Chapter 102 Primary Vitrectomy in Rhegmatogenous Retinal Detachment
 For additional online content visit http://www.expertconsult.com
For additional online content visit http://www.expertconsult.com
Introduction
Currently, rhegmatogenous retinal detachment (RRD) continues to be an important cause of visual loss. The fundamental principles involved in reattachment of a retina include identification of all retinal breaks, and relief of the vitreous traction. Traditionally, scleral buckling (SB) was viewed as the gold standard treatment for uncomplicated RRD. Pars plana vitrectomy (PPV) was traditionally reserved for treatment of eyes with complications, such as those showing giant retinal tears or exhibiting significant proliferative vitreoretinopathy (PVR). In the 1980s, the indications for PPV in RRD patients were broadened to include less complicated instances, and the term “primary vitrectomy” was introduced by Klöti.1
As the necessary instrumentation for, and safety of, PPV continue to improve with developments in microscope technology, intensified endoillumination, and wide-angle viewing systems, the indications for vitrectomy in RRD have been further expanded to include most patients with RRD. Indeed, PPV is more useful than SB in eyes requiring simultaneous cataract extraction or those of pseudophakic status.2–8
Pathogenesis of Rhegmatogenous Retinal Detachment
Liquefaction of the vitreous occurs naturally upon aging, developing more rapidly in eyes with significant myopia, surgical or non-surgical trauma, and/or intraocular inflammation. Apart from liquefaction, alterations in the extracellular matrix of the vitreous facilitate detachment of the posterior vitreous from the underlying retina. PVD usually presents as an acute event, and is more prevalent in patients older than 50 years, with frequencies as high as 53%.9 PVD often precipitates RRD because the tractional forces necessary to generate retinal breaks are produced upon development of PVD, although not all retinal breaks progress to detachment. The reported incidence of retinal tears in patients with acute symptomatic PVD varies from 8–46%.10 In a study in a general population,11 18% of eyes with retinal breaks developed retinal detachment. Risk factors for progression included fresh, symptomatic, horseshoe-shaped tears; breaks suggestive of the presence of subclinical retinal detachment (RD); and pseudophakia/aphakia.
Categories of Rhegmatogenous Retinal Detachment
The number of aphakic/pseudophakic patients with RRD has increased significantly over the past decades. After cataract surgery, vitreous liquefaction accelerates, causing premature PVD and subsequent RD. Aphakic/pseudophakic eyes tend to have small (and sometimes multiple) anterior breaks. The status of the posterior capsule also influences the speed of vitreous liquefaction. One study found that Nd:YAG laser posterior capsulotomy increased the risk of RD after cataract extraction up to 4.9-fold.12 Because of the characteristics of the breaks and the status of the vitreous in aphakic/pseudophakic eyes, vitrectomy is preferred by many surgeons and has a good success rate.13
Patient selection for primary vitrectomy
SB and/or pneumatic retinopexy serve as the first treatment option(s) in patients with localized detachment in one quadrant together with single neighboring breaks. Young age and anteriorly located small holes in phakic patients encourage the use of SB. The success rates of final reattachment are 90–95%.14
Recent developments in vitrectomy instruments, including small-gauge systems, wide-angle viewing systems, and endoilluminators, as well as adjuvants, including triamcinolone acetonide suspension, perfluorocarbon liquids, and intraocular tamponades, led the choice of surgical technique for the treatment of RRD with medium-complexity shift more and more towards PPV.15–17 During the last 5 years, several surgeons have reported that primary vitrectomy is the method of choice in 40–80% of all patients with RRD.17,18
Several trials comparing PPV to SB in patients undergoing RRD surgery have been reported.19–23 In general, PPV was favored for treatment of pseudophakic eyes with unseen breaks, eyes featuring ocular hypotony, or eyes showing prolonged macular detachment. One large-scale prospective multicenter randomized trial, scleral buckling versus primary vitrectomy in rhegmatogenous retinal detachment study (the SPR Study), also supported the superiority of PPV in the pseudophakic/aphakic eyes, in terms of a primary success rate and a rate of retina-affecting secondary procedures. This study, however, showed no differences in phakic eyes.19
Surgical techniques
Primary vitrectomy is commonly performed using a wide-angle viewing system attached to an operating microscope. The surgical steps of primary vitrectomy using sutureless MIVS are described below (Figs 102.1–102.4).
