Chapter 9 Management of the Patient with Inner Ear Allergy
Introduction
It is likely that there is more to an “allergic” reaction involving the labyrinth than a classic type 1 hypersensitivity reaction. The pathogenesis of immune-mediated inner ear disorders is not known, although autoantibodies, autoreactive T cells, immune-complex deposition, and vasculitis have all been suggested.1 Autoimmune responses involving the inner ear range from the patient with Ménière’s disease who has a clear seasonal component to his or her symptoms, to the patient with a true organ-specific response characteristic of autoimmune inner ear disease (AIED).
The temporal relationship between ingestion of a suspect food and the later development of vertigo or hearing loss in an affected individual, as well as the well-documented evidence of increased circulating immune complexes in the serum of patients with Ménière’s disease, all hint strongly at a type 3 immune-complex-mediated hypersensitivity in some patients with this syndrome.2,3
However, we do not believe that all immune-mediated damage to the inner ear is “allergic,” but rather that there is truly a spectrum, including some who have an organ-specific autoimmune disease involving the labyrinth, which is best treated by steroids or, potentially, other immunosuppressive or immunomodulating medications.
Review of Immunology
The inner ear has little exposure to pathogens and few resident cells that are associated with immunologic function.4 While this led in the past to the assumption that it is immunologically privileged, in a manner similar to that of the brain, more recent research has indicated that inflammation can occur there, and that it is actually more immunoresponsive than the brain. Like the brain, the labyrinth also exhibits a blood–labyrinthine barrier, analogous to the blood–brain barrier, which helps to maintain the ionic characteristics that are unique to the cochlear environment. Also, in a manner similar to the brain, there is no lymphatic drainage from the inner ear. While immunoglobulins are present in the perilymph, the amount is only 1/1000 of that present in the serum.5
The inner ear demonstrates both cellular and humoral immunity. Most leukocytes enter the cochlea via the spiral modiolar vein.6 The innate immunity of the cochlea has been suggested to allow an adaptive local response to antigen challenge.7 Hashimoto et al have suggested that the inner ear may be “primed” by lipopolysaccharides or other viral/bacterial antigens, resulting in the upregulation of interleukin 1β in the fibrocytes of the spiral ligament, which in turn permits the entry of leukocytes. Subsequently, in those individuals having lymphocytes primed to react against inner-ear antigens, an immune response may be initiated, resulting in local inflammation and hearing loss.
Altermatt et al have suggested that the seat of immunoactivity in the inner ear appears to reside in the endolymphatic sac and duct.8 Immunoglobulins G, M, and A, as well as secretory component, are all found in the endolymphatic sac, and numerous plasma cells and macrophages are found in the perisaccular connective tissue.
As well as having an apparent innate immunity, the labyrinth has been found to have active components of allergic reactivity as well. Mast cells have been identified in the perisaccular connective tissue. Following sensitization, IgE-mediated degranulation of the mast cells has resulted in eosinophilic infiltration of the perisaccular connective tissue and the clinical production of endolymphatic hydrops.9
The endolymphatic sac has been shown to be capable of both processing antigen, as well as producing its own local antibody response.10,11 The surgical destruction of the endolymphatic sac or the obliteration of the endolymphatic duct results in a decrease in both antigen and antibody responses.11 The endolymphatic sac has a highly vascular subepithelial space containing numerous fenestrated blood vessels.12 Arterial branches of the posterior meningeal artery supply the endolymphatic sac and duct.13 While the labyrinth is similar to the rest of the central nervous system in being protected by this blood–labyrinthine barrier, the posterior meningeal artery is fenestrated, offering a peripheral portal of circulation. In other parts of the body, fenestrated vessels supplying organs involved in absorption (e.g., kidney, choroid) are especially susceptible to damage by immune complex deposition.
From this abbreviated background of otoimmunology, we shall now review some specific symptom complexes in the labyrinth that may be caused or influenced by an underlying allergic reaction (Box 9.1).
