Chapter 2 Principles of Allergy Management
Core Concepts
In a strict sense, allergic load refers to the cumulative, clinically relevant, antigenic exposure affecting the patient at any one moment in time. Allergic load as a concept is important as it may directly influence the allergic response, both early and late phase inflammation, and expression of symptoms. Controlling allergic load therefore becomes an important tool in overall allergy management. Quantitative antigen exposure may vary from one point in time to another. For example, seasonal pollen counts may vary from one year to another and from day to day during any one year’s season. In addition, they are usually higher in the morning than in the evening, and will be reduced depending upon rainfall during the day. Dust mite exposure varies from time spent indoors versus outdoors, in humid versus arid climates, and as a function of elevation above sea level. Becoming familiar with the nature of antigens and antigen classes is essential in understanding and applying the concept of allergic load. This working knowledge directs history taking, the direction of diagnostic testing, and the formulation of a management action plan.
In addition to the importance of the allergic load, the concept of nasal priming further implies that the cumulative, clinically relevant antigenic exposure required to provoke symptoms tends to lessen as the patient is repeatedly challenged by antigen. From a basic immunologic standpoint, antigen-specific naïve lymphocytes may be primed when an antigen is presented to them in an immunogenic form (e.g., antigen incorporated in a presenting cell) which results in a differentiation into armed effector cells or memory cells capable of a second or subsequent immune response.1,2 Quantitatively, continued subsequent antigen exposures require less and less antigen to produce the response. Wachs et al describe nasal priming as “increased clinical response to daily nasal challenges.”3
Nasal priming is not antigen specific.4 Skoner et al discuss possible mechanisms for increased tissue responsiveness after antigen stimulation,5–10 and suggest how the priming effect and continued exposure to allergens would lead to prolonged and chronic inflammation with the promotion of chronic symptoms and comorbid conditions. With their work on Eustachian tube dysfunction, antigen exposure, and nasal priming, Skoner et al showed how inflammation continued for a period of time, up to weeks after cessation of pollen exposure, and theorized how this inflammation could possibly promote chronic Eustachian tube dysfunction and middle ear disease.4,5,11 In addition, only 23% of allergic rhinitic patients have pure seasonal rhinitis; 77% of allergic rhinitics, therefore, have perennial rhinitis, with or without seasonal flaring. Thus, seasonal antigens may add to chronic inflammation that already exists due to perennial antigenic exposure, which further amplifies the association with chronic, comorbid conditions such as middle ear disease, rhinosinusitis, and/or asthma.
While nasal priming was at one time thought to be specific only for antigenic triggering,12–14 other authors indicate this is not the case, for example citing histamine as a trigger of the phenomenon.5,15 Allergic and nonallergic triggering is therefore another essential concept in comprehending the additive nature of rhinitic and/or other respiratory inflammation. In assessing the history, seldom does the patient with allergic rhinitis solely have allergic triggers, and in some patients the rhinitis will be purely nonallergic. Vasomotor or idiopathic triggers may include, but are not limited to, temperature change (especially cold), exercise, barometric pressure change, gustatory stimulation, and chemical or irritant exposure. Infectious insults also augment inflammation in several ways. For example, allergic factors are suspected in the pathogenesis and expression of recurrent acute rhinosinusitis and acute exacerbations of chronic rhinosinusitis, which are often triggered by a viral respiratory infection. In addition to the direct inflammatory response to the viral particles, the allergic individual will reactively produce larger amounts of immunoglobulin during the acute illness. This effect is additive. Viral illness in the allergic individual versus the nonallergic tends to be more symptomatic, more morbid, and more likely to require an antibiotic and extended care for secondary bacterial sequellae. In addition, while Samter’s triad or aspirin (ASA) triad patients (nasal polyposis, asthma, and ASA and/or NSAID (nonsteroidal anti-inflammatory drugs) sensitivity) will usually not have allergic factors, a number of nasal polyp patients (including allergic fungal sinusitis (AFS) patients) may have concurrent allergic rhinitis. Previous studies lead the clinician to believe allergic management in these patients helps control the overall rhinitic impact, and improves the control of the hyperplastic membrane disease, approaching a level of control experienced with the nonallergic polyp patient. Other chronic diseases may trigger nonallergic rhinitis in the allergic patient, such as sarcoidosis, inflammatory bowel disease, granulomatous disease, and the neurogenic (trigeminal nerve/inferior salivary nucleus) mediated nasal congestion/lacrimation of some migraine/vascular headaches. Medication side effects may add to rhinitis symptoms. The Physicians’ Desk Reference cross-references side effects of sinusitis and rhinitis for 300 and 400 drugs respectively.16–18 In addition, nasal symptoms may have noninflammatory factors as well. For example, obstructive rhinitis or rhinosinusitis may have fixed mechanical component(s) such as a deviated nasal septum, paradoxical middle turbinate, concha bullosa, or some other anatomical form of adynamic obstruction. These adynamic factors act in concert with the more dynamic (mainly inflammatory) factors in producing the additive result of obstruction and other symptoms. In a more abstract sense, other medical comorbidities such as poorly controlled diabetes and immune deficiency, can amplify rhinitis symptoms.
