(1)
Department of Ophthalmology, St. Thomas’ Hospital, London, UK
Abstract
Posterior vitreous detachment is the commonest and most important event that occurs in the vitreous. As the vitreous ages, the normal architectural features apparent in childhood gradually disappear as degeneration causes syneresis, lacuna (cavity) formation and collapse of the vitreous gel. The collagen fibrils disintegrate and aggregate giving rise to symptomatic floaters (Bishop et al. 2004; Akiba et al. 1993). There is loss of sodium hyaluronate (Larsson and Osterlin 1985) and an increase in vitreous mobility with age (Walton et al. 2002). Most individuals will develop posterior vitreous detachment (separation of the posterior hyaloid membrane from the internal limiting membrane), without symptoms or pathological sequelae, usually between the ages of 40–80 years. 27 % of patients in their seventh decade and 63 % in their eighth decade have PVD (Foos and Wheeler 1982). This may occur at a younger age (less than 40 years old) in myopia, diabetes, retinal vascular disorders, trauma and retinitis pigmentosa (Hikichi et al. 1995b, c; Sebag 1993; Morita et al. 1995; Yonemoto et al. 1994; Akiba 1993). Presentation with symptomatic PVD (flashes and floaters) may be more common in females than males and in myopia (Chuo et al. 2006). The detached posterior hyaloid membrane becomes wrinkled and usually separates completely from the retina up to the posterior border of the vitreous base (or up to the posterior aspect of any other vitreoretinal adhesions, which may be present). Acute ischaemic events such as retinal vein occlusion may induce PVD with an increased prevalence of PVD 1 year after onset of the vein occlusion (Kado et al. 1990). No racial differences in the rates of PVD have been found between whites and oriental peoples with disagreement whether black races have less PVD (Hikichi et al. 1995a; Weiss and Tasman 1978; Foos et al. 1983). The fellow eye has evidence of PVD in 90 % in 3 years (Hikichi and Yoshida 2004) with 11 % developing symptomatic PVD in the other eye in 2 years often demonstrating similar problems to the first eye such as tears or vitreous haemorrhage (Novak and Welch 1984).
4.1 Introduction
Posterior vitreous detachment is the commonest and most important event that occurs in the vitreous. As the vitreous ages, the normal architectural features apparent in childhood gradually disappear as degeneration causes syneresis, lacuna (cavity) formation and collapse of the vitreous gel. The collagen fibrils disintegrate and aggregate giving rise to symptomatic floaters (Bishop et al. 2004; Akiba et al. 1993). There is loss of sodium hyaluronate (Larsson and Osterlin 1985) and an increase in vitreous mobility with age (Walton et al. 2002). Most individuals will develop posterior vitreous detachment (separation of the posterior hyaloid membrane from the internal limiting membrane), without symptoms or pathological sequelae, usually between the ages of 40–80 years. 27 % of patients in their seventh decade and 63 % in their eighth decade have PVD (Foos and Wheeler 1982). This may occur at a younger age (less than 40 years old) in myopia, diabetes, retinal vascular disorders, trauma and retinitis pigmentosa (Hikichi et al. 1995b, c; Sebag 1993; Morita et al. 1995; Yonemoto et al. 1994; Akiba 1993). Presentation with symptomatic PVD (flashes and floaters) may be more common in females than males and in myopia (Chuo et al. 2006). The detached posterior hyaloid membrane becomes wrinkled and usually separates completely from the retina up to the posterior border of the vitreous base (or up to the posterior aspect of any other vitreoretinal adhesions, which may be present). Acute ischaemic events such as retinal vein occlusion may induce PVD with an increased prevalence of PVD 1 year after onset of the vein occlusion (Kado et al. 1990). No racial differences in the rates of PVD have been found between whites and oriental peoples with disagreement whether black races have less PVD (Hikichi et al. 1995a; Weiss and Tasman 1978; Foos et al. 1983). The fellow eye has evidence of PVD in 90 % in 3 years (Hikichi and Yoshida 2004) with 11 % developing symptomatic PVD in the other eye in 2 years often demonstrating similar problems to the first eye such as tears or vitreous haemorrhage (Novak and Welch 1984).
