotomy.
6.
Prepare the long-acting gas (mixed to the desired concentration with filtered air) by inserting into a 50-ml syringe (make sure any tubing for drawing up gas is flushed through with the gas before drawing up onto the syringe). Draw up the gas; for 30 % gas, you need 15 ml of gas followed by 35 ml of air to give a total of 50 ml (you may need more in a high myope; use two syringes). You can usually see how much gas was inserted by holding up the syringe to the light. Look for a condensation line where the syringe stopper was drawn up to with the long-acting gas, for example, a line at 15 ml. Mistakes can occur with gas mixtures with resultant underfill with too little long-acting gas or severe IOP rise with too much. Therefore, it is worth being careful and observing the processes during gas mixing to ensure the correct dosages are used. Use a 100 ml syringe to avoid conversion of ml to percentage, ie 30 mls = 30%.
7.
Attach the syringe to the three-way tap, and flush out the air by inserting 35 ml. Keep 15 ml in case of hypotony during closure of the surgical wounds.
8.
At the end of the operation, the air in the vitreous cavity must be flushed with a volume of gas to achieve the correct gas concentration.
9.
Close the second sclerotomy.
10.
With 23 g, remove both upper trochars and insert a 26-g needle through the pars plana to allow exhaust of the gases, attach the 50-ml syringe onto the three-way tap and flush through the gas to 15 ml.
Break closure can be achieved by the use of an internal tamponade such as a gas bubble. This acts in two ways:
1.
By ‘tamponading’ the break (the gas is in contact with the edge of the break) so that an accumulation of fluid is not possible through the break. The RPE pumps out the SRF flattening the retina. This is utilised in pneumatic retinopexy where SRF is not drained by the surgeon, and the retina is allowed to flatten spontaneously after intravitreal gas injection.
2.
By forcing the retina flat by displacing the retina outwards (except where aqueous persists, e.g. inferiorly). This is primarily reserved for an eye, which has had a vitrectomy, and the retina has already been flattened.
Note: Pneumatic retinopexy, that is, insertion of gas without vitrectomy, has a success rate of approximately 70 % which is lower than conventional or vitrectomy surgery (Zaidi et al. 2006; Yanyali et al. 2007; Lowe et al. 1988; Kulkarni et al. 2007; Hilton et al. 1987). However, it may reduce the need for more extensive surgery if one can accept the relatively low success rates and risk of PVR. In pneumatic retinopexy, rotation of the eye over a number of hours whilst the gas bubble is present may also be used to try to flatten the retina.
A gas bubble must have its effect for at least 5 days because the retinopexy requires time to take effect. For this reason, larger molecule gases are used so that dissipation of the gas bubble from the eye is retarded. The most popular gases are sulphahexafluoride (SF6) and perfluoropropane (C3F8) (Chang et al. 1984, 1985; Lincoff et al. 1983).

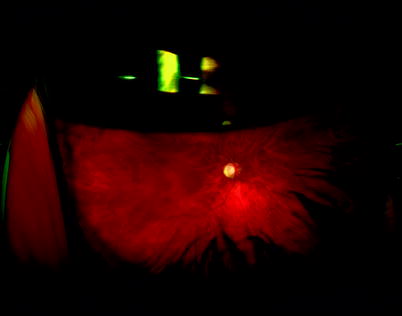
Fig. 3.1
When inserting gas through the three-way tap, make sure the tap is closed to the air infusion line; otherwise, the gas will enter the air infusion line and you will not achieve a full flush out of the air
Fig. 3.2
A wide angle view of an intraocular gas bubble; notice the flattened inferior surface of the gas bubble. The gravitational effect of the dense vitreous liquid relative to the less dense gas overcomes the surface tension (which tries to create a spherical gas bubble) thereby distorting the bubble and flattening the inferior surface
Fig. 3.3
As the gas bubble gets smaller, the inferior surface becomes more curved; when the bubble is very small, it will be spherical
Note: If the retina is completely flat (no SRF), then tamponade is not necessary to close the break, and retinopexy is enough. This is exploited when treating a flat retinal break in the clinic (the retina around the break remains flat despite the need for a few days for the retinopexy to reach full adhesion) presumably because the retinopexy confers some mild adhesion immediately. This has been exploited by Martinez-Vasquez (Martinez-Castillo et al. 2007) who has described vitrectomy with aqueous tamponade for pseudophakic RRD. This method requires fastidious removal of all of the SRF during the PPV (the SRF is squeezed out by the use of heavy liquid posteriorly and air anteriorly, with the air removed again at the end of the operation) and heavy diode laser retinopexy. As a proof of principle, the method is of interest, but most surgeons would leave the air inside the eye and tamponade as usual. However, the principle is exploited in RRD with inferior holes where contact of a gas bubble cannot be guaranteed, and the surgeon, with complete removal of SRF, can leave the inferior holes treated with retinopexy and no indentation; see later chapters (Tanner et al. 2001; Martinez-Castillo et al. 2005).