Ménière’s Disease
The senior author’s practice is composed largely of patients diagnosed with Ménière’s disease, whether felt to be related to allergy or not, and this chapter will largely deal with this syndrome. A suggestion that at least some cases of Ménière’s disease may have an allergic component is hardly a new idea. In fact, the first published report of Ménière’s disease felt to be provoked secondary to an allergic reaction was in 1923.14 Both inhalant and food allergies have been linked with symptoms of Ménière’s disease and cochlear hydrops.15 Changes in electronystagmography and electrocochleography recordings have been noted on patients injected with food extracts during provocative food testing.16,17 Additionally, Gibbs et al have reported the production of electrocochleographic changes in patients with known inhalant allergies and Ménière’s disease after nasal provocation by inhalant antigens.18
Many of the clinical characteristics of Ménière’s disease suggest an underlying inflammatory if not autoimmune etiology. Its notorious propensity to wax and wane, becoming active again after long periods of remission, suggests an inflammatory component. It is bilateral in a significant number of cases.19 A delayed Ménière’s-like picture may develop in a normal ear following trauma to the contralateral ear. It is often initially responsive to steroid treatment, although the senior author has noted a tendency towards steroid resistance developing in patients with Ménière’s disease. An increased level of circulating immune complexes has been found to be present in 96% of patients with Ménière’s disease.3
Despite the aforementioned evidence of immune activity, only 30% of patients with Ménière’s disease show evidence of a true autoantibody response to specific anticochlear antibody by western blot assay.20 Tests of abnormal cell-mediated immunity, such as the lymphocyte transfer test and the lymphocyte migration inhibition assay, have either been inconsistent, or have been found to be normal even in patients with known causes of autoimmune dysfunction of the inner ear, such as Cogan’s syndrome.20 It is clear that, in spite of our increasing understanding of inner ear immunoreactivity, we have not yet developed a reliable laboratory marker to “prove” autoimmune or allergic causation in a patient with Ménière’s or other forms of suspected inflammatory hearing loss.
Although the most accurate tests currently available to diagnose an autoimmune abnormality are often normal, there may be other immune-mediated causes for the development of symptoms. With an incidence of 20%, allergy is the most common “autoimmune” disease clinically. In a survey of 734 patients with Ménière’s syndrome, the prevalence of test-confirmed concurrent allergic disease was 41%, twice the incidence in the population in general.21 In a yet more recent survey study, patients reported a 58% rate of history of allergy, and, again, a 41% rate of positive skin or blood test.22 An increased incidence of self-reported migraine as well as allergic rhinitis has been reported in patients with Ménière’s disease as compared to a control group of age and sex-matched patients without Ménière’s attending an otolaryngology clinic.23 The prevalence of migraine in Ménière’s sufferers was 39%, while the rate in the control group was 18%. The prevalence of reported allergy in this study was also higher in those with Ménière’s disease, 51.9%, compared to 23% in the non-Ménière’s group.
This apparent relationship between allergic rhinitis, Ménière’s disease, and migraine is interesting in that all produce symptoms that are recurrent and paroxysmal. Vascular changes have been implicated to play an important role in all three conditions as well. While there are at least as many published “triggers” of migraine as there are of Ménière’s, the pathophysiology appears to be that of vasoconstriction, followed by vasodilation of meningeal vessels, with plasma protein extravasation.24 In a like manner, small ruptures in the membranous labyrinth secondary to changes in the cochlea microvasculature have been found to be associated with endolymphatic hydrops and Ménière’s disease.25,26
An elevated level of circulating immune complexes (CICs) has been reported in patients with allergic rhinitis and asthma, as well as those with Ménière’s disease.3,27 The whole concept of a sudden influx of fluid into the endolymphatic sac, producing a rupture of Reissner’s membrane, and the resulting production of Ménière’s symptoms would be very consistent with the vasodilation, fluid transudation, and inflammatory reaction that are the hallmarks of an allergic reaction.