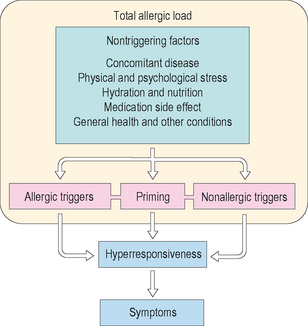
Given the preceding discussion, some conclusions are suggested. In the broadest and most clinically relevant sense, the definition of allergic load now becomes the sum total of all environmentally and medically related factors which may impact the expression of allergic rhinitis and its sequellae in a given patient at any one point in time (Figure 2.1). Reducing the allergic load as a treatment modality therefore goes beyond the environmental control (EC) of allergens. It includes avoiding or controlling respiratory irritants and other vasomotor factors, managing respiratory infections, identifying and treating comorbid medical problems and other chronic inflammatory diseases, lessening medication side effects, and utilizing indicated airway operative procedures. An example in summary: the asthmatic allergic rhinitic with chronic rhinosinusitis, who smokes, has poorly controlled diabetes, and is on a beta blocker for poorly controlled migraine headache masquerading as a sinus headache, has a number of factors to deal with for optimum rhinitic outcome and quality of life.
Lastly, a discussion of the lower respiratory tract is necessary. Current models of allergic respiratory disease regard the respiratory tract not as divided upper and lower components, but as one unified system, responding in a homogeneous fashion to inflammation. The early conceptual work involved studies of allergic response. About 35% of patients with allergic rhinitis will develop asthma at some time in their life. Up to 95% of asthmatics have chronic rhinitis. Diagnosing asthma goes beyond bronchial hyperreactivity. There has to be an associated, reversible, obstructive functional change. That being said, most allergic rhinitics will demonstrate increased bronchial hyperreactivity during times of increased rhinitis and will be subject to priming and all of the conceptual nuances discussed thus far.5 As such with this unified airway concept in mind, the inflammatory problems of the respiratory tract to be examined in the bulk of the remaining chapters are rhinitis, rhinosinusitis, otitis, conjunctivitis, laryngitis, and asthma. With all of the previous comments noted, the last core concept to be discussed is the classification of antigens.
▪ Classification of Antigens
Inhalant allergens are categorized by phylogeny and to some extent by the times during the year in which the patient is exposed, i.e., perennial or seasonal (Box 2.1). The pollens are a broad group consisting of grasses, trees, and weeds. These antigens tend to be clinically significant on a seasonal basis. In temperate climates, grass pollination generally begins in the spring and extends into the summer. Tree pollination begins in the late winter, accelerates in the spring and declines in the summer. The weeds may begin in mid summer, accelerate in late summer and early fall, and decline in mid fall. Variations may occur on the basis of temperature, rainfall, and other environmental factors. For example a dry, cold, late winter–early spring, may delay pollen emergence or suppress quantity. However, in warmer climates, such as the southern USA, grass may pollinate almost on a perennial basis, or perhaps have two distinct seasons within a year’s time. For such locale-related inconsistencies in antigen description and other reasons, there is a current movement to describe allergic disease in terms of its chronicity as being intermittent versus persistent and its severity as being either mild, moderate, or severe. This description parallels current systems used in describing asthma. It is clear that clinicians need to be familiar with the antigens in their locale. Given the different routes of exposure through which allergens stimulate the patient, it is common to classify allergens by phylogeny and structure (e.g., pollens, dust components, fungi or molds, animal epithelials, insects, foods, venoms/drugs, and contactants). Some characteristics of these antigen classes will be discussed next. Additional characteristics will be presented in the section on environmental control (EC) and will be discussed then.
Plant Antigens (Pollen)
Pollen is the male germinal element of plant flora emitted during the reproductive phase. Such plants can be pollinated by the wind, known as anemophilous, or by insect transfer of heavier, stickier pollen, known as entomophilous. Most clinically significant pollens (mainly anemophilous) share certain characteristics that promote their clinical antigenicity, and are said to satisfy the elements of Thommen’s postulates listed in Box 2.2. Even though entomophilous plants do not produce light, buoyant, windborne pollen, some may still be clinically significant if the patient handles the pollen from the plant, or with a massive, direct exposure. Of the thousands of continental anemophilous plants, only a little over 100 appear to be clinically prominent. Due to climate, natural selection, and human management of the environment, numerous pollen and mold zones exist around the world. Up-to-date zonal pollen and mold information is available through the Internet, the printed literature, and through antigen extract and allergy testing device vendors. While university extension divisions can also be queried in narrowing the number of pollinating plant species of antigenic and clinical importance, this approach may be of limited utility. Box 2.3 demonstrates a collection of suggested antigens, including pollens by family that can be used for objective testing and screening purposes. Antigenic plants are generally classified as trees, grasses, or weeds.
