Primary Angle-Closure Glaucoma
JoAnn A. Giaconi
Simon K. Law
Joseph Caprioli
Primary angle-closure glaucoma (PACG) has received increasing amounts of research and clinical attention since the 1990s, as appreciation has been gained of its high worldwide prevalence and visual morbidity. Primary angle-closure glaucoma is a particularly visually destructive form of glaucoma. Although it accounts for just one quarter (26%) of the 60.5 million people that will be affected with glaucoma in a 2010 projection, based on prevalence models and United Nation world population projections, angle-closure glaucoma will account for almost half (46%) of the cases of glaucoma blindness.1
In recent decades, the definition of PACG has been formalized. Understanding of its pathophysiology has led to the recognition that different mechanisms of angle closure may be responsible in different ethnic groups. It has been suggested that angle-closure glaucoma is not a single entity but a number of different disorders with a final common pathway.2 A number of large epidemiologic studies have been undertaken to understand the extent of the disease and the related public health concern. Various treatments and their long-term outcomes are under formal study, which will lead to enhanced evidence-based treatment. However, it is important to recognize that in older reports, nonstandardized definitions of the disease and less-than-ideal methodology were used, and so there remain many unanswered questions about PACG as we await the results of newer studies.
Nomenclature
Angle closure is defined by the apposition of peripheral iris to trabecular meshwork that leads to reduced drainage of aqueous humor through the anterior chamber angle. Terminology for PACG is inconsistent throughout the literature, which sometimes leads to the grouping of related but separate entities that may have different prognoses and treatments.
For some time, classification was based on clinical observations of the disease in Western populations, in which the condition is relatively uncommon but often symptomatic. With the recognition that a chronic, asymptomatic form of PACG predominates in the world, groups interested in the epidemiology of glaucoma who met at the International Society for Geographical and Epidemiological Ophthalmology (ISGEO) in the Netherlands in 1998 and the World Health Organization (WHO) in 2001, proposed redefining the disease. The proposed classification scheme sought to provide a more uniform definition of the disease and one that was consistent with the classification of primary open-angle glaucoma (POAG).3,4,5
In the newer system (Table 53.1), the term glaucoma is reserved for people with established, visually significant end organ damage as evidenced by glaucomatous optic neuropathy (GON). The use of angle closure is appended to glaucoma if the cause of GON is elevated intraocular pressure (IOP) through the apposition of iris to trabecular meshwork. Therefore, an individual with acute angle closure and increased IOP will not be considered to have angle-closure glaucoma unless optic neuropathy is also present. Individuals with gonioscopic criteria of narrow angles and evidence of significant obstruction of the functional trabecular meshwork by peripheral iris, such as peripheral anterior synechiae (PAS), are classified as having primary angle closure (PAC). Primary angle closure can include both symptomatic and asymptomatic individuals. If PAC is accompanied by significant glaucomatous damage to the optic nerve, this is defined as primary angle-closure glaucoma (PACG). In primary angle-closure suspects (PACS), appositional contact between peripheral iris and posterior trabecular meshwork is considered likely. This group has no evidence of glaucoma or damage to the angle, i.e., no elevation of IOP or PAS.
Table 53.1 Primary Angle Closure Definitions | |||||||||
|---|---|---|---|---|---|---|---|---|---|
|
A categorization of disease stage (PACS, PAC, or PACG) does not identify the mechanism causing the angle closure. Causes of angle closure include pupillary block, plateau iris, lens-induced, and retrolenticular mechanisms.6 The recognition that Asians tend to have a different type of angle closure than Caucasians led He et al.7 to substitute the term plateau iris with “anterior nonpupillary block” because some cases of angle closure remaining after peripheral iridotomy (PI) do not display the characteristics of classic plateau iris. The term anterior nonpupillary block encompasses angle closure caused by peripheral iris crowding and prominent last iris roll.7
The newer unified scheme classifies the disease according to the physical signs of end organ damage and has the advantage of recognizing the disease in its earliest and most treatable forms. It removes a source of confusion in the traditional terminology—acute, subacute, intermittent, chronic, creeping, and mixed mechanism—that relies primarily on the degree or duration of symptoms. The term “acute” has been applied to cases with at least two of the following symptoms: ocular or peripheral ocular pain, nausea or vomiting, and a history of intermittent blurring of vision with haloes; and at least three of the following signs: IOP greater than 21 mm Hg, conjunctival injection, corneal epithelial edema, middilated unreactive pupil, and shallow anterior chamber in the presence of an occludable angle.8 The terms “intermittent” or “subacute” can be used interchangeably and are used to characterize repeated, brief episodes of angle closure with the symptoms and signs described previously that resolve spontaneously. “Chronic” refers to an eye in which there is a gradual asymptomatic closure of the angle via the formation of PAS that results in an elevation of IOP.9,10 “Creeping” angle closure is a subtype of the chronic form in which PAS formation slowly advances circumferentially, usually starting superiorly, and making the iris insertion appear to become more and more anterior.11 In “mixed-mechanism” or “multimechanism” glaucoma, an element of pupillary block contributes to the angle closure in addition to lens-related mechanisms, malignant glaucoma, and/or anterior nonpupillary block.12
Pathophysiology
Primary angle closure is the result of pupillary block and anterior nonpupillary block mechanisms that can include plateau iris and prominent last iris roll. Lenticular and retrolenticular mechanisms are classically defined as secondary causes of angle closure (Table 53.2). Pupillary block is the most understood mechanism and is discussed first.