Adding support to a hypothesized allergic component to symptom production in some patients with Ménière’s disease, Keles et al found total IgE to be elevated in 41.3% of patients with Ménière’s disease, but in only 19.5% of their control group.28 This is in contrast to an earlier study by Stahle et al who found no elevation of total IgE in patients with Ménière’s disease.29 However, adding support to an apparent allergic predisposition in Ménière’s, the Keles et al study also reported significant elevations of Th2 derived IL-4 in the Ménière’s disease group as compared with the controls.28
If we accept that 40% of patients with Ménière’s disease are also allergic, how do we distinguish which patients should undergo diagnostic testing and treatment? Should all patients with Ménière’s disease be tested for allergies? While the authors have reported a prevalence rate of allergy, confirmed by skin and/or in vitro testing in 40% of patients with Ménière’s, the corollary is that the other 60% do not have allergy. A careful history, including family history of allergy, as well as a physical examination specifically looking for other stigmata of allergy is essential in all patients with Ménière’s disease. It is the senior author’s opinion that it is the uncommon patient with Ménière’s and underlying allergy who does not also have other nonotologic physical signs or symptoms suggestive of an allergic diasthesis. An uncommon exception is the patient who has no family or childhood history of allergy, no history of upper or lower respiratory symptoms suggestive of allergy, but who will report a clear-cut relationship between Ménière’s symptom production and either season of the year or ingestion of a food that does not contain natural vasoactive compounds such as caffeine or has a high natural sodium content. Box 9.2 lists the type of symptoms that should alert the clinician to the possibility that an underlying problem with allergies may cause or contribute to Ménière’s disease symptoms in a given patient.
BOX 9.2 Indications for allergy testing in patients with Ménière’s disease
Childhood or past history of allergy
Patient suspects food reaction
Other allergic symptoms (asthma, rhinoconjunctivitis, etc.)
Steroid-dependent symptoms (rule out autoimmune inner ear disease)
There have been several studies from our institution to assess the profile and treatment outcome in patients with Ménière’s disease and allergy treated with specific immunotherapy and dietary elimination. In the first study, 93 patients with Ménière’s disease, diagnosed according to AAO-HNS standards, were tested for allergies.30 Criteria for patients in the testing group included a history of Ménière’s symptoms related to seasons, weather changes, or a suspect food; a known history of allergy; a significant childhood history of allergy; bilaterality of symptoms; or refractoriness to usual methods of treatment. Patients underwent control skin testing with histamine, saline, and glycerine, then the serial endpoint titration (SET) technique skin testing, now referred to as Intradermal Dilutional Testing, or IDT, for inhalant allergens. RAST screening was also performed in selected cases. Patients were asked to keep a food diary for 1 to 2 weeks before undergoing food testing with the Subcutaneous Provocative Food Test. In addition, IgG, IgE, and RAST tests were performed for selected foods.
Nearly a third (32.6%) of the patients felt that a reaction to a food provoked their Ménière’s symptoms. Many patients also felt that their symptoms were related to weather (23.7%) or seasonal changes (47.3%). Nine percent of patients had a history of a known autoimmune disease. Eighty-two percent of patients had a normal total serum IgE (<100 ng/ml). Antigen-specific IgE as measured by SET also tended to be of low levels, with the majority of endpoint dilutions to weed, grass, and tree pollens, as well as dust and mold, occurring in dilution #2 (1–500 w/v). The most common foods identified by provocative food testing (PFT) included wheat, milk, corn, egg, yeast, and soy. Following immunotherapy, 56 of the 90 patients with follow-up (62%) reported a decrease in both frequency and severity of vertigo attacks. Fifty percent also reported an improvement in tinnitus. None were worse.
In a second study, we evaluated the effect of specific allergy immunotherapy and food elimination of suspected food allergens on the course of patients with Ménière’s disease for whom allergy treatment had been recommended.31 Subjects were mailed a questionnaire regarding their symptoms. The 113 patients treated for symptoms of allergy using desensitization and diet showed a significant improvement from pre- to posttreatment, not only in allergy symptoms, but also in Ménière’s symptoms. The patient ratings of frequency, severity, and interference with everyday activities of their Ménière’s symptoms also appeared better after allergy treatment than ratings from the control group of 24 untreated patients. Vertigo control results, using the AAO-HNS classification, were 47.9% Class A or B. Hearing was stable or improved in 61.4%. Results indicate that patients with Ménière’s disease can show improvement in their symptoms of tinnitus and vertigo when receiving specific allergy therapy and suggest that the inner ear may also be the target, directly or indirectly, of an allergic reaction.