Properties
100 % SF6 doubles its volume in 2 days and is present for 2 weeks (Lincoff et al. 1984). Its non-expansible concentration is between 20 and 30 % with air.
C3F8 expands four times at 100 % concentration, lasts 8 weeks and has a non-expansible concentration with air of 12–16 %.
With experience, the concentration most appropriate to the surgeon can be decided upon. 30 % SF6 and 16 % C3F8 may be suitable to start with.
The gases have a high surface tension of 70 mN/m, that is, the gas remains as one sphere and does not break up into smaller bubbles. This stops the gas bubble from going through the retinal break, allowing contact with the edge of large breaks without the gas entering the subretinal space.
Problems with gas bubbles can be determined from the Fick’s diffusion equation, for example, during surgery with injection of gas; nitrous dioxide from the anaesthetic will rapidly enter the gas-filled eye. This means that postoperatively, the gas bubble will shrink as the lungs exhale this nitrous dioxide. In practice, this may not have a major effect on the size of the gas bubble, but most surgeons prefer to switch off nitrous dioxide when using gases during surgery. A patient with gas in situ should not have a general anaesthetic using nitrous dioxide because this will enter the gas bubble and cause expansion and a severe rise in IOP potentially resulting in central retinal artery occlusion (Hart et al. 2002).
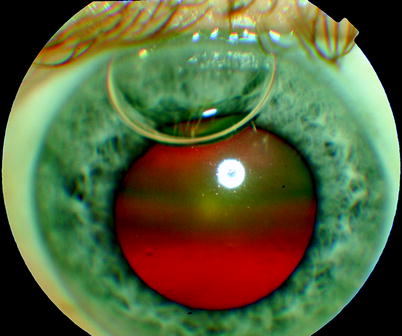
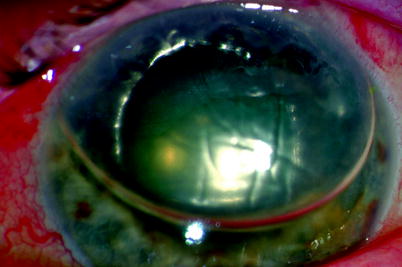
Fig. 3.4
Air can enter the anterior chamber at the end of the operation as in this eye in which there is presumably a defect in the zonule. Attempting to remove the AC gas by aspiration and infusion of fluid can result in a reduced gas fill in the posterior segment because the infusion fluid enters the vitreous cavity (passing with gravity around the lens) and the gas escapes through the sclerotomies. Therefore, it is best to have the sclerotomies closed. Any gas leakage must then occur through the anterior segment and can be monitored by the surgeon. If the gas bubble is not removed, the bubble will be present in the postoperative period usually without any consequences and with gradual absorption
Fig. 3.5
A large air bubble which has leaked into the anterior chamber has caused pupil block
The inferior border of a gas bubble has a flattened meniscus. Therefore, it is not possible to know reliably that the gas bubble will tamponade detached inferior breaks. For this reason, surgeons often apply a plombage between the 4 and 8 o’clock positions. However, in a vitrectomised situation, this may give a risk of choroidal haemorrhaging because of hypotony, indentation of the choroid and suturing near vortex veins. It is, therefore, sometimes advisable to rely on strict posturing of the patient to tamponade an inferior break. In this circumstance, the patient with an equatorial or pre-equatorial break which is inferiorly placed is postured face up. This may increase the risk of cataract but reliably closes inferior breaks. If an inferior plombage is desired, insert heavy liquids into the eye before placement of the explant. This will limit the size and spread of any haemorrhage should it occur.