BOX 2.2 Thommen’s postulates
The plant must be seed bearing, with pollen windborne
The pollen must be produced in large quantities
The pollen must be buoyant to be widely transported
The plant must be abundantly distributed, preferably close to human habitation
Trees
Tree pollination usually occurs most vigorously in the spring but varies according to latitude, longitude, and climatic influences. The seasons for each of the tree species tend to be short and well defined compared with the grasses. There may be cross-reactivity between closely related trees (genus), but as a rule, trees do not cross-react widely among different families. Therefore, antigen selection for testing and treatment may include a number of trees within the clinician’s area or other nonindigenous trees brought into the patient’s environment. Diameter of tree pollen is usually up to 40 μm. Trees are divided into two main groups, the larger flowering trees (angiosperms), and the cone-bearing trees (gymnosperms). Box 2.4 lists members of both of these classes with examples for each. Some of the members, marked in bold, may have implications as food sensitizers.
Grasses
Grass pollen is very potent, perhaps the most potent sensitizer among plant antigens. Only the fall weeds, specifically the ragweeds, sensitize more allergy patients seasonally. Of the thousands of grass species and their five major subfamilies of antigenic interest listed in Box 2.5, the three of most clinical significance are noted in bold with examples. There is a great deal of cross-reactivity within the subfamilies. As such, and with the high degree of potency and sensitizing capability, the number of grasses tested and treated should be limited to one member of each subfamily of importance within the patient’s environment. Testing and treating with multiple grasses in a more extensive fashion increases the risk of adverse reaction. The grass pollination season generally begins in the spring and continues into the summer. Seasons will vary depending upon latitude and climate. Shorter and better defined seasons may be found in temperate climates, as opposed to longer seasons for some species in warmer subtropical and tropical climates.
Weeds
The fall weed season has often been described using the term “hayfever” for the seasonal allergic rhinitis occurring at this time of year. Weeds usually pollinate in late summer into fall, but like the grasses, these seasons vary. They may overlap with grass, mold, and some tree seasons. Where prevalent, the ragweeds are the most significant pollen sensitizers. In most climates, the six families of most allergenic interest are listed in Box 2.6 with subfamilies and examples. There is some degree of cross-reactivity within subfamilies, thus there should be some economy in antigen selection for testing and treatment. In some cases, such as with the ragweeds, an extract of a ragweed mixture may be used. Some of the subfamily members are not readily windborne and are of lesser clinical importance. One such example cited is goldenrod. Minor weed subfamilies need to be considered, as there may be certain patients who will be exposed and sensitized to them.
Animal Antigens
Mammalian and avian antigens
Products of mammals and birds are also antigenic and may include epithelials such as feathers, hair, dander, pelt, saliva, or urine. In addition, even mold growing in aged feces can be antigenic. By far, cat seems to be the most significant sensitizer, of which dried saliva is of primary importance. In the atopic child, early exposure to mammalian antigen, especially cat, along with prematurity and exposure to wood burning appliances or cigarette smoke has been linked with the early emergence of allergic disease including asthma. Cat antigen is so ubiquitous in the environment and is such a potent allergen that it should always be screened for even if the patient does not come in known direct contact with the animal. This testing is especially important if the patient has reactive airways disease. Dog antigen may also be important, and antigenicity may vary from breed to breed. In some parts of the world, dog also may be a food allergen as well as inhalant allergen. When examining animal allergy, the patient history must extend beyond cat and dog. A thorough assessment of both the patient’s home and work environments is important, since patients in agriculture and laboratory settings may come into contact with mammalian species other than cat and dog.
Fungi – Yeast and Molds
The fungi may be antigenically important as inhalants, ingestants, or contactants. While fungi include yeasts and molds, they are referred to in this section globally as molds. Mold allergies may be perennial or seasonal, indoor or outdoor. In theory, molds may elicit a Gell-Coombs I (allergic) or IV (delayed) response. In the central USA, for example, mold activity is perennial outdoors, especially if the winter is warm. There are seasonal flares in the spring, with the return of warmer and rainy conditions; in mid to late summer with increased humidity and heat; and in the moderate warmth of fall, with the decay of foliage and the priming of the weed season. Indoors, mold is promoted by dampness, warmth, darkness, and any moist, organic material used as a source of nutrients. Although many tens of thousands of species are known, less than 100 are of allergenic significance. Clinically important molds are noted in Box 2.7. Four of the most common mold species found indoor/outdoor are Alternaria, Penicillium, Aspergillus, and Cladosporium. In addition, mold families that are clinically important in allergic fungal sinusitis (AFS) may differ from those involved in rhinitis. Box 2.8 demonstrates a list of molds often reported in cases of AFS. There is little cross-reactivity between mold families. The major molds in any one locale will be important in the evaluation of not only rhinitis, but also asthma. Buoyant mold spores, measuring up to 20 μm, are a common form of inhalant mold exposure, in addition to mycelial forms and yeasts, which may be contactants and/or ingestants as well. Mold spores may be transported over long distances by the wind, and are of higher concentration in the cool of the evening and during warm windy weather after precipitation. While 8–12 molds are often sufficient for testing, in the highly mold sensitive patient, the difficult to diagnose patient, or the patient who is not doing well under treatment due to a suspected unidentified mold, a more expanded mold test battery may be indicated. At times, it has been worthwhile setting out mold spore collection plates obtained from some extract vendors to identify the prevalent species in the difficult patient’s environment.