Table 53.2 Mechanisms of Angle-Closure Glaucoma (Both Primary and Secondary) | |||||||
|---|---|---|---|---|---|---|---|
|
Pupillary block is a frequent cause of primary angle closure. In 1920, Curran.13 documented the beneficial effect of iridotomy in eyes with angle-closure attacks and proposed that there was impaired aqueous humor flow into the anterior chamber. After laser iridotomy, pigment can be seen to flow from the posterior to the anterior chamber, the forward convex shape or bowing of the iris flattens, and the central iris settles on the lens. All of these signs result from the alternate route of flow created by the iridotomy that allows the obstruction of aqueous flow at the pupil to be bypassed.
Aqueous humor is produced by the ciliary body and normally moves from the posterior chamber through the pupil into the anterior chamber (Fig. 53.1). The movement of aqueous from posterior to anterior chambers occurs across a pressure gradient, with the pressure behind the iris being slightly greater than that in front of the iris. In most clinical situations, it is believed that the pressure differential is only 1 to 2 mm Hg14 This small pressure differential across the iris causes it to bow forward slightly. This natural anatomic configuration has been seen with Scheimpflug photography.15 During its passage, aqueous encounters resistance at the iris–lens channel, which is estimated to be less than 25 microns in width.16 Ultrasound biomicroscopy has suggested that the iris actually rests on the lens.17 Resistance at the iris–lens channel is the phenomenon of relative pupillary block (Fig. 53.2). Relative pupillary block is present in most phakic eyes. Additional factors are necessary for this block to become abnormal and lead to angle closure. As relative pupillary block increases, for example when the pupil is middilated and the iris rests more firmly against the lens, the pressure gradient between the posterior and anterior chambers increases, causing further bowing forward of the iris (Fig. 53.3). This process can continue until the iris comes into contact with the trabecular meshwork, which will eventually block aqueous outflow through the meshwork and cause the IOP to rise to very high levels (Fig. 53.4). Absolute pupillary block occurs when there is synechial closure of the pupil edges to the lens capsule completely obstructing aqueous flow. Of note, pupillary block can also occur if the pupil edge adheres to an intraocular lens, capsular remnants, vitreous face, air, or silicone oil.
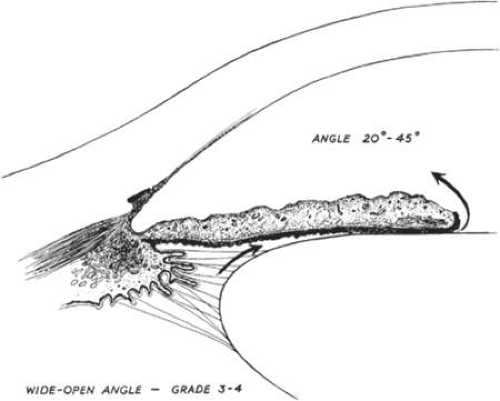 Figure. 1. Anterior chamber angle width. Cross-sectional diagram of a deep anterior chamber with a nearly flat iris plane, minimal apposition between the iris and lens at the pupil, and a wide-open angle entrance to the filtration area. In this type of eye, aqueous passes easily from the posterior chamber through the pupil into the anterior chamber and out through the filtration area. (Kolker AE, Hetherington J Jr: Becker and Shaffer’s Diagnosis and Therapy of the Glaucoma, p 42. St. Louis, CT Mosby, 1970) |
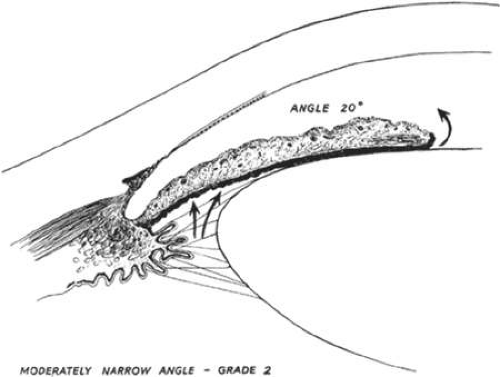 Figure. 2. Anterior chamber angle width. A Shallow anterior chamber with a more anteriorly located lens than is shown in Figure 1. Apposition of the lens and iris in the pupillary zone is increased, producing a relative pupillary block that interferes with aqueous flow from the posterior to the anterior chamber. The pressure differential between the posterior and anterior chambers is increased. (Kolker AE, Hetherington J Jr: Becker and Shaffer’s Diagnosis and Therapy of the Glaucoma, P 42. St. Louis, CV Mosby, 1970) |
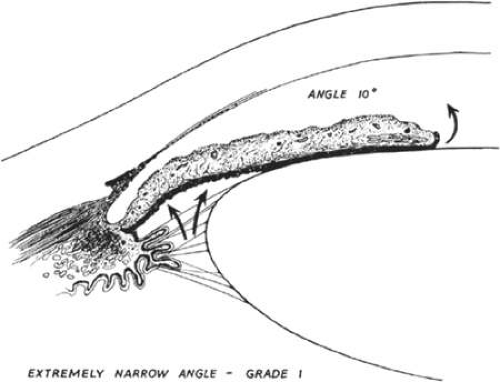 Figure. 3. Anterior chamber angle width. Extremely narrow anterior chamber angle entrance with a mid-dilated pupil and a lax peripheral iris. Increased pressure in the posterior chamber pushes the peripheral iris forward where it lies near the filtration area; at this stage, it does not block outflow of aqueous or increase intraocular pressure. (Kolker AE, Hetherington J Jr: Becker and Shaffer’s Diagnosis and Therapy of the Glaucoma, p 43. St. Louis, CV Mosby, 1970) |
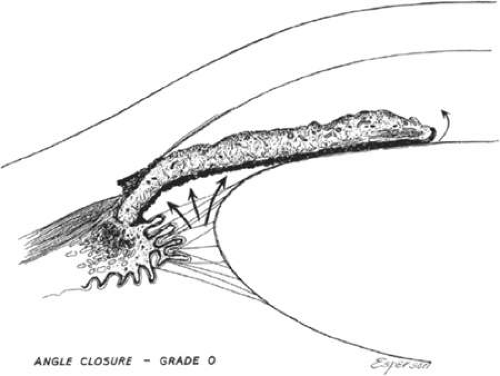 Figure. 4. Anterior chamber angle width. The angle has closed and the iris now lies against the trabecular meshwork, obstructing outflow. If closure has occurred around a significant portion of the circumference of the angle, intraocular pressure will rise. (Kolker AE, Hetherington J Jr: Becker and Shaffer’s Diagnosis and Therapy of the Glaucoma, p 43. St. Louis, CV Mosby, 1970) |
It was suggested first by Chandler18 and Lowe19 that pupillary block is simply the consequence of contact between the iris and anterior lens surface. Lowe.11 later proposed a more sophisticated model of pupillary block, describing a conceptual force vector onto the lens surface resulting from co-contraction of the sphincter and dilator iris muscles. Mapstone then refined this model, using pharmacologic provocation tests and anterior segment photographs, and proposed that it resulted from three forces, sphincter and dilator muscles, iris elasticity, and relative or absolute obstruction to aqueous flow.20 Pupillary block is the consequence of multiple forces acting between the lens and iris.