A Safe Method for Drawing Up Gas
Most gases are provided in disposable canisters, and the assistant fills a 50-ml syringe with the correct percentage of gas and air. Errors can occur, and if the wrong gas is inserted for flushing at the end of surgery, there can be catastrophic visual loss from central retinal artery occlusion. Allowing the assistant to draw up the gas and air has led to 100 % gas fills and CRAO from severe IOP rise in the early postoperative period.
Follow this method to minimise the risk of error:
1.
The assistant draws the correct amount of gas into the syringe, for example,
8 ml for a 16 % gas fill in air
15 ml for a 30 % gas fill in air
2.
The assistant hands the syringe to the surgeon who draws in the air to make up the volume to 50 ml. Alternatively use a 100ml syringe to avoid the need to convert mls to percentage.
By splitting the responsibility for drawing up the gas by the assistant and the air by the surgeon, it is very difficult to create an error of 100 % gas (the surgeon would not have any space to draw up air if the assistant hands over 50 ml of gas). Both must check the type of gas used. The surgeon can double check if the correct gas volume has been drawn up by observing a tell tale condensation mark, for example, at the 8 ml mark. The only risk of error is that the assistant incorrectly draws up air rather than the long-acting gas (or the wrong number of mls of gas). This will lead to a gas bubble duration which is too short, a problem which can be overcome by reoperation or strict posturing. This is preferable to an erroneous 100 % long-acting gas and subsequent IOP rise and central retinal artery occlusion.
3.1.2 Complications
Vision
Postoperatively, the patient with a gas bubble will notice that they have blurred vision from refractive changes in the eye. As it resolves, a dark line (the inferior edge of the bubble) passes horizontally from superiorly to inferiorly, the bubble gets smaller and more spherical, and gradually multiple small bubbles appear and shortly after complete dissipation of the bubble. Once the bubble edge passes above the visual axis (the dark line is now below the patient’s central vision), the patient will start to see more clearly.
Fig. 3.6
A patient’s drawing of visual phenomena around the gas bubble showed diffraction of light and an alteration of colour in the centre of the bubble
Refraction
The phakic or pseudophakic patient is made myopic by the gas bubble and can often see more clearly close to the eye and looking down. The aphakic patient is made even more hypermetropic.
Fig. 3.7
The refraction of the gas-filled phakic or pseudophakic eye is increased because the effective power of the posterior surface of the lens is increased (the difference in the refractive index of air and the lens is greater than the difference between water/vitreous and the lens), causing a large myopic shift. In an aphakic eye, the convexity of the gas bubble in the pupil effectively creates a negative refractive change causing a large hypermetropic shift
Cataract
The gas itself may cause a feathery posterior subcapsular cataract or ‘gas cataract’ which is temporary (clears once the gas absorbs) but associated with an increased risk of nuclear sclerotic cataract later on.
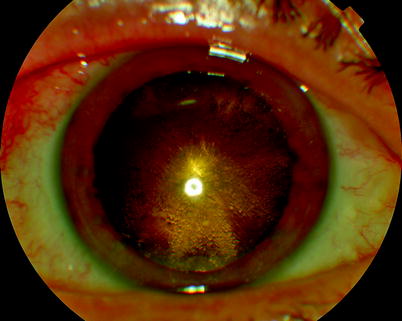
Fig. 3.8
A typical feathery cataract from gas insertion. This will clear but results in an increased chance or early onset nuclear sclerotic cataract formation
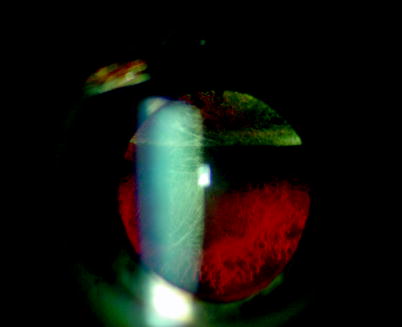
Fig. 3.9
In some patients, gas in the vitreous cavity causes a feathery and bubbly posterior subcapsular cataract in the early postoperative period, for example, 2 weeks. This clears once the gas absorbs but usually leads to early onset nuclear sclerosis

Fig. 3.10
Gas in the anterior chamber postoperatively has led to the formation of an anterior capsular opacity
IOP
Raised intraocular pressure may occur after gas expansion in the early stages but can usually be treated medically.
Severe IOP elevation suggests an error in the composition of the gas during mixing with air at surgery, that is, the gas is at too high a concentration and is expanding causing an IOP rise. Some gas may need to be removed, but there is a risk of choroidal haemorrhage during this manoeuvre if the IOP cannot be brought down medically before the gas removal.