Ingestants
Fixed Food Allergy
Although virtually any protein with antigenic potential could cause an allergic reaction if ingested by a susceptible individual, ingestant allergy problems are usually foods or drugs. Only about 20–30% of adverse food reactions are felt to be IgE-mediated, and therefore allergic. The term adverse food reaction is inclusive of hypersensitivity reactions and the nonimmune food intolerance. To the patient, the two groups are undistinguishable. Most people feel that any food-related reaction is “allergic.” The hypersensitivity group, commonly called allergic, contains the true IgE-mediated reactions and other immune-related reactions which may or may not include an IgE participation. The overall incidence of food allergy has been estimated to be up to 8% in children and up to 2% in adults. The majority of documented food offenders in children include egg, peanut, soybean, fish, wheat, tree nuts, and milk. In adults the majority list would include tree nuts, peanut, fish, and shellfish. Members of food families often cross-react within specific families. True IgE-mediated clinical manifestations of food allergy would include urticaria and/or angioedema, respiratory symptoms including rhinosinusitis, laryngitis, Eustachian tube dysfunction, asthma, and conjunctival/scleral symptoms. Other IgE manifestations may include anaphylaxis, oral allergy syndrome (discussed later), atopic dermatitis, and eosinophilic GI disease. Patients with atopic dermatitis (eczema) may have IgE-mediated food sensitivities in an estimated 30–40% of cases. Only a portion of the eosinophilic GI patient’s symptoms may have IgE-mediated factors. Other suspected immune hypersensitivities include a few enteropathies and inflammatory bowel conditions described elsewhere. Food intolerance may include metabolic, toxic, or even functional/psychological conditions of nonhypersensitivity natures.19
Nonfixed food allergy
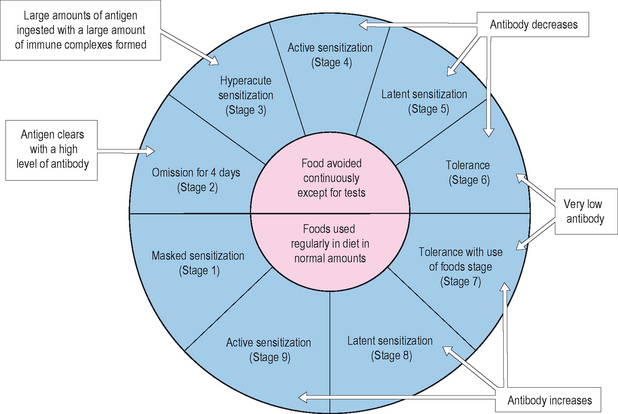
Food allergy may be rarely fixed, but is more commonly acquired in nature. Acquired food allergy is demonstrated in a susceptible individual, who begins to develop symptoms after repeated ingestion of a food. A current model for describing the conduct of this phenomenon is the cyclic nature of food allergy (Figure 2.2). In this model, after introduction and sensitization to the food, the patient begins to have symptoms with further ingestion of the food. If the ingestions are separated by intervals of time of several days or more, the symptoms may be easily identified with the ingestion. If the ingestions are very frequent, say daily, the symptoms may be more muted, diffuse and systemic, and more difficult to associate with the ingestion. Through elimination of the offending food, symptoms eventually improve/resolve, and in a period of months, the patient may become tolerant to the ingestion of the food. Tolerance may be maintained with infrequent ingestions, whereas the patient may cycle back to symptomatic expression if the interval of ingestion becomes more frequent. Fixed food allergy is always symptomatic and not affected by periods of abstinence from the food. Symptoms for peanut, seafood, and tree nuts generally do not improve with cessation and time.
Positive epicutaneous skin testing for food is often inaccurate, although negative epicutaneous tests may have better predictive ability. There is some controversy over the efficacy of in vitro methods for food testing, with IgG food testing only relevant for ingestion, not hypersensitivity. When feasible, any possible food allergen, identified by history or positive in vivo or in vitro test, should have its clinical significance determined by elimination over a period of 1–2 weeks resulting in improvement of symptoms, or the elimination for 5–7 days and the demonstration of symptoms with reintroduction over a 2-day period. Suspected fixed food allergies should not be challenged, and strict avoidance of those foods should be recommended. The other option, and the gold standard, for cyclic food allergy is the use of the double-blinded, placebo-controlled food challenge. This challenge also requires an elimination of the food to be tested for 1–2 weeks before the challenge.19
Drug Allergies
Most patient-reported “allergic reactions” to drugs are not allergic in nature. The range of real and perceived adverse reactions involving drugs is rather wide. Drug side effects, drug–drug interactions, dose related symptoms, and the like are not allergic in nature. Macy et al use the example of the non-IgE-mediated angioedema seen with ACE inhibitors as an idiosyncratic response.20 True IgE-mediated reactions involve an antigenic protein or hapten coupling to trigger the response. A common example of a true allergic reaction is that of penicillin sensitivity in which a penicillin metabolite couples with a protein to form a hapten which is immunogenic.20 Drugs may be involved in several Gell-Coombs types of reactions. Intravenous radiologic contrast sensitivity is an example of an anaphylactoid type response, i.e., a direct, nonallergic effect on mast cell release. IgE-mediated reactions have also been reported for a variety of hormonal proteins such as insulin. Skin testing, when prudent and possible, is still used to help with making a diagnosis. Unfortunately specific antigenic testing materials for drug testing are often not readily available. For example, not all of the determinants to be tested in penicillin allergy are made by commercial vendors. Cephalosporin minor determinant antigens are also not available for skin testing. In vitro testing is nonexistent or at best, limited. While avoidance of IgE-mediated drug allergens is the treatment of choice, there are times when graded challenges, provocation testing, and desensitization may be indicated for diagnosis and/or therapy.20 Lastly, drug reactions on occasion may be the subject of reactions to nonactive ingredients in the drug other than the active, named drug. These ingredients can include chemical additives or foods. Drug allergy is discussed in detail in Chapter 10.