Given that anterior iris bowing figures prominently in acute angle closure, it has been studied in detail. Tiedeman.21 modeled the forces accounting for the naturally occurring convexity of the iris, including the forces of the radially oriented dilator fibers, the centrally oriented sphincter, the force acting to hold iris to the iris root, and the hydrostatic pressures in the two chambers that lift the iris away from the lens. The model shows that the iris takes on an anteriorly convex shape, and that this convexity increases when the lens is located more anteriorly relative to the iris root. The model also predicts that the iris shape comes closest to closing off the angle when the pupil is in the middilated position, a feature that is clinically seen during acute attacks. Silver and Quigley.22 modeled the resistance at the lens–iris channel using different values for the channel height and length. Varying these anatomic dimensions, as well as aqueous flow and pupil diameter, they suggested that the posterior chamber pressure could be substantially higher than in the anterior chamber. It has been speculated that iris thickness may affect convexity. In a laboratory model simulating anterior segment structures, it was found that although doubling the iris thickness did not alter iris shape, it did increase the posterior to anterior pressure differential.23 The dark-brown irises of more heavily pigmented people may generate larger pressure differentials between posterior and anterior chambers than that seen in eyes with thinner, lightly colored irises. Combining the information from these models helps to explain why certain eyes can develop an iris shape that appositionally closes the angle.24
Eyes that experience acute attacks of angle closure are anatomically different than normal—they have shorter axial lengths, shallower anterior chambers, thicker and relatively anteriorly positioned lenses, and flatter corneas25—but it appears that they also may be physiologically different than normal.24 In a case-control study by Friedman et al, it was found that eyes with acute attacks of angle closure responded differently to provoking stimuli (going from light to dark and pilocarpine). The patients with previous acute angle closure (AAC) had anterior chambers that became 50% narrower than in control eyes, and when treated with pilocarpine their angles opened up 50% less despite the same baseline biometry as the normal eyes. It has also been noted that in PAC eyes, there is a tendency for the lens and iris to move forward during surgery. This can occur even in the presence of a patent iridotomy and with the patient in a supine position,26 suggesting that there is a physiologic tendency for the anterior chamber to shallow apart from high iris–lens resistance.24 Previous studies of central anterior chamber depth before and after prophylactic iridotomy showed no significant deepening of the anterior chamber (AC) or at most 50 microns of increased depth.15,27,28 One study demonstrated anterior chamber depth to be much narrower immediately after resolution of an acute attack than 4 months later when the attack eye’s AC depth was similar to the contralateral eye.24 Quigley hypothesized that there is a tendency for the lens to move forward in acute attacks and potentially even in chronic forms of angle closure. One cause of forward lens movement in his theory may be expansion of the choroid. One study showed that choroidal expansion was present in several PAC eyes studied shortly after acute attacks, and while it is possible that the expansion was unrelated or a result of pressure-lowering treatments, it is also possible that the expansion preceded the attack.29,30 Increases in choroidal volume can move the lens forward dramatically.29 Until an accurate measurement system is developed for this parameter, this will remain a theory.
It is also recognized that pupillary block does not satisfactorily explain all cases of angle closure. In Chinese people, only 38% of angle closure is attributable solely to pupillary block. Wang et al.31 have proposed to classify PACG in Chinese eyes into three types: angle closure caused by pupillary block, angle closure caused by nonpupillary block, and angle closure caused by a combination of these two mechanisms. It is believed that most PACG in Chinese is caused by multimechanism PACG. In Chinese eyes, there is also a high prevalence of creeping angle closure that is not caused by pupillary block.9 The position of the iris insertion and ciliary body are thought to predispose to creeping angle closure. In a study analyzing the anterior chamber angle of blacks, whites, and Far East Asians using the Spaeth gonioscopic grading system, the iris was found to join the scleral wall most anteriorly in Asians and most posteriorly in whites, despite the fact that there was no significant difference in the angle width of these three groups. In addition, this racial difference was more apparent with indentation gonioscopy.32 There may be a tendency for the lens to move forward in asymptomatic chronic angle closure; however, the exact pathophysiology in these chronic forms of angle closure is yet to be exactly described.