What to do: Attach a needle to the air pump, increase the pressure to the patient’s IOP level, insert the needle into the eye and gradually reduce the air pump pressure to allow a controlled reduction in IOP. Then you can proceed to PPV and exchange of the gas for the correct concentration. This will require gas fluid exchange and fluid air exchange (if you still need the tamponade agent, the pathology may now have resolved, e.g. check if the macular hole is closed) followed by flushing with the correct gas concentration as described above.
Fig. 3.11
An anterior ischaemic optic neuropathy possibly from IOP rise after PPV showing thinning of the nerve fibre layer superiorly on OCT scan
Loss of the Gas Bubble
Gas dissipates early, or the bubble size is too small if the concentration inserted has been too low. This risks failure of the surgery because of reduced tamponade area.
1.
What to do: Some of the error can be compensated for by asking the patient to posture so that the gas bubble contacts the area of pathology, for example, face-down posturing for a macular hole. Occasionally, the gas bubble will need to be replaced by repeat operation.
Gas may vent through an open sclerotomy if the pressure rises significantly leading to underfill.
Gas in the Wrong Place
If the infusion cannula is unstable during surgery, it may angle forwards risking gas insertion through the zonules of the lens and into the anterior chamber. If the hole in the zonules is large, gas may represent through the hole even after removal of the gas from the AC. This can make visualisation of the retina difficult in which case the gas may be displaced by viscoelastic. Removal of the viscoelastic may allow the gas back into the AC. In most circumstances, gas in the AC postoperatively can be allowed to dissipate without problems (the flattened inferior meniscus allows the aqueous to flow without causing pupil block). Occasionally, pupil block glaucoma will occur, which can be temporarily alleviated by YAG peripheral iridectomy and medication until the gas is absorbed.
Gas in the suprachoroidal or subretinal spaces is very rare. Again movement of the infusion cannula especially in patients with anterior contraction of the vitreous base (as in PVR) or with detachment into the pars plana may allow air to infuse under the retina. To leave gas in postoperatively will cause recurrent retinal detachment with PVR.
1.
What to do: The gas can be removed via retinotomy or via a retinal break or choroidectomy. Alternatively, a fine gauge needle can be inserted transconjunctivally and through the scleral (whilst observing the eye internally) to contact the bubble and allow egress.
Table 3.1
Common gases used during pars plana vitrectomy
Gas | Structure | Molecular weight | Expansion of 100 % concentration | Duration (days) | Non-expanding concentration (%) | Uses |
|---|---|---|---|---|---|---|
Air | 29 | 0 | 5–7 | NA | Flat retinal breaks | |
Sulphur hexafluoride (SF6) |  | 146 | 2 | 14 | 20 | Superior retinal breaks (above 4–8 o’clock) |
Perfluoroethane (C2F6) |  | 138 | 3 | 30 | 16 | Macular hole surgery |
Perfluoropropane (C3F8) |  | 188 | 4 | 60 | 14 | Multiple holes |
Inferior breaks | ||||||
Macular holes | ||||||
Early PVR | ||||||
Diabetic TRD |
Table 3.2
Complications from gas insertion
Complications of gas insertion | Abnormality | Frequency |
|---|---|---|
Cataract and lens | Gas cataract | Occasional |
Nuclear sclerosis | Very common | |
Posterior subcapsular cataract | Rare | |
Displacement of an intraocular lens implant (especially sulcus fixated lenses or anterior chamber lenses) | Occasional | |
Glaucoma | Temporary from gas expansion | Common |
Angle closure from gas in the anterior chamber | Very rare | |
Gas errors | Wrong gas | Very rare |
Wrong concentration | Very rare | |
Underfill | Rare | |
Refraction | Myopic shift whilst gas is in situ | Always |
Gas in the wrong place | Subconjunctival gas from wound leakage | Very rare |
Anterior chamber gas from leakage through a zonule dehiscence or capsulotomy | Rare | |
Visual field loss | Probably from drying of the retinal surface peroperatively; by closing the sclerotomies (valves or plugs) the flow of air over the retina is minimised | Rare |

Fig. 3.12