Injectants
Allergic reaction by injection of allergenic material usually falls within the realm of drug allergy. Patient histories on occasion have indicated that oral ingestion of an allergen may not produce the reaction experienced with the injection of the drug. This observation is of limited clinical interest, since any true allergy to a drug by one route of exposure mandates avoidance of the use of that drug. Once again, some injectables have other nonactive ingredients which may be the provoking agent. Other injecting allergens may be via the puncture or sting of plants or animals. Reactions may be local, self-limited irritating responses, or delayed, more widespread immune responses, or an overwhelming systemic, IgE-mediated anaphylaxis. Allergic reactions to the stinging order of Hymenoptera (vespids and bees) are perhaps most important, followed by reactions to the fire ant. Distinction has to be made between a local reaction at the sting site versus a true allergic, more systemic or anaphylactic reaction. Desensitization in many cases is possible and indicated.21 Insect allergy is discussed in detail in Chapter 9.
Contactants
Boguniewicz and Beltrani22 estimate there are 85000 chemicals which will cause an irritant type of reaction to the skin upon contact. These irritant responses are nonimmunologic, usually cytotoxic. Approximately 2800 of these chemicals are capable of a delayed, Gell-Coombs type IV response, the mechanism of allergic contact dermatitis (ACD). Photocontact dermatitis is similar to ACD except that ultraviolet light is needed as part of the triggering mechanism. Irritants may include soaps and other cleaning agents, petroleum products, paint and printing chemicals, adhesives and synthetic resins, hair products, landscaping and pest control chemicals, building and insulating materials, and common allergens such as dust, plants, foods, and insects. Contact allergens include plants such as poison ivy or ragweed, metals such as nickel, plastic resins, organic dyes, preservatives, topical medications such as neomycin, and rubber chemicals including latex. These agents are often tested with patch testing, which is discussed later in this chapter. Identification and avoidance is the treatment of choice, augmented with topical and systemic medication.22
Cross-reactivity
Cross-reactivity between antigens occurs when an antibody directed against one specific antigen is successful in binding with another, different antigen. The two antigens in question have similar three-dimensional structural regions, known as epitopes, which allow the antibody for one antigen to recognize a second antigen as being structurally the same antigen. Cross-reactivity may be robust among antigens of similar phylogeny such as different types of oak trees or ragweeds. Seemingly different antigens within families may substantially cross-react, such as with timothy and rye grass, or there may be a weaker cross-reactivity, such as with timothy and Johnson grass. Foods may also cross-react with other foods such as within the families of grains. Foods may cross-react with inhalants as in the oral allergy syndrome described later. Other associations described have included ragweed and some melons or bananas for example.23 Patients may be more symptomatic during ragweed season when consuming cantaloupe, adding to their critical allergic load. This last example has been called concomitant food sensitivity. Latex represents an example of a collage of antigens to which some latex-sensitive individuals have reported a significant incidence of concomitant food sensitivity. Food cross-reactivities are not well understood and there has been a recent change in their emphasis. Knowledge of cross-reactivity allows for better management of allergic load, and the use of fewer antigens in objective testing and immunotherapy.
Testing Methods
▪ In Vivo Techniques
Skin testing is the primary technique used for the diagnosis of inhalant allergy. For at least 135 years physicians have been testing patients for specific antigen using the skin. Blackley described a first test, the precursor to the scratch test, for fall pollen in 1873.24 Noon and Cooke were among the early clinicians to use skin testing for immunotherapy.25,26 By the 1920s the scratch test, skin prick test (SPT), and fixed concentration intradermal test (FIT) were being used. Hansel described a 1 to 10 dilutional method of intradermal testing which was the precursor to skin (serial) endpoint titration (SET), a 1 to 5 quantitative, dilutional method described by Rinkel in the 1950s.27–30 More recently, hybrids of SPT and SET, mainly the modified quantitative test (MQT), have been introduced to improve patient and physician cost as well as patient convenience, while keeping the level of quality commensurate with SET.30 Because of the adaptation of intradermal testing beyond the methodology of SET, intradermal dilutional testing (IDT) is now the appropriate term for the use of varied but sequential dilutions of antigen concentrations in intradermal testing methods. Skin testing may be epicutaneous or intradermal. Epicutaneous tests include the scratch test, and the prick/puncture tests, for which physicians may use either single or multiple prick/puncture testing devices. Intradermal tests utilize either fixed concentration (FIT), or sequential concentration dilutions (IDT) for testing. These tests may be used in screening for allergy or in an expanded battery for a more comprehensive evaluation.