Although the above study asked patients to retrospectively rate their pretreatment symptoms, a more recent prospective study had 68 patients complete the questionnaire before treatment and at an average of 23 months follow-up.32 Results were similar, with significant improvement in frequency and severity of vertigo and unsteadiness, and improvement in the AAO-HNS disability scale and a number of quality of life scales (Table 9.1). Statistical analyses strongly suggested that these improvements were independent of medical treatment for Ménière’s disease and were not likely related just to natural history.
TABLE 9.1 Paired comparison of symptoms at initial and follow-up intervals for 68 patients with Ménière’s disease and allergy undergoing immunotherapy and/or diet treatment for allergy32
| Rights were not granted to include this data in electronic media. Please refer to the printed book. |
Clearly, a weakness of these studies, as well as other case reports and series suggesting that antigen-specific immunotherapy or dietary food elimination results in an improvement in the symptoms of Ménière’s disease, is that there is no control group receiving saline injections or given diets eliminating foods that were negative on testing. It has been our observation that patients with Ménière’s disease as well as allergic rhinitis are reluctant to commit to months or a year of possible placebo injections to “prove” that immunotherapy may be helpful in improving symptoms of vertigo, hearing loss, and/or tinnitus. For the present, we rely on the use of statistical control as well as research that clearly demonstrates the ability of allergy immunotherapy to downregulate Th2-driven inflammatory responses in patients with allergic rhinitis and asthma.33 If Ménière’s disease is believed to be a chronic condition with an inflammatory component, it is logical that downregulating the production and release of both proinflammatory and vasoactive mediators that promote fluid extravasation and/or retention could be helpful in lessening symptoms. This has certainly been the rationale for the use of steroids and even dietary restriction of salt in patients with Ménière’s. Interestingly, increased levels of sodium have been shown to increase the vasodilatory effect of histamine.34
While there is no universal agreement, the symptoms of Ménière’s disease – vertigo, hearing loss, and tinnitus – are thought to be produced by a sudden influx of fluid into the endolymphatic sac, producing a rupture of Reissner’s membrane in the cochlea. The resulting potassium intoxication of the auditory and vestibular nerves causes the local neurological changes. This increase in fluid could be caused by a sudden cessation of endolymph resorption in the endolymphatic sac, or could be secondary to the rapid production of endolymph in either the stria vascularis or the endolymphatic sac. The site is more likely the endolymphatic sac; the sac is not only capable of secretion as well as absorption, it is also known that the response of the sac to inner ear disturbance actually appears to be an increase in its secretory activity.35
Increasingly, there is evidence that it may also be necessary to have an anatomic variant in order to develop Ménière’s disease. It has been noted that the endolymphatic sac is smaller in patients with Ménière’s disease than in normal controls (Figure 9.1).36 Yet, we also find patients with smaller than average endolymphatic sacs in this group who did not develop Ménière’s disease. We could theorize that perhaps a smaller sac in the presence of a patient with allergy, or some other condition resulting in local inflammation, would predispose that individual to being less able to handle the sudden secretion of endolymph that could be stimulated by an underlying problem with allergy.
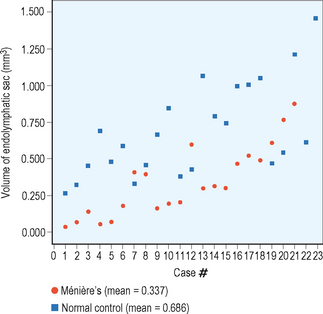
Figure 9.1 Endolymphatic sac volume (mm3) for 21 patients with Ménière’s disease and 23 normal controls.
(Data courtesy of Fred Linthicum, MD, House Ear Institute, 2006.)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


