Chapter 4 Management of the Patient with Rhinosinusitis
Introduction
Rhinosinusitis is one of the most common and prevalent illnesses throughout the world. Both acute and chronic forms of rhinosinusitis (RS) have been described, and affect patients of all ages. By a variety of reports, the incidence of RS is increasing, and the number of patients diagnosed around the world with RS continues to climb.1 Allergy plays a role in the pathogenesis and expression of symptoms among patients with both acute and chronic RS, although the precise relationship between atopy and the presence of sinus disease can be difficult to define. Due to the heterogeneity seen in acute and chronic RS, consensus panels have been convened to provide clarity to the diagnosis of these common conditions, and to develop guidelines for further research and optimal treatment. This chapter will discuss the various types of RS, diagnostic strategies, and treatment options for both acute and chronic rhinosinusitis.
Prevalence and Burden of Rhinosinusitis
From a variety of sources, it has been noted that RS is increasing in prevalence. In the USA alone it is estimated to affect as many as 31 million patients on an annual basis.2 It accounts for billions of dollars in expenditure, with significant increases in direct and indirect costs noted over a several year period.3 In addition, 15% of the US population is symptomatic from sinusitis for a period of at least 3 months annually.4
While most adults will experience between two and four acute upper respiratory infections annually, less than 2% of these episodes are due to acute bacterial rhinosinusitis (ABRS).5 By calculation, there would therefore be an expected 20000000 cases of ABRS in the USA alone on a yearly basis. RS was estimated to account for 9% of pediatric and 21% of adult prescriptions in the USA annually,6 with over $3.5 billion USD spent in 1999 funds for the treatment of ABRS alone.7
Two recent studies have examined the burden of chronic rhinosinusitis (CRS) on both patient impact and financial cost. Bhattacharyya followed 322 patients with CRS prospectively over a 1-year period.8 During that 1-year period, patients received an average of 2.7 courses of oral antibiotics, and used nasal steroids for over 18 weeks. In addition, patients missed an average of 4.8 days of work related to CRS and had mean medical expenses of US$921. In a second study by Murphy et al, over 200 000 patients in a health maintenance organization (HMO) were surveyed during the 1-year period 1994.9 Approximately 10% of patients in the HMO were identified with diagnoses of CRS during this one year. Among this patient group, CRS was responsible for an average of 2.0 office visits and 5.1 pharmacy fills per patient during 1994. Extrapolating to the general US population, this study estimated the overall direct cost of CRS in 1994 to be US$4.3 billion.
In addition to the clear economic burden of both acute and chronic RS, both of these diseases exert significant impact on patient symptoms and quality of life. Gliklich and Metson assessed this impact, and noted that RS is associated with a more negative quality of life than other common medical diseases such as chronic obstructive pulmonary disease and lower back pain.10
Definition of Rhinosinusitis
The term that is currently accepted by the majority of specialists who manage patients with acute and chronic illnesses affecting the paranasal sinuses is rhinosinusitis. While there is still some debate regarding the use of this term, and while there are individuals who prefer the older term sinusitis, rhinosinusitis is the accepted term agreed to by a consensus group of American medical societies, including the American Academy of Allergy, Asthma and Immunology (AAAAI), the American Academy of Otolaryngic Allergy (AAOA), the American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS), the American College of Allergy, Asthma and Immunology (ACAAI), and the American Rhinologic Society (ARS).11 The choice of the term rhinosinusitis implies that the physiological condition of the sinuses correlates closely with the concurrent condition of the nose. Nasal disease, i.e. rhinitis, usually precedes the development of sinus disease, and sinusitis is rare without rhinitis.1,11,12 Given the contiguity of the nasal and sinus mucosa and the interdependency of the nose and sinuses, the term rhinosinusitis (RS) appears to be a more representative name for this process, and will be used in the current chapter.
In 1996, a task force of the AAO-HNS reviewed the current state of knowledge in RS, and drafted a definition statement based upon this expert panel. They defined RS as “a condition manifested by an inflammatory response involving the following: the mucous membranes (possibly including the neuroepithelium) of the nasal cavity and the paranasal sinuses, fluids within these cavities, and/or underlying bone.”1 The key message implied from this definition is that RS is primarily an inflammatory disease, not an infectious disease. Infection is only one type of pathophysiological process that can affect the sinuses. In addition, recognizing the close relationship between the nose and sinuses, a conjoint conference involving the American allergy/immunology and otolaryngology communities concluded that “rhinosinusitis may be a more appropriate term than either rhinitis or sinusitis alone.”12 Similar definitions have been applied by the European allergy and otolaryngology communities.13
In 2003, the Sinus and Allergy Health Partnership (SAHP), a conjoint society made up of representatives from the AAOA, the AAO-HNS, and the ARS, also met to consider the knowledge base around RS, and drafted a similar definition to that offered in 1996. The SAHP defined RS as “a group of disorders characterized by inflammation of the mucosa of the nose and the paranasal sinuses.”14 The 2004 consensus panel decided to “endorse and adopt” this definition for framing future research strategies and diagnostic and treatment methodologies.11 The members of this panel recognized that inflammatory processes simultaneously affect the nose and sinuses, and that the term rhinosinusitis best describes this concurrent process.