Scratch Testing
The scratch test, as its name implies, involves scratching the superficial, keratin layer of the skin with a sharp instrument. This scratch may be performed through a drop of concentrated antigen extract placed on the skin, or the antigen may be applied to the area after the scratch. The site is observed for 10–20 minutes and the wheal and flare of any reaction is subjectively graded. The results are compared with positive and negative controls. The positive control is usually histamine, and the negative control is usually saline or diluent. For a test to be considered truly positive, the skin must be reactive to a positive control, usually histamine. Unfortunately there is frequently a high incidence of false positive results with scratch testing. The trauma of the scratch on occasion can stimulate a histamine-related axonal reflex, resulting in an axonal driven wheal and flare at nearby test sites (false positives). In addition, there is a significant occurrence of insufficient antigen penetrating the subkeratin layer to elicit a positive response in a truly allergic patient (false negative).31–33 Thus, the scratch test has been considered unreliable in the diagnosis of allergy by the American Medical Association Council on Scientific Affairs due to its lack of sensitivity (false negatives) and specificity (false positives).34 This safe but unreliable qualitative test, once widely performed, is not in common use today.
Prick/Puncture Test
SPT may be performed in one of two ways. The “drop and puncture” method involves applying antigen extract to the skin first and then puncturing the skin through the droplet.31,33,35 The volar surface of the forearm is usually chosen as the site for the test, although the upper arm and the back can also be used for testing. With the SPT being performed initially on the arm, management or adverse systemic reactions may be facilitated by using a tourniquet on the arm above the site of the test. Therefore, the SPT is usually performed on the forearm and the FIT on the upper arm or back. The antigen used is usually a standardized concentrate or a nonstandardized concentrate of 1 : 10 or 1 : 20 w/v. The positive and negative controls are histamine and a diluent such as buffered, phenolated saline respectively. After alcohol cleansing and drying the volar surface of the forearm, areas at least 2 cm apart are marked. This distance between test sites will potentially avoid vigorous wheal and flare responses from running into each other as well as making an axonal response less likely. A drop of a different specific antigen, determined by the history, is placed at each mark. Using one of several single puncture devices available, the skin is punctured through the droplet to a superficial level without producing a show of blood (Figure 2.3). The device is discarded. As recommended by OSHA, the puncture and wipe technique should not be currently used because of the bodily fluid/pathogen contamination risk to the technician and the possibility of cross-contamination of antigens. There are numerous single puncture instruments to choose from. Some of these include: the Duotip-Test® and Duotip-Test®II (Lincoln Diagnostics, Decatur, IL), Sharp-Test™ (Panatrex, Inc., Placentia, CA), Morrow Brown® (Alkaline Corp., Oakhurst, NJ), Quintip® (Hollister-Steir Labs, Spokane, WA), GreerPick™ System (Greer Laboratories, Inc., Lenoir, NC), and AccuSet™ (ALK-Abelló, Round Rock, TX).

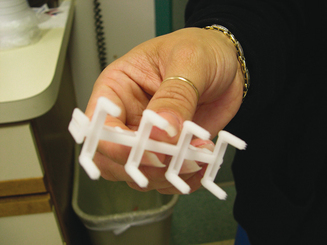
The “dip and puncture” method allows test site preparation in the same fashion as above.31,33,35 After marking the arm, the puncture device tip is dipped into a well with the concentrate of the specific antigen to be tested, and then the “loaded” device is applied to the test site. As with single prick testing, there are several multiple puncture devices available to apply more than one antigen simultaneously. Some of these devices and their manufacturers are: Multi-Test and Multi-Test®II (Lincoln Diagnostics, Decatur, IL), Quick-Test (Pantarex, Inc., Placentia, CA), Quin-Test® (Hollister-Steir, Spokane, WA), and Skintestor Omni™ (Greer Laboratories, Inc., Lenoir, NC). As an example, the Multi-Test®II device has two rows of four puncture heads in parallel (Figure 2.4). The plastic points of each head are 1.9 mm in length and hold the antigen after placement, until it is deposited into the epithelial/superficial dermal layers of the skin, for a total of eight tests per application. The firm but gentle pressure of the application, followed by a gentle rolling motion delivers a test comparable to a superficial intradermal test. Multiple puncture devices are safe, reproducible, and reliable, and may be used effectively as a screening test modality.31,36,37 Multiple puncture devices deliver more tests per unit time, and are cost-effective and well tolerated by patients.