It has been assumed that if angle closure continues despite a patent iridotomy, which eliminates pupillary block, then there is another mechanism of angle closure at play. In Chinese eyes, Hung and Chou.33 reported that the dark-prone provocation test was positive in 60% of Chinese eyes postiridectomy, compared with being positive in only 12.5% of normal eyes. Plateau iris and plateau iris syndrome are cases in which angle closure can continue despite patent iridotomy (Fig. 53.5), depending on the height of the plateau and the width between the peripheral iris and trabecular meshwork.34,35,36 Prominent last iris roll is another situation in which iridotomy may not be completely effective. This term, sometimes attributed to Fuchs, refers to an anterior nonpupillary block entity in which there is a very thick iris that is thrown into prominent circumferential folds peripherally. These folds in eyes with a thick iris can occupy a larger proportion of the anterior chamber angle than in an eye with a thin iris. With dilation of these irides, the folds become more pronounced and may even contact the trabecular meshwork.7 Additional mechanisms may be at play in the progression of angle closure after iridotomy. Valsalva maneuvers can lead to significant anterior segment shallowing, as evidenced by ultrasound biomicroscopy testing.37 A patent iridotomy may not prevent iridotrabecular apposition during a Valsalva, and it has been suggested that this may be one reason for progression from PACS to PAC and PACG despite a patent iridotomy.38
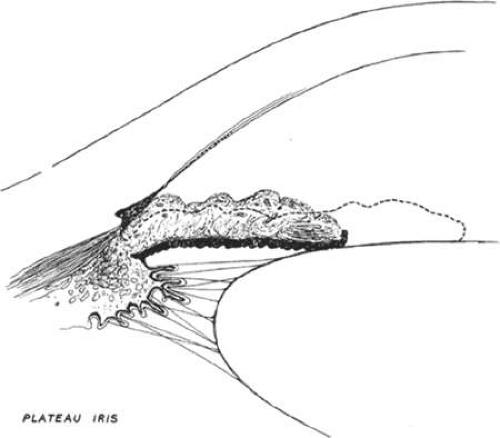 Figure. 5. Plateau iris configuration. The anterior chamber is deep axially and the iris plan is flat. The angle is open but is narrow when the pupil is small (dotted line) and closed when the pupil is dilated. (Kolker AE, Hetherington J Jr: Becker and Shaffer’s Diagnosis and Therapy of the Glaucoma, p 198. St. Louis, CV Mosby, 1970) |
Epidemiology
Prevalence
There are considerable differences in the prevalence of primary angle closure and primary angle-closure glaucoma among different racial and ethnic groups. There are also significant differences in the mechanism of angle closure between different groups.
European Descent
In populations of European descent, PACG has a lower prevalence than primary open-angle glaucoma (POAG). The prevalence of PAC and PACG in European-derived people is between 0.04% and 0.6%.39,40,41,42,43,44 Specifically, in the Beaver Dam Study of Wisconsin prevalence was 0.04%; in Melbourne, Australia 0.06%; in Wales, UK 0.09%; in Baltimore 0.4%; and in Northern Italy, within a relatively isolated population, 0.6%. The predominant mechanism of angle closure in these populations is pupillary block.
Inuit
The Inuit people of Alaska, Canada, and Greenland suffer the highest rates of PACG of any population,45,46 and the angle closure is caused by pupillary block. With Koeppe lens gonioscopy, a population survey of Greenland Inuit found that 88% of prevalent glaucoma was caused by angle closure.47 Among Greenland Inuit aged 40 years and older, 5.1% of women and 1.6% of men had PACG.48 In Alaska, 2.65% of Inuit Eskimos older than 40 years of age have PACG and 17% older than 50 years were found to have occludable angles.46
Pupillary-block glaucoma is a serious disease that leads to a high rate of blindness that is often bilateral. In a survey of blindness in Greenland, 64% of all Inuit blindness was caused by glaucoma.49 Of the registered blind with glaucoma in 1972, 93% had PACG and many were blind to the level of no light perception. Since the institution of biometric screening, followed by gonioscopy and prophylactic iridotomy where indicated, the proportion of PACG blindness in Greenland Inuit at risk has been reduced from 64% to 9% over a period of 37 years.49
Mean anterior chamber depth (ACD) in Inuit eyes was found to be shallower than similar measurements in Caucasians, after excluding known cases of PACG and their families.50 In known cases of ACG, the average ACD was 1.8 mm. Those at greatest risk of PACG were also found to have smaller corneal diameters, axial lengths, and anterior chamber volumes.25 Alsbirk.45 postulated that the extreme differences in ocular biometry in the Inuit may be an evolutionary adaptation to the harsh environment to which their eyes were exposed after they migrated from Asia (specifically the area of Mongolia) more than 9,000 years ago. The Inuit are believed to be descendants of East Asian people.51
East Asia
In the next few decades, it is predicted that nearly half of all worldwide cases of glaucoma will occur in Asia.1 This prediction is rooted in data from population-based studies used in prevalence models combined with UN world population projections. Asians will represent 47% of those with glaucoma and 87% of those with PACG by 2020. Most Asian people suffering from angle-closure glaucoma experience no symptoms, as chronic primary angle-closure glaucoma is much more prevalent in these populations.52,53
Earlier prevalence studies of glaucoma reported an extremely high rate of PACG compared to POAG in China. It has been recognized that these studies used inconsistent definitions of PACG and less than optimal methods of examination, and probably grossly underestimated the number of POAG cases.54,55 Since 1989, there have been data on PAC and PACG in Asia of good methodologic quality, using the newer definitions of PAC and PACG established by the International Society of Geographical and Epidemiological Ophthalmology.