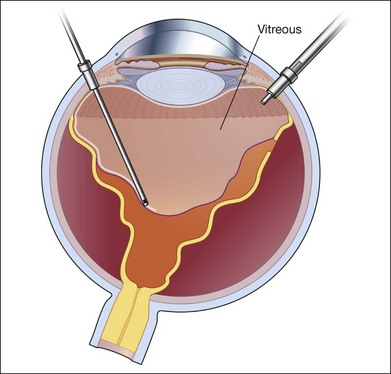
Fig. 102.1 Detached retina with posterior vitreous detachment is shown. Core vitrectomy is performed.
Core vitrectomy
First, the central vitreous is removed (Fig. 102.1). When PVD is absent, or even when PVD has occurred, triamcinolone acetonide can be injected to afford better visualization of the vitreous gel, to facilitate PVD, and to completely remove the residual vitreous. The posterior vitreous membrane can be removed using a diamond-dusted scraper; this prevents secondary macular pucker (Fig. 102.5).
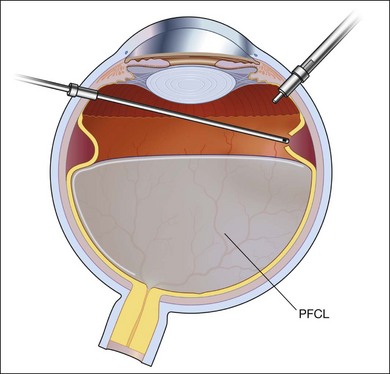
Peripheral vitrectomy
After core vitrectomy, PVD is further extended using a wide-angle viewing system. Usually, PVD is already present, up to the positions of the retinal breaks. However, abnormal attachment may be noted in other locations. If retinal breaks are located posterior to the equatorial zone, the vitreous bridge between the tears and the ora serrata must be separated and removed. If the breaks are peripheral to the equatorial zone, the vitreous on the flap should be shaved away, with scleral indentation. In case of bullous RD, perfluorocarbon liquid (PFCL) may be injected to flatten the detached retina, so that the peripheral vitreous can be safely shaved without creating an iatrogenic tear (Fig. 102.2).
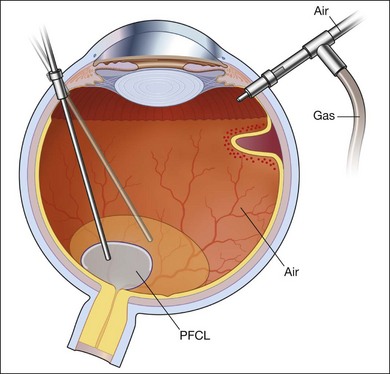
Fluid–air exchange
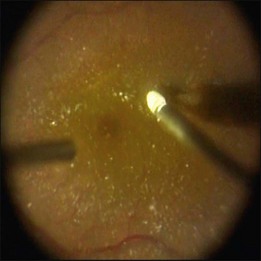
Subretinal fluid is removed through the original breaks using a backflush needle in the presence of air irrigation. PFCL may be injected, up to the level of the posterior edge of the break; the PFCL bubble displaces posterior subretinal fluid through the break. Next, air–fluid exchange at the top of the PFCL bubble may displace peripheral subretinal fluid through the break. PFCL is not indicated for all eyes. The preferable indications are bullous RD or RD that is associated with retinal breaks anterior to the equatorial zone; the subretinal fluid can thus be removed without creating a drainage retinotomy (Fig. 102.4).
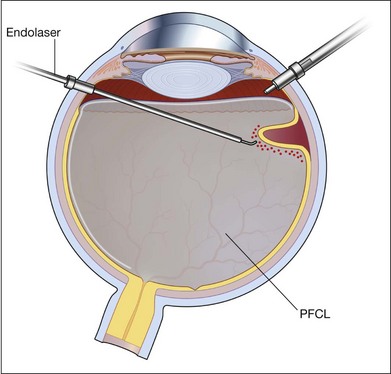
Photocoagulation/cryopexy of the retinal tear
Whenever retinal breaks are found, endodiathermy may be used to mark the breaks. Once retinal reattachment is complete, endophotocoagulation is performed under air or a PFCL bubble. Two-to-three rows of laser burns can be applied, around each break and site of lattice degeneration (Fig. 102.3). Strong photocoagulation should be avoided on the thin retina detached by the residual subretinal fluid. Alternatively, cryopexy may be utilized if a break is located at the far periphery of phakic RD eyes.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