Classification of Rhinosinusitis
▪ RS: 1997 Consensus
In the 1997 system, the diagnosis of RS was based purely on patient symptoms. These symptoms were broken down into major and minor factors that were associated with the presence of RS. These major and minor factors are noted in Box 4.1. It is important to note that headache or facial pain are not sufficient symptoms for the diagnosis of RS in the absence of other major or minor factors, primarily nasal in origin. These criteria are useful in assisting the clinician in the consideration of the diagnosis of acute or chronic RS, but do not require the presence of confirmatory findings on either physical examination or radiological imaging to apply a diagnosis. This lack of confirmation was felt to be a weakness in the 1997 document.
BOX 4.1 Factors associated with a diagnosis of rhinosinusitis.
(Adapted from Lanza DC, Kennedy DW. Adult rhinosinusitis defined. Otolaryngol Head Neck Surg 1997;117:S1–S7)
a Facial pain/pressure alone does not constitute a suggestive history for rhinosinusitis in the absence of another major nasal symptom or sign.
b Fever in acute sinusitis alone does not constitute a strongly suggestive history for acute rhinosinusitis in the absence of another major nasal symptom or sign.
The 1997 task force also described the temporal course of RS and divided RS further into five categories, three primary categories: acute rhinosinusitis, recurrent acute rhinosinusitis, and chronic rhinosinusitis; and two derivative categories: subacute rhinosinusitis and acute exacerbations of chronic rhinosinusitis. The three primary groupings are often used to delineate the time course of RS in individual patients and to assist in the development of appropriate treatment modalities (Figure 4.1).
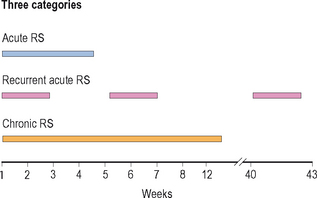
Figure 4.1 Temporal course of rhinosinusitis: acute, recurrent acute, and chronic.
(Adapted with permission from Lanza DC, Kennedy DW. Adult rhinosinusitis defined. Otolaryngol Head Neck Surg 1997;117:S1–S7.)
Acute Rhinosinusitis
Acute rhinosinusitis (ARS) is a very common condition, and generally has a sudden onset of symptoms, often following a viral upper respiratory infection. It is defined as lasting from 1 day to 4 weeks. It is important to distinguish between a viral upper respiratory infection, which is very common, and an acute bacterial rhinosinusitis. The most robust method of distinguishing these two conditions is the temporal course of the illness. Viral symptoms generally peak within 3 or 4 days of onset and then decline in severity. By contrast, acute bacterial RS generally worsens after 5 days and persists longer than 10 days.15 In addition, certain physical signs are suggestive of a diagnosis of acute bacterial RS. Facial erythema or swelling are associated with bacterial disease, although they are uncommon. Maxillary tooth pain is correlated well with the presence of bacterial disease, and when accompanied with fever often confirms the presence of acute bacterial RS.16
Recurrent Acute Rhinosinusitis
Many patients may experience episodes of acute bacterial RS that last 7–10 days and respond rapidly to treatment, yet seem to have frequent recurrent episodes with a similar pattern. Between symptomatic episodes, these patients may be clear of any symptoms of nasal or sinus disease. The frequent recurrent nature of these episodes suggests a separate categorization of disease, which has been called recurrent acute RS. While there are not strict criteria for the diagnosis of this process, some authors have suggested that patients should experience at least four episodes of acute RS within a year, and that intervening periods without symptoms should be at least 8 weeks.1,17 It is not clear whether recurrent acute RS is a distinct pathophysiological entity, reflecting a unique underlying process, or if it simply reflects random variation in the frequency of disease.