Detailed epidemiologic studies show that Mongolians have dramatically higher rates of PACG than Caucasians.52 Primary angle-closure glaucoma is the predominant form of glaucoma in Mongolia, and its prevalence is almost three times higher than that of POAG in this population.52 Narrow angles or PACS were found with a prevalence of 6.4%, whereas PAC and PACG were found with a prevalence of 2.0% and 0.8%, respectively. Interestingly, 91% of all glaucoma cases were previously undiagnosed. Pupillary block is believed to account for at least 90% of PACG cases in Mongolia.56
In Singapore, there is a mixed ethnic population. Three quarters of the population is Chinese and the remainder is largely Malay and Indian. In a study isolating the Chinese population 40 years and older, the age-standardized prevalence of glaucoma was 3.2%.57 The age and sex-standardized prevalence rates of occludable angles were similar to those found in Mongolia: 6.3% for all occludable angles of PACS, 2.2% for PAC, and 0.8% for PACG. This study found POAG to be 1.5 times more common than PACG.57 Chronic PACG accounted for 45% of the total glaucoma cases in Singapore, and most were found to be asymptomatic. Although PACG occurred in only 1% of the general population, its prevalence increased to 7% to 8% of those 60 years and older. Being of Chinese ethnicity compared to Malay or Indian was associated with a relative risk of 2.8. Being female was associated with a relative risk of 2.4, and age greater than 60 had a relative risk of 9.1. In Singapore, only 21% of cases of PACG had not been previously diagnosed.57
On mainland China, the urban population of Liwan District, Guangzhou, was studied between 2003 and 2004 for the prevalence of glaucoma.58 The crude prevalence of PACG and POAG was 2.1% and 1.5%, respectively, and age- and sex-standardized prevalence rates were 1.8% and 1.3%. Persons with PACS accounted for 10.2% of participants, PAC 2.4%, and PACG 1.5%. The prevalence of narrow angles was almost twice as high in women (12.5%) as in men (7.1%). The prevalence of narrow angles increased with age, from 3.7% in the sixth decade to 20.0% in the ninth decade. The prevalence of PAC and PACG also increased with age and female gender. Of the cases with PACG, 42.9% were blind in at least one eye (best-corrected visual acuity [BCVA] 3/60 or worse) compared to 17.2% of those with POAG.
The data from China is similar to the Singaporean data in that POAG affects more people than PACG, but that PACG causes more severe disease. In the Beijing Eye Study (a population-based study on subjects 40 years or older in northern China carried out in four urban communities and in three rural communities), glaucomatous optic neuropathy was detected in 3.1% of subjects, with 2.2% being attributed to open-angle glaucoma and 0.9% to angle-closure glaucoma.59 The prevalence of PACS and PAC was not reported in this survey.
In Japan, the situation with PACG is different. The Japanese population is a relatively homogeneous population. A nationwide Japanese glaucoma survey in 1988 and 1989 reported a prevalence of 2.62% for POAG and 0.34% for PACG.60 In a more current survey, the prevalence rates of all glaucoma and glaucoma suspect were estimated to be 5% and 7.5%, respectively. The estimated prevalence of PACG was 0.6%, much lower than in other Asian groups.61
There are few data on Korean glaucoma prevalence in the Western literature. According to a hospital-based epidemiology study presented at the Korean Glaucoma Society meeting in November 2001, the overall prevalence of glaucoma was 1.9%. One third of cases were owing to POAG (0.65% prevalence), 22% to normal tension glaucoma (NTG) (0.42% prevalence), and 15% to PACG (0.29% prevalence).62 Future population-based surveys in Korea should provide more representative data.
Southeast Asia
In Myanmar (formerly Burma), the prevalence of PACG is about equal to POAG (1.25:1).63 This population has a lower ratio of PACG to POAG compared to the Mongolian population but a higher rate compared to Chinese and Indian eyes. Overall, prevalence of PACG was 2.5% and POAG 2.0%. Acute angle closure and chronic angle closure were almost equally found in this population. Primary angle-closure glaucoma accounted for 84% of all eyes blind from glaucoma. As in the other studies, prevalence increased with age. The prevalence of occludable angles in at least one eye was 5.7% and of PAC 1.5%.64
A similar prevalence of occludable angles was found in Vietnamese eyes. Since the Vietnam War, more than 1.4 million East Asian Indochinese refugees have settled in the United States.65 Nguyen et al.66 reported that Vietnamese American patients had a much higher prevalence of narrow angles and a greater risk of angle-closure glaucoma than white patients. Of 482 patients examined, 8.5% had a gonioscopic Shaeffer grade between 0 and 1 and were considered to be at high risk for occlusion.
The prevalence of POAG and PACG among Thai people appears to be different from that in Burmese and Vietnamese people. In 701 subjects aged 50 years or older examined in a population-based survey in the Rom Klao district of Bangkok, prevalence of POAG and PACG was 2.3% and 0.9%, respectively.67 Although the prevalence of PACG was lower in this population sample, the prevalence of occludable angles (14%) was higher than in the Burmese and Vietnamese.