This gas bubble is pushing the IOL forwards at the superior edge which can entrap the edge of the iris. Wait till the gas bubble has gone, and then divide the inevitable posterior synaechiae from the anterior capsule by passing a cannula between the capsule and the iris, free up the iris margin and relocate the IOL edge behind it
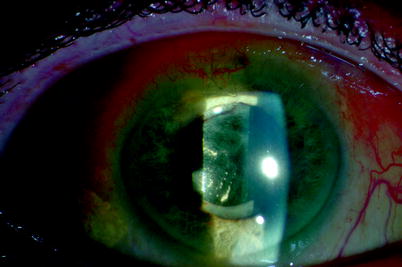
Fig. 3.13
In some patients with combined PPV, gas and cataract extraction, the IOL may be tilted by the gas bubble. The edge of the IOL may move anteriorly to the edge of the pupil causing ‘capture’ of the pupil margin and adhesion of the iris to the lens capsule. This is associated with rapid posterior capsule opacification. Once the gas bubble has reabsorbed, the pupil should be surgically released from the capsule and replaced in its correct position in front of the IOL. A surgical capsulectomy can be performed with a vitrectomy cutter on low cut rate (200 bpm) introduced through pars plana
3.1.3 Important Postoperative Information
Flying or Travel to High Altitude
The patient should avoid flying whilst the gas bubble is in situ as the drop in cabin pressure causes increased IOP because the bubble tries to expand (Lincoff et al. 1989a, b) resulting in pain and a risk of central retinal artery occlusion. Subsequently, after the eye has adjusted to the raised IOP during the descent of the aircraft, the eye becomes hypotonous with a risk of intraocular haemorrhage. Similarly, the patient should not change altitude (e.g. driving across a high mountain pass) because the variations in atmospheric pressure will increase or decrease the bubble size.
Flying or travelling to high altitude causes a drop in atmospheric pressure which would normally be accompanied by an increase in the volume of the gas bubble (Aronowitz and Brubaker 1976). Within the confines of the eye, this expansion cannot occur without loss of aqueous from the eye. If the aqueous cannot be removed, the IOP elevates; see the table. As aqueous leaves the eye, the IOP will gradually fall; some eyes, for example, glaucomatous eyes with poor aqueous outflow facility, will struggle to reduce their aqueous volume to compensate for the increase in volume required.
The absolute pressure in the eye is atmospheric pressure (760 mmHg) and IOP combined therefore.
At sea level | 776 mmHg (760 + 16 mmHg) |
At 2,400 m altitude | 576 mmHg (560 + 16 mmHg) |
Table 3.3
Pressure changes in a normal-sized eye during air travel and cabin depressurisation (sea level to the equivalent pressure of 2,400 m altitude). Therefore, any volume around 0.50 ml (one-eighth full) or more in a normal-sized eye risks producing an IOP which can occlude ocular circulation
Gas volume (ml) | IOP rise (mmHg) from a baseline of 16 mmHg | Duration to achieve IOP rise (min) |
|---|---|---|
0.125 | 26 | 10 |
0.25 | 43 | 10 |
0.5 | 70 | 10 |
1.0 | 105 | 10 |
2.0 | 120 | 8 |
4.0 | 140 | 8 |
It is possible to calculate how much the gas bubble must expand to allow the IOP to normalise:


P1 = 776 mmHg, that is, atmospheric pressure plus 16 mmHg and P2 = 576 mmHg, atmospheric pressure at 2,400 m plus 16 mmHg after the bubble has expanded to allow the IOP to drop to 16 mmHg.


Therefore, the bubble must expand to about 1.35 times its initial volume for the pressure to drop back to normal, that is, the eye will need to lose aqueous to allow the expansion.
How long this will take will depend on the initial gas bubble volume and the rate of aqueous outflow, assuming no wound leak.
Larger volumes will prevent the IOP ever returning to normal; for example, a 3.0-ml bubble cannot expand to 1.35 times its initial volume in a 4-ml eye however much aqueous escapes.
Note: It is the difference in pressure between atmospheric pressure and absolute eye pressure (measured as IOP) which affects the ocular circulation because measured systemic blood pressure is similarly the difference between atmospheric pressure and the pressure in the blood vessel.
General Anaesthesia
General anaesthesia should be only performed with the anaesthetist aware of the gas within the eye to allow the avoidance of expansion of the bubble with the anaesthetic gases particularly nitrous dioxide. Patients have lost all vision from central retinal artery occlusion in this circumstance (Hart et al. 2002; Fu et al. 2002; Mostafa et al. 1991). Some surgeons provide a wristband to be worn by the patient warning about gas in the eye and to alter any general anaesthesia agents used.