Chronic Rhinosinusitis
Chronic rhinosinusitis (CRS) is in many ways a distinct pathophysiological process that reflects the chronic inflammatory nature of the disease. It is not simply acute disease that has not resolved or has progressed into chronic disease. From a temporal standpoint, CRS is generally classified as persistent sinonasal symptoms for at least 12 weeks,11,18 although some systems suggest that 8 weeks may be adequate to classify the disease as CRS.19 CRS likely has numerous mechanisms involved in its pathogenesis, and is probably best considered as a syndrome rather than a unique pathophysiological entity. Recent classification systems make clear distinctions between CRS with the presence of nasal polyps (CRSwNP) and CRS without the presence of nasal polyps (CRSsNP).11,13
▪ RS: 2004 Consensus
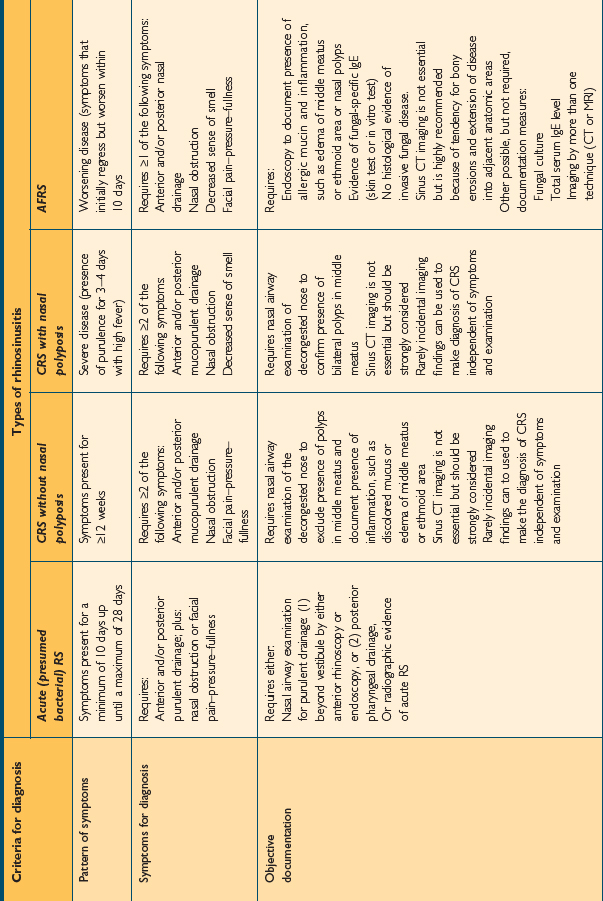
The 2004 consensus document broadens the criteria necessary for the diagnosis of RS. While the document is designed to promulgate diagnostic criteria for research studies and clinical trials, it is practical to include some element of objective evidence into diagnostic practices when managing the patient with presumed RS. This document sets out specific criteria for the diagnosis of various forms of RS based on patient symptoms, the pattern of those symptoms, and the presence of objective documentation. It describes specific definitions for patient care. These consensus criteria are noted in Table 4.1.
TABLE 4.1 Rhinosinusitis consensus definitions for patient care. (Source: Meltzer EO, Hamilos DL, Hadley JA, et al. Rhinosinusitis: establishing definitions for clinical research and patient care. Otolaryngol Head Neck Surg 2004;131:S1–S62)
Allergic Fungal Rhinosinusitis
Allergic fungal rhinosinusitis (AFRS) is classically described as a type of CRS with or without polyposis that is associated in its expression and pathogenesis with an IgE-mediated response to one or more families of fungal organisms. These organisms are present in the sinuses of patients with AFRS, and patients will demonstrate an IgE-mediated hypersensitivity reaction to those fungi, either by in vitro specific IgE testing or through skin tests for relevant fungi. AFRS is not diagnosed in the absence of confirmatory IgE testing, despite the presence of fungi on either culture or histopathology. The diagnosis of AFRS requires the presence of nasal and sinus symptoms for at least 12 weeks, including anterior/posterior mucopurulent drainage, nasal obstruction, and facial pain-pressure-fullness. It also requires a nasal airway examination demonstrating allergic mucin and inflammation, with or without nasal polyps. CT imaging is important to demonstrate the extent of the disease. In addition, physical examination and CT imaging should not demonstrate the presence of changes consistent with invasive fungal sinusitis.
Anatomy of the Paranasal Sinuses
Ethmoid Sinuses
The anatomy of the ethmoid sinuses is variable. They can be best viewed as a group of discrete cells separated into anatomic regions by a series of bony partitions. These cells can be grouped into two units: the anterior ethmoid cells, which are numerous and smaller in size, and the posterior ethmoid cells, which are less numerous and larger.
Frontal Sinuses
The sinus chambers are lined with a ciliated pseudostratified columnar respiratory-type epithelium. This mucosa is similar histologically to that seen in the nose and the lower respiratory tract (Figure 4.2). This histological similarity is one reason that inflammatory respiratory diseases commonly affect more than one portion of the respiratory tract simultaneously. This epithelium secretes mucus, which is swept from the interior of the sinuses to the ostia and into the nose by fine cilia on the surface of the mucosal cells. This mucus blanket traps particles in the nose and sinuses, and transports these particles posteriorly into the nasopharynx, where they then can be swallowed. Particulate matter that can affect the nasal and sinus mucosa includes bacteria, viruses, irritants, and allergens.