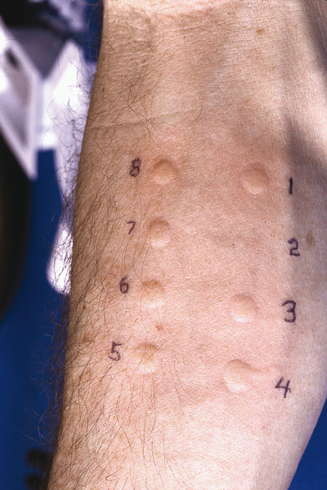
Interpretation of SPT can utilize a subjective grading system or can involve precise measurement of wheal size. Tests are usually read in 15–20 minutes and area compared to positive and negative controls (Figure 2.5). Pseudopodia and irregular spreading are noted. Wheal sizes of 3 mm or greater than a negative control are generally considered positive. In another approach, SPT results can be given a score of 0 to 4+ based on size, amount of erythema, and presence of pseudopodia. While SPT testing is becoming more uniform, the scoring systems are still varied.31,33,35
A nuance in testing is the use of SPT in the evaluation of oral allergy syndrome (OAS). The technique has been called the prick + prick method, an attempt to use fresh, unprocessed antigen in the epicutaneous test format. Pastorello has described OAS as a complex of signs and symptoms exclusively involving the oral and pharyngeal mucosa subsequent to contact with a specific food.38–41 The foods involved are usually either a fresh fruit, nut, or fresh vegetable. There is almost always an association with an inhalant, most commonly a pollen. The presentation may be as minor as tingling in the mouth or as threatening as laryngopharyngeal edema with airway obstruction. The suspected relationship is a cross-reactivity between the food and the pollen. When the food is ingested, often during the pollen season, the syndrome is triggered.42 As an example, OAS has been demonstrated with silver birch and hazelnut.43
In evaluating this syndrome from an objective testing standpoint, there are problems with false negatives for both in vivo and in vitro techniques. It is suspected that there is a degree of physical lability of the functional immunogenic makeup of the antigens involved which makes detection difficult.44 For testing purposes, antigenic material has to be processed in some way. Antigens are processed to be made into allergenic extracts and they are processed to be attached to a substrate for an in vitro test. Even the food used for the double-blind, placebo-controlled food challenge has to be lyophilized, and there is a problem as well with gastric acid altering the processed food antigen(s).43,45 It is suspected that during the processing, the antigenic nature of the epitopes involved is changed enough such that the testing results in cases of truly positive patients are inconsistent. As such, some in vitro and in vivo testing methods using fresh, unprocessed antigenic material have shown some promise.36,46,47 One attempt is a prick + prick method. As an example, a fresh fruit being tested is punctured by the pricking device which hopefully loads the device with workable antigenic material. Immediately the skin of the patient is then pricked with the loaded device. While results using this method have shown somewhat better correlation of history with objective testing, less than optimal sensitivity still makes testing for OAS problematic. OAS represents a form of concomitant sensitivity and has been referred to as clustering of hypersensitivity.48
Single-dilution (Fixed-dilution) Intradermal Test
Epicutaneous tests such as SPT are often utilized as screening tests for allergy. They may be used in a screening battery, and in the traditional sense of allergy testing, as a safe first step in the testing sequence. If the SPT is negative for a particular antigen, and the history suggests presence of allergy to that antigen, it may be indicated to perform an intracutaneous or intradermal skin test for diagnosis. Intradermal tests are generally more sensitive than epicutaneous tests. They also have a higher risk of adverse reactions. It is therefore essential to demonstrate the absence of severe reactivity with a negative SPT first, or to use a dilutional intradermal method such as IDT, or a blended test such as modified quantitative test (MQT). In performing FIT, the concentration is usually 1 : 100 to 1 : 1000 of that concentration used for the negative SPT. This test should not be used for food testing because of the incidence of false positives and the risk of a systemic reaction in a highly allergic patient.35 The test is performed by injecting just enough test antigen (usually 0.02 mL) under the superficial epithelial layer of the skin (intradermal) to raise a 1- to 3-mm skin wheal. This is done with a tuberculin syringe, bevel down, at an approximately 45 degree angle. The test is read and scored in a similar manner as with SPT.35 With the traditional sequencing of SPT and FIT, highly sensitive (+SPT) and relatively lower sensitive (−SPT, +FIT) patients may be detected.
If a patient is going to be treated with environmental control (EC) and symptomatic medication, there has been some controversy as to the utility and accuracy of the single-dilution intradermal test.31 The use of SPT and FIT for diagnosis and the institution of immunotherapy, however, has been successfully practiced by allergists for many years. One specific issue of concern is diagnostically overlooking the patient with very low sensitivity to the antigen being tested. This failure to diagnosis low-level allergy may be a factor leading to less than optimal results with diagnosis and immunotherapy since the risk of undertreatment is higher. This issue led to the development of dilutional techniques such as IDT and MQT.