3.2 Silicone Oil
Additional Surgical Steps
Method 1 (has the advantage that the retina can be manipulated during the oil insertion):
1.
Attach a silicone oil-filled syringe linked to the silicone oil pump set to 50 psi to the three-way tap. Reduce the pressure to 30 psi with 23 gauges to avoid separation of tubing from the infusion trochar.
2.
Insert a flute needle and drain intraocular fluids (SRF, then vitreous cavity fluids and then heavy liquids) whilst actively inserting the oil.
3.
Drain fluid off the disc.
4.
Leave the IOP at approximately 10 mmHg.
Method 2 (has the advantage of inserting the oil onto the macula first allowing egress of SRF through anterior retinal breaks and may reduce the risk of subretinal oil):
1.
Fill the eye with air.
2.
Insert the oil through a sclerotomy allowing the air to egress from another sclerotomy.
3.
Leave the IOP approximately at 10 mmHg.
Silicone oil is used when more permanent tamponade is required, for example, for retinal breaks with residual traction from proliferative vitreoretinopathy (PVR), or in trauma. It has a Si–O–Si polymer structure. Two types are in use, 1,000–1,300 and 5,000–5,900 mPas. There are theoretical advantages for the use of the latter for permanent tamponade or to avoid emulsification of the oil, for example, in young patients; however, the former is easier to handle surgically because of its lower viscosity. 1,000–1,300 mPas is recommended in most circumstances. In my experience, there appears to be little advantage in using 5,000 mPas oil (Scott et al. 2005).
Surgical Pearl of Wisdom
There is a simple explanation of why a direct oil/PFCL exchange is less likely to cause slippage, and it is as follows:
When oil is injected and once it makes contact with PFCL, the two liquids join together to make a single bubble. The reason is that both oil and PFCL are hydrophobic and they prefer to be in contact with one another and thus exclude water from the interface. This single bubble at the beginning is in fact a heavy bubble. Any aqueous is therefore displaced superiorly and laterally towards the sclerotomy.
Slippage is the posterior displacement of aqueous under the retina by an incoming bubble (usually air). It results in retinal folds and leaves large area of bare RPE to promote PVR.
The tip I wish to offer is to fill the vitreous cavity as full as possible with PFCL when dealing with giant retinal tear or giant retinotomy after adequate relief of traction. As the oil is injected, pass the draining flute needle through the oil and dip into the PFCL. This way, the two liquids will be forced to make contact. Once they touch, the aqueous will automatically be displaced laterally and superiorly (Li and Wong 2008).
Try it.
Professor David Wong, Dept of Ophthalmology, University of Hong Kong, Hong Kong, China
3.2.1 Properties
1.
Viscosity, 1,000–1,300 or 5,000–5,900 mPas
2.
Molecular weight 25,000 or 50,000
3.
Refractive index 1.4
4.
Density 0.97 g/cm3
5.
Surface tension 21.3 mN/m
6.
Interfacial tension in water 40 mN/m
Silicone oil is clear, inert and floats in aqueous, and is highly stable in the eye (Lakits et al. 1999). It has a flotation force, but its density is only slightly less than water, so the bubble is dominated by its interfacial tension. Therefore, it has a spherical configuration within the eye. Using the principle of ‘a sphere within a sphere’, its contact with the retina is less extensive than a gas bubble (see Appendix). Oil may sometimes be used in complex retinal detachments without PVR when there are multiple breaks requiring multiple retinopexy applications or very large breaks such as giant retinal tears. The risk of missing a small break in such a situation, for example, when 10 or 12 breaks are present, means that using gas could result in early return of the retinal detachment and the onset of PVR. The latter occurs because of the recent operation and the release of cytokines and growth factors from the increased use of retinopexy. A tamponade of silicone oil will prevent retinal redetachment until removal of the oil, thereby allowing the inflammatory mediators in the postoperative period to subside. Thereafter, oil removal may reveal a return of the retinal detachment, but this will be hopefully detected early (or even during the oil out operation; see ROSO plus) and localised to the area of the retinal break and will not have other influences increasing the risk of PVR. Of course, in this situation, there is a risk that the complications of silicone oil may ensue. However, its short-term use in this situation should avoid most of these.




