Chapter 13 Preseptal and orbital cellulitis
Classification
Infective orbital cellulitis and its complications can be classified into five types which are not mutually exclusive and do not necessarily progress in that order1 (Table 13.1):
Table 13.1 Classification of orbital cellulitis
| Stage | Signs and symptoms | CT findings |
|---|---|---|
| Preseptal cellulitis | Eyelid swelling, occasional fever | If performed, sinusitis may be present |
| Orbital cellulitis | Proptosis, decreased painful eye movements, chemosis | Sinusitis, mild soft tissue changes in the orbit |
| Subperiosteal abscess | Signs of orbital cellulitis, systemic involvement | Subperiosteal abscess, globe displacement, soft tissue changes in the orbit |
| Orbital abscess | Signs of orbital cellulitis, systemic involvement, ophthalmoplegia, visual loss | Orbital collection of pus with marked soft tissue changes of the fat and muscles |
| Intracranial complication | Signs of orbital or rarely preseptal cellulitis, marked proptosis, cranial nerve palsies (III, IV, V, VI) | Intracranial changes: cavernous sinus thrombosis, extradural abscess, meningitis, and osteomyelitis |
Modified from Uzcategui N, Warman R, Smith A, et al. Clinical practice guidelines for the management of orbital cellulitis. J Pediatr Ophthalmol Strabismus 1998; 35: 73–9. © 1998 Slack Inc.
Preseptal cellulitis
Preseptal cellulitis is five times more common than orbital cellulitis, especially in children under the age of 5 years.2,3 It is often secondary to lid and cutaneous infections – styes, impetigo, erysipelas, herpes simplex, varicella, or dacryocystitis (Figs 13.1, 13.2, and 13.3). It is also associated with upper respiratory tract infections, uncomplicated sinusitis (Fig. 13.4), or lid trauma.






Infective preseptal cellulitis must be distinguished from other causes of lid edema such as adenoviral keratoconjunctivitis, atopic conjunctivitis, or, rarely, Kawasaki’s disease.4 In one series, 16% of children referred with preseptal cellulitis were found to have adenoviral keratoconjunctivitis.5
Clinical assessment
Examination
It can be difficult to differentiate between preseptal and orbital cellulitis and the diagnosis may change from preseptal to orbital cellulitis if orbital signs become more obvious, clinically or by imaging.6
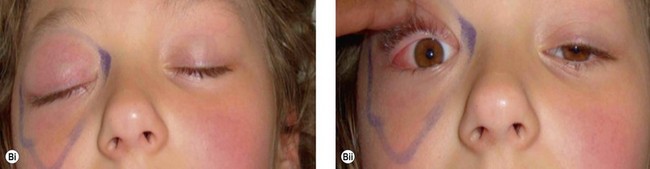
The clinical picture varies with the organism involved. In staphylococcal infections there is a purulent discharge, while Haemophilus infection leads to a non-purulent cellulitis with a characteristic bluish-purple discoloration of the eyelid with irritability, raised temperature, and otitis media (Fig. 13.5). In streptococcal infection there is usually a sharply demarcated red area of induration,7 heat, and marked tenderness (Fig. 13.6A,B). Preseptal cellulitis may be complicated by meningitis, particularly if the infection is due to Haemophilus influenzae type B.8


Management
Children with mild to moderate preseptal cellulitis can be managed in the same way as uncomplicated sinusitis on an outpatient basis with oral broad spectrum antibiotics or as an inpatient with intravenous antibiotics, if more severe (Table 13.2).9,10
Table 13.2 Initial antibiotic treatment of preseptal and orbital cellulitis
| Preseptal cellulitis | Associated with upper respiratory tract infection |
| Cefuroxime 100–150 mg/kg per day or amoxicillin-clavulanate (augmentin) or ampicillin 50–100 mg/kg per day and chloramphenicol 75–100 mg/kg per day (IV in divided doses) | |
| Orbital cellulitis | Ceftazidime 100–150 mg/kg per day or cefotaxime 100–150 mg/kg per day or oxacillin or nafcillin 150–200 mg/kg per day (in divided doses) |
| Ceftriaxone: 80 mg/kg (max 4 g/day) | |
| Flucloxacillin: 50 mg/kg qds IV (max 2 g/dose) | |
| Co-Amoxiclav: 30 mg/kg tds (max 1.2 g/dose) | |
| Metronidazole: 7.5 mg/kg tds (max 500 mg/dose) | |
| Vancomycin should be considered in resistant cases | |
| Clindamycin should be added in necrotizing fasciitis |
Note: You should consult your own pharmacy for correct doses.
The exact dose will vary with age and severity of infection.
There may be local variations in pathogens and antibiotic resistance.
A CT scan to assess orbital, sinus, and brain involvement is indicated when lid swelling prevents an adequate examination of the globe.11
Lid trauma may result in suppurative cellulitis, when the causative agent is Staphylococcus aureus or a beta-hemolytic Streptococcus. It is usually sufficient to culture the wound discharge as there is rarely any bacteremia; blood cultures are usually negative.12 Parenteral antibiotics are administered and tetanus prophylaxis is provided, if appropriate. If the skin has been penetrated by organic material or animal bites, antibiotics should be included coverage for anerobic organisms.
Rarely, beta-hemolytic Streptococcus may cause necrotizing fasciitis. It is characterized by a rapidly progressive tense and shiny cellulitis with excessive edema and poorly demarcated borders with a violaceous skin discoloration. Necrosis develops and streptococcal toxic shock syndrome is common (Fig. 13.7). Treatment is with immediate hospitalization with a multidisciplinary team implementing resuscitation and medical support with immediate high-dose intravenous antibiotics including a penicillin or third-generation cephalosporin and clindamycin. Surgical debridement should be considered if there is not a clear response to medical treatment.13,14