As mentioned previously, the Singaporean population consists of a mixture of Chinese, Malay, and Indian people. In a prospective, island-wide incidence study, Chinese ethnicity carried a significantly higher risk of symptomatic PAC compared with non-Chinese Singaporeans (relative risk 2.8).68 The hospital discharge rates (per 100,000 per year) for PACG among Malays and Indians in Singapore were 6.0 and 6.3, respectively, and were very similar to the rate of symptomatic PAC (7.0/100,000/year) reported among Thai people.69
South Asia
It has been widely believed that PACG is more common on the Indian subcontinent than among European people,70 but population surveys provide conflicting data depending on which region of the country is studied. In Vellore, Southern India, a study that did not use the standardized ISGEO classification to define glaucoma, found the prevalence of PACG to be 4.3% among people aged 30 to 60 years. All detected cases of PACG were of the chronic type, making PACG about five times as common as POAG.71 Another study, in the Southern Indian state of Tamil Nadu on a rural population aged 40 and older, reported sex- and age-adjusted prevalence rates of 6.10% for PACS, 0.66% for PAC, and 0.82% for PACG. Most cases were asymptomatic, suggesting chronic angle closure.72 In the Aravind Eye Study, prevalence of POAG and PACG was 1.7% and 0.5%, respectively, among subjects 40 years and older living in the rural region of Southern India.73 In the Southern urban city of Hyderabad, the prevalence of PACG (1.08%) was about half that for POAG (2.56%) in subjects 40 years of age or older.74,75 Occludable angles without glaucoma (i.e., PACS and PAC) and PACG were found with a prevalence of 2.21% and 1.08%, respectively, in participants 40 years of age or older, but the prevalence of these two conditions considered together increased significantly with age. Only a third of PACG had been previously diagnosed, most cases (83%) had the chronic form of the disease, and PACG was responsible for blindness in at least one eye of 42% of cases.75 In contrast, in West Bengal the crude ratio of POAG to PACG favored a diagnosis of POAG 10:1, with a rate of PACG of 0.23% in those 50 and older. What can be gleaned from these studies is that PACG is probably more common in India than in European people, but that the prevalence may vary depending on what part of the country one is from. As in the rest of Asia, it has a tendency to be asymptomatic.
Among people aged 40 years and older examined in a population-based survey in Dhaka, Bangladesh, the prevalence of definite and probable glaucoma was 3.1%: POAG 2.5% and PACG 0.4%. Primary open-angle glaucoma accounted for 75% all glaucoma cases. This population has a pyramidal age structure in which 40% of people were in the 40- to 49-year age group.76
Africa
Africa is home to a diverse population, and there are few population-based studies using the ISGEO classification. Three studies were performed in South Africa. In a study of black residents in Temba, North West Province, PACG was found to affect the population much less frequently than POAG. Age- and gender-adjusted prevalence rates were 0.5% and 2.9%, respectively.77 In a South African Zulu population, PACG also accounted for a very low percentage of the glaucoma found.78 In a mixed ethnic population near Cape Town, whose ancestors included Southeast Asians, indigenous Africans, and to a lesser extent Europeans, the prevalence of PACG was much higher at 2.3%, compared to a 1.5% prevalence of POAG. However, in this study glaucoma was diagnosed based on an IOP greater than 21 mm Hg or a visual field defect with an occludable angle, and this may have caused an overestimation of PACG prevalence.79 In another study in Tanzania, the prevalence of PACG was 0.59% compared to 3.1% for POAG. In the Tanzanian study, only cases meeting certain criteria plus a 20% random sample underwent gonioscopy.80 From the limited population-based studies in Africa, we can conclude that PACG is not the predominant form of glaucoma on this continent.
South America
In South America, there is only one study of glaucoma prevalence to date with the ISGEO classification system. This study screened the residents 40 years and older in Piraquara City in the south of Brazil. Participants self-reported their race as white (71.5%), mixed black-white (18.2%), black 5.9%, Asian/native Indian (0.2%), and undetermined (4.2%). Gonioscopy was not part of the screening examination so rates of PACS and PAC are unknown; however, gonioscopy was performed on confirmed cases of glaucoma. Crude prevalence of PACG in this population was 0.7% with equal prevalence in white and nonwhite participants. The white Brazilians had a higher rate of PACG than most European-derived populations.81
Incidence
The incidence of acute or symptomatic angle closure has been reported in several countries: Finland,82 Croatia,83,84 United States of America,85 United Kingdom,86 Japan,87 Israel,88 Thailand,87 Singapore,68,69 and Hong Kong.89 Increasing age and female gender are risk factors for acute angle closure in all of these studies. In Finland, 74% of cases were accounted for by women. In Israel, cases in women outnumbered those in men 2:1. It is also important to note the ethnic trends in incidence. East Asian people (except Japanese and Koreans) tend to have the highest rates of acute angle closure followed by South and Southeast Asians (e.g., Indian, Thai, and Malay people). Age and gender standardized incidence varies from 2.8 cases per 100,000 population per year in Croatia to 15.5 cases per 100,000 per year among Chinese Singaporeans.90
Most of the reports of incidence are retrospective case series, as attacks of angle closure are relatively infrequent events. However, two of the studies cited above were prospective studies collecting cases over a 1- or 2-year period. In Hong Kong Chinese, the incidence rate was 10.4/100,000 per year.89 In Singapore, the overall incidence rate was 12.2./100,000 per year, with the highest rate in Chinese Singaporeans.68