Intradermal Dilutional Test
Intradermal dilutional testing (IDT) is a skin testing method using a series of 1 to 6 dilutions of a test antigen concentrate, applied in sequence from dilute to more concentrated, until an endpoint determining diagnostic reactivity is obtained. This method is both qualitative and quantitative. IDT has been approved by the AMA Council on Scientific Affairs for the diagnosis of allergy and, when indicated, the initiation of immunotherapy.34 This method is safe, and does not require a preceding epicutaneous test. Other benefits of IDT include an improvement and standardization of test interpretation, reproducibility and standardization of testing procedure, and due to its functioning as a quantitative bioassay, a method for allowing safety with variations in antigen sourcing and single antigen extracts. The following explains the method. The reader is referred to other references for even more extensive details and nuances which are beyond the volume of this chapter.31,32
Antigen preparation for IDT testing is important. Extract concentrates formulated by the vendor in the weight/volume (w/v) format should be 1 : 20 w/v or converted to 1 : 20 if supplied as 1 : 10 w/v by diluting 1 to 2 with a buffered, phenolated saline diluent (diluent). Antigens supplied as standardized extracts are usually considered conceptually as 1 : 20 dilutions, although local practices for individual antigens may differ. The panel of six dilutions for each specific antigen needed for the testing will be made starting with six, 5-mL, sterile injection stoppered bottles filled with 4 mL of diluent. One milliliter of the concentrate is then injected and mixed with the diluent filled bottle labeled #1 dilution. This now becomes a 1 to 5 dilution of the concentrate designated for mixing the testing dilutions. The #2 dilution is then mixed in a similar manner taking 1 mL of the #1 dilution and mixing it with the 4 mL of the next diluent filled bottle, labeled #2 dilution (1/25 of the concentrate). This process is repeated until the #6 dilution (1/312 500 of the concentrate) is made. It is rare that dilutions weaker than a #6 dilution will be needed for testing or mixing antigen for immunotherapy. Extracts from the vendor will have glycerin in them to preserve potency. Glycerin, as an irritant, can be a nonallergenic trigger for a whealing response and will need to be used as one of the three controls for the testing method. The glycerin control results will be taken into consideration when evaluating IDT results for the more concentrate dilutions (higher glycerin content from the concentrate). The other two controls will be histamine and the phenolated saline diluent. These controls will help rule out a suppressed reactive state (anergy or medication suppression [e.g., antihistamine, tricyclic antidepressant] = negative histamine control) or a hyperreactive state (e.g., dermatographia = positive histamine, glycerin, and diluent control). Rarely a patient will react to the phenol in the diluent in which case the diluent control will be positive.31 With six-bottle series of dilutions for each antigen, the clinician is ready to perform IDT.
The upper outer, hairless surface of the arm is prepped with alcohol and dried, then marked horizontally at the arm’s top, left to right, 6 to 1, with 2 cm between marks (helps prevent axonal responses). Then, vertically down, below and left of the #6 mark, the arm is labeled for the antigens to be tested, again 2 cm spaced. After the controls are placed and a response indicating the patient’s appropriate state for testing established (refer to reference 31), specific antigen testing begins with an array of intradermal tests for the #6 dilution of all of the different antigens to be tested. This amounts to a vertically placed row of tests below the #6 mark and to the right of the respective antigen labeling (Figure 2.6). The technique for placing the test is as described before, except enough antigen volume is drawn into the testing syringe to produce a 4-mm skin wheal. Since this usually requires an injected volume of about 0.02 mL of antigen, accomplishing the 4-mm wheal comes from trial and error experience rather than trying to allocate 0.02 mL by a measured injection. The tests are observed for 10–20 minutes, after which the diameter of the wheal is measured, neglecting the erythema which may accompany it. A negative whealing response will be 5 mm, starting with the 4-mm bleb at the time of the intradermal injection, which grows to 5 mm due to nonallergic factors. If an initial test at the #6 dilution is negative, another test using the #5 dilution is placed in the appropriate column, and so on, until all the dilutions are shown to be negative or until a positive response occurs. A positive response will be a wheal size greater than the 5 mm. A positive allergic response with a defined endpoint will be the demonstration of an increase in whealing response starting with a negative test, and progressing over the next two dilutions, increasing 2 mm in whealing size per dilution. For example, a whealing pattern for a specific antigen demonstrating an allergic response might be 5 mm for the #5 dilution, followed by 7 mm for the #4 dilution, and 9 mm for the #3 dilution. This is a positive testing sequence indicating allergy for that antigen where the endpoint is defined as the first reacting dilution in the 2 mm per dilution succession, i.e., the #4 dilution. The confirming dilution is the dilution producing the second, successive 2-mm gain in whealing size, i.e., the #3 dilution in the example. There is no reason to test past the confirming test. In fact, there is an increased risk of provoking symptoms or an adverse reaction. In an allergy battery, the endpoints for the different positively tested antigens are usually varied, thus giving results quantitated to that patient’s degree of sensitivities. Compared to traditional methods, these various endpoints then provide the basis for tailored immunotherapy, which allows starting doses of therapy to be safely more concentrated, theoretically producing improvement in symptoms within an earlier timeframe. Testing from one dilution to the next in sequence across the dilutions from weaker to stronger is called horizontal testing, which is safe but can be time consuming and labor intense. When the initial test for a specific antigen is negative (#6 dilution), it is permissible to jump two dilutions and place the #4 dilution on next. Depending upon a positive result, the third test may have to be one dilution up or down to try to confirm an endpoint. If the second test (#4 dilution) is negative, the skipping process, i.e., go to a #2 dilution, is permissible. This process, especially when the testing sequence for other allergens in the battery can be performed in this manner at the same time, is called vertical testing.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