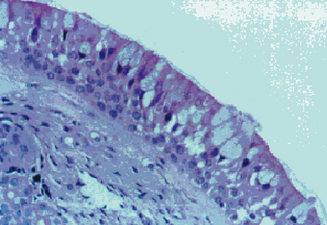
Figure 4.2 Appearance of the normal respiratory epithelium of the nose and paranasal sinuses.
(Reproduced with permission from Minshall E, Ghaffar O, Cameron L, et al. Assessment by nasal biopsy of long-term use of mometasone furoate aqueous nasal spray in the treatment of perennial rhinitis. Otolaryngol Head Neck Surg 1998;118:648–654.)
Physiology of the Sinuses in Health and Disease
In healthy sinuses, mucus is secreted by goblet cells within the epithelium and transported to the ostia of the sinuses for clearance into the nose. This process for the transport of mucus within the nose and sinuses is known as mucociliary clearance. Through active action of the cilia, mucus is easily moved from the periphery of the sinuses toward the ostia. This mucociliary clearance is generally rapid and efficient, and prevents the accumulation of mucus and particulate debris within the sinus chambers. It is essential for normal sinus health and function (Figure 4.3). Mucociliary clearance patterns within the sinuses are genetically directed to maintain the flow of mucus from the sinuses through the sinus ostium and into the nose itself.20
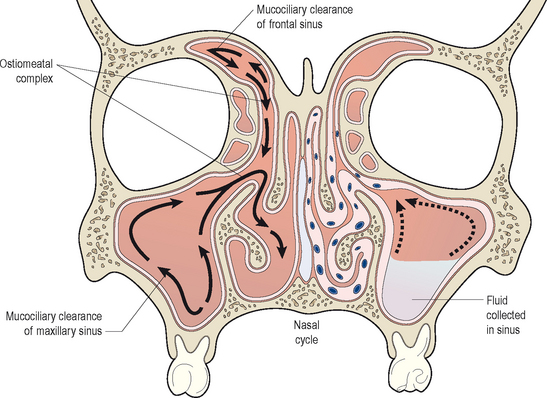
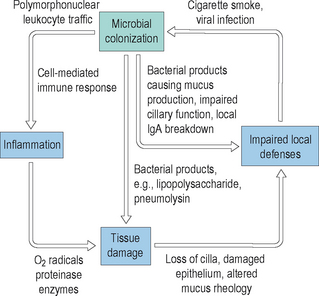
By contrast, when normal mucociliary clearance is inhibited, either through local physiological changes or through anatomic obstruction, the sinuses become diseased. It is clear that ventilation of the sinuses and drainage of mucus out of the sinuses maintains the normal physiology of the sinuses. Disruptions to this normal ventilation and drainage is a central factor in the pathogenesis of acute and chronic rhinosinusitis.21 Many factors can adversely influence the clearance of mucus from the sinuses, and thereby result in acute and chronic changes. Mucociliary clearance can be directly affected by ciliostatic agents, such as tobacco smoke and viral infections. Both irritants such as smoke and viral disease disrupt the cilial layer in the sinuses, resulting in cilial loss and impaired cilial motility. With impairment of the normal clearance mechanisms of the sinus mucosa, mucus stasis occurs and bacterial colonization can begin. As bacteria colonize the sinuses, they can proliferate within the mucus layer and can cause localized acute inflammation. This inflammation will cause tissue edema and ostiomeatal narrowing, which can result in additional injury to the mucosa. In addition, any structural obstruction to the ostia or significant decrease in their diameter will further impair mucociliary clearance and lead to increased bacterial growth. In response to the increased presence of bacteria, normal host mechanisms will recruit neutrophils and other inflammatory cells into the sinuses, resulting in increased local inflammation and secondary injury to the mucosa. An illustration of this inflammatory cycle is displayed in Figure 4.4.
The consequence of this cyclical inflammation is the creation of conditions that support the development of both acute and chronic rhinosinusitis. As also demonstrated in Figure 4.3, in contrast to the normal physiology of the healthy sinuses, in diseased sinuses conditions exist that favor the proliferation of bacteria and the development of symptoms. In diseased sinuses pressure is created from tissue edema, resulting in contact between the mucous membranes of the nose, turbinates, and sinuses. This contact stimulates nerve fibers resulting in localized pain. In addition, bacteria multiply within the chambers of the sinuses, resulting in additional pain as mucosal swelling increases. In addition, fever is common in response to the presence of infection and the host response generated by the infection. It is clear from this model that normal mucociliary clearance is essential in the normal physiological functioning of the sinuses.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