In another study, the incidence of acute angle closure was carried out in Greenland Inuit. Of 69 patients who had gonioscopy at baseline, 20 were considered to have occludable angles. At a 10-year follow-up examination, 7 of 20 (35%) had developed PACG. Of the 49 patients with nonoccludable angles at baseline, only 4/49 (8%) were diagnosed with PACG at follow-up. The patients in this study were originally selected based on a van Herrick score of 2 or less with a central anterior chamber depth (ACD) by pachymetry less than or equal to 2.7 mm (including cornea).91
In a prospective multicenter study conducted in the United States, 129 patients who were judged to be at risk for developing angle-closure glaucoma according to a baseline examination were followed up with no treatment. (Baseline examination included gonioscopy, refraction, anterior chamber pachymetry, ultrasound biometry, and an angle-closure provocative test.) With a mean follow-up of 2.7 years (maximum follow-up 6 years), 25 patients (19.4%) developed angle closure in at least one eye, but in two thirds of these patients (17 of the 25 patients, 68%), the angle closure was nonacute (that is, there were no clinical signs or symptoms and no increase in IOP). By using a Kaplan-Meier life table, the risk of developing an acute angle closure during the total follow-up period of 7 years approaches 30%.92
Two publications from Vellore, Southern India, provide insight into the natural history of angle closure among Indians. Among people with narrow drainage angles/PACS, the 5-year incidence of PAC was 22% (95% confidence interval [CI]: 9.8, 34.2).93 In a second report, people found to have established angle closure at the time of the population survey were advised to undergo laser iridotomy. Eight of 28 people examined with PAC (28.6%, 95% CI: 12, 45) progressed to PACG over 5 years. One of nine (11.1%) who agreed to recommended laser peripheral iridotomy (LPI) progressed, compared to 7 of 19 (36.8%) who refused LPI.94
Risk Factors
Many factors have been identified that increase the risk of PACG (Table 53.3). They include demographic factors, anatomic features of the eye, and environmental factors. As described in the epidemiology section of this chapter, there is clearly a pattern of increased risk with ethnicity—Inuit having the highest risk, followed by East Asians (primarily Chinese), and Southeast Asians. Female gender is another predisposing risk for both acute angle-closure attacks and angle-closure glaucoma across all ethnicities. Women were found to carry at least twice the risk for the disease compared to men. They have a higher prevalence of narrow drainage angles, PAC, and PACG. A statistical model estimating the total number of people affected by glaucoma suggests that 70% of those affected by angle closure worldwide are women.1 Increasing age is another demographic factor related to PAC and PACG. Angle closure before the age of 40 years is rare but increases with each decade of life. For example, in Southern Croatia, the relative risk for acute angle closure in persons older than 69 years of age is 28 compared to those in the 30- to 39-year age group.84 In Singapore, the relative risk of acute angle closure in persons 60 years of age or older is 9.1 compared to those in their thirties.68 The prevalence of narrow angles in China was found to increase from 3.7% in the sixth decade to 20.0% in the ninth decade.58
Table 53.3 Risk Factors for Primary Angle Closure | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
|
Compared with normal eyes, eyes with PACS, PAC, and PACG have smaller anterior chamber depth (ACD), a thicker lens, a more anterior lens position, and a shorter axial length.27,95,96,97,98,99,100,101,102,103,104,105 Studies using ultrasound biomicroscopy also show lower values for these parameters in PACG than in normals.98,106,107,108 These differences between PAC eyes and normals have been found across different ethnic groups. In a study of Chinese eyes, axial length was shorter in those eyes affected by symptomatic acute angle closure than in those affected by asymptomatic angle closure. Both the symptomatic and asymptomatic eyes had shorter axial lengths than the normal controls.102 In India, in a study comparing people with acute, subacute, and chronic angle closure, it was found that all groups with angle closure had shorter axial lengths than age- and gender-matched controls.97
The most important biometric feature predisposing to angle closure is a shallow anterior chamber. The mean depth of eyes with angle closure has been reported to be 1.8 mm, which is 1.0 mm shallower than the mean value of normal eyes.109 Relative pupillary block is rare when ACD exceeds 2.5 mm.10 Limbal ACD is another important risk factor. Patients with PACG were 19 times as likely to have a shallower limbal ACD (point estimate 25%; 95% confidence interval, 8.3%–45.2%) than normals.110
The risk of angle closure at various ACDs was studied in a European population, and the risk was found to increase as ACD decreased.111 The same association has been documented in the Inuit, Mongolian, and Chinese populations, and in Indian and Australian clinics.45,97,112,113,114 Anterior chamber depth correlates with demographic factors; namely, female gender, increasing age, and certain ethnicities are associated with shallower anterior chamber depths.105,115,116,117 Cross-sectional data suggest that ACD decreases with age. Age-related changes in ACD appear to be more pronounced in women than in men,45,116 and greater differences in mean angle width between younger and older people have been reported among men and women.105,117
Anterior chamber depths in persons of European ancestry, a population with a relatively low prevalence of PACG, are greater than those of East Asian people or the Inuit, who have the highest prevalence of PACG and the shallowest ACD of all populations.118 However, there is one study that contradicts these data. In a study comparing Taiwanese Chinese and white and black residents of Baltimore, Maryland, no significant difference was found for ACD and axial length among these three groups, but whites in this study had more hyperopia and Chinese had a significantly smaller corneal radius of curvature. It is argued that the difference between the prevalence of hyperopia among Chinese and Caucasians is unlikely to explain the increased amount of PACG among Chinese. However, a smaller radium of corneal curvature may imply a more crowded anterior chamber and angle that explains the excess risk of PACG among Chinese. The authors also suggested that additional factors other than anterior chamber depth might be responsible for the interracial predisposition toward angle closure.119
The prevalence of PAS is also related to shallower chamber depth, as seen in studies from Mongolia and Singapore. In addition, ACD is inversely related to the prevalence of glaucomatous optic neuropathy (GON) in both populations. People with an ACD less than 2.00 mm were between 5 and 23 times more likely to have glaucomatous optic neuropathy in Singapore and Mongolia, respectively. The different rates of PAS were strikingly different between the two ethnic groups. Mongolians had almost no PAS until ACD was less than 2.5 mm, whereas relatively deep axial anterior chambers were seen in Singaporeans with PAS. The increase in PAS with shallowing of the anterior chamber was much less pronounced in Singaporeans than in Mongolians.90,120
Anterior chamber depth depends on the position of the anterior lens surface and is determined by the thickness and position of the lens inside the eye. In his own Australian clinic population, Lowe.121 found that the main reason for shallower anterior chambers in PAC patients was a more anterior lens position and a thicker lens. Sun et al.102 reported similar findings in a Chinese clinic. Another study of Chinese people found that lens thickness was the major determinant of a shallow AC, with lens position differing by only 4% between PAC and normal eyes.110
It has been noted for some time that hyperopia is a risk factor for PACG, and many angle-closure patients are hyperopic; however the association is not invariable.122 In general, the anterior chamber depth and volume is smaller in hyperopes.123 In Australia, a 5.5% rate of myopia, 33% rate of emmetropia, and 61.4% rate of hyperopia were found in a study of PACG eyes.113 In Singapore, only 23% of people graded with PAC and 33% of those with PAS had myopic refractions.122 In Philadelphia, a retrospective review of 322 PAC eyes revealed only 6 cases in myopic eyes—2% of cases of PAC had myopia of -5 diopters or more.124 In a study of 18,000 myopes, PAC was found in 0.1%.125
Environmental factors have also been studied as risk factors for symptomatic PAC in susceptible individuals. The incidence of PAC has been reported to be highest at times of extreme temperatures.68,82,83,84,88,126,127 It has been suggested that unpleasant weather encourages people to stay indoors so that they spend more time in dim lighting conditions.122 An association between incidence of symptomatic PAC and sunspots has also been described.68,128 Sunspots are regions on the sun’s surface of lower temperature associated with strong magnetic activity. Sunspots can affect the earth’s upper atmosphere. In a nationwide, population-based study to investigate the dependence of PACG hospital admission rates on meteorologic conditions in Taiwan, PACG admission rates were significantly higher in March and at times of increased relative humidity, but no significant relationship existed with temperature, rainfall, barometric pressure, or hours of sunshine.129
Family history is another risk factor for angle closure and PACG. The risk of developing PACG is 3.5 times higher in first-degree relatives of affected Inuit patients, and 6 times higher in family members of affected Chinese patients.31 The risk appears to be incurred because of the inheritance of a small, crowded anterior chamber. Shallow anterior chambers are more commonly observed in close relatives of patients with angle-closure glaucoma.111,130 In Eskimos, a heritability of 70% was found for ACD, indicating that two thirds of the age- and sex-independent variation in ACD was due to genetics.131 A more forward and thicker lens appear to be determined genetically as well.10
Gonioscopy and Angle Grading Systems
Examination of the angle, called gonioscopy, is vital to diagnosing narrow angles and angle closure. A successful examination of the angle is dependent on the skill and experience of the examiner. It can be difficult to evaluate some narrow or closed angles (Fig. 53.6), whereas it is relatively easy to identify wide open angles (Fig. 53.7). In Asian eyes, some authors have commented that it is difficult to describe angles using the established nomenclature systems that were developed based on the examination of primarily Caucasian eyes.12
 Figure 53.6. This angle is closed. At the arrow, one sees the edge of the peripheral iris. The ciliary band, scleral spur, and trabecular meshwork are covered by peripheral iris, and one sees only cornea anterior to it. This could be reversible appositional closure of the angle or permanent synechial closure. |
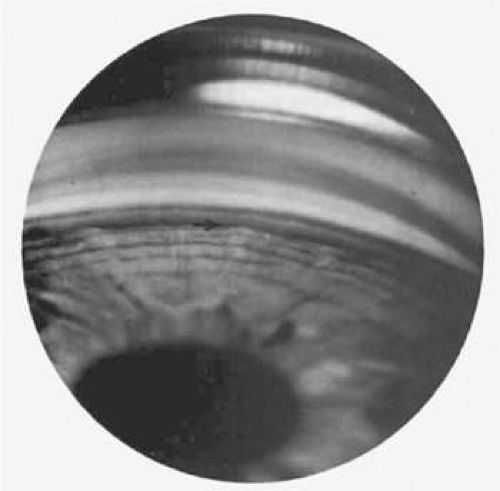 Figure. 7. In this goniophotograph, the angle is moderately wide open. As one looks just anterior to the edge of the peripheral iris (arrow), one sees the dark ciliary band, white scleral spur, and trabecular meshwork, which is moderately dark and pigmented in this eye. Schwalbe’s line anterior to the trabecular meshwork is not visible in this photo. Such an angle is much too wide to be susceptible to primary angle-closure glaucoma. |
When performing gonioscopy, it is vital that the examination is performed under dimly lit conditions. The slit-beam should be a small rectangle or square only as bright as necessary to view angle structures, with care not to allow the light to enter the pupil and activate the light reflex. Illumination used for examination can constrict the pupil, pull iris out of the angle, and alter gonioscopic findings. In a study comparing gonioscopy under dark room conditions to ultrasound biomicroscopy (UBM), all but one of eighteen subjects (94%) with gonioscopic findings of appositional angle closure were found to have iridotrabecular apposition by UBM. When the room lights were turned on, only 56% of the subjects had a closed angle by UBM, highlighting how dramatically the exam can be changed by illumination. It is estimated that light will open an appositionally closed angle 38% of the time.132,133
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