PVD is the primary process in the development of most rhegmatogenous retinal detachments because of its role in retinal tear formation. It is also implicated in common macular disorders, such as macular pucker and macular hole formation. Separation of the gel may also tear blood vessels in the retina or in neovascular complexes causing haemorrhaging into the vitreous cavity. The importance of PVD has led many investigators to try methods for the artificial inducement of PVD (Unal and Peyman 2000; Hesse et al. 2000; Kakehashi et al. 1994; Hikichi et al. 1999; Verstraeten et al. 1993; Harooni et al. 1998; Tezel et al. 1998; Kang et al. 1995) such as plasmin injection as a proteolytic acting on the vitreoretinal interface.
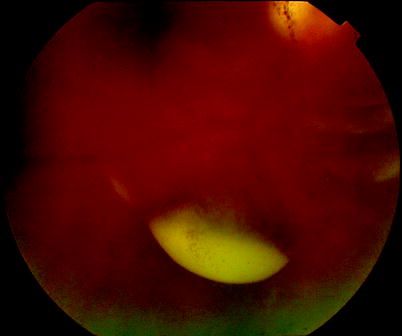
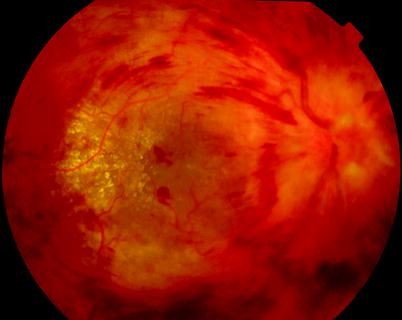
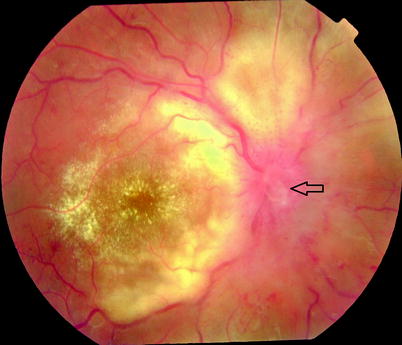
Fig. 4.1
Syneresis of the vitreous causes lacuna formation; in this figure, the presence of a lacuna is demonstrated by the fluid level of old altered blood which is trapped inside a lacuna cavity
Fig. 4.2
A 13-year-old girl with CRVO in whom the onset was associated with a bout of diarrhoea on ski trip and a short-haul plane journey. She had a familial cholesterolaemia
Fig. 4.3
At 2.5 months, there is a Weiss ring (arrow) visible in front of the disc demonstrating induction of a PVD by the CRVO
2.
The vitreoretinal adhesions at the vitreous base move gradually posteriorly as the eye ages (Wang et al. 2003).
Fig. 4.4
One patient’s drawing of his floaters from posterior vitreous detachment showing the Weiss ring moving around in the eye
Patients often notice a floater in their vision describing it as a ‘cobweb’ or ‘spider’ or ‘fly’ which moves with eye movements. OCT has revealed that many adults have an incomplete PVD not visible on biomicroscopy but with separation of the posterior hyaloid membrane from the retina with residual attachments at the optic disc or the fovea (Uchino et al. 2001).
Table 4.1
Vitreoretinal conditions and the vitreous
Vitreoretinal conditions and the vitreous | |
|---|---|
Caused by age-related posterior vitreous detachment | Retinal breaks |
Rhegmatogenous retinal detachment | |
Macular epiretinal membrane and vitreomacular traction syndrome | |
Macular hole | |
Vitreous haemorrhage | |
Associated with pathological vitreous separation | Diabetic tractional retinal detachment |
Complications of posterior uveitis | |
Trauma | |
4.1.1 Symptoms
Floaters
Floaters must be discriminated from paracentral scotomata. Ask the patient to describe the floater which should have momentum as the eye moves, that is, the floater will move with the eye but will continue to move when the eye stops before finally returning to its original position and resting there. In contrast, a scotoma remains in the same position (relative to fixation) in all positions of gaze. The patient may also describe the floater as something in front of the vision or ‘in the way’ of the vision. Floaters can be characterised by cobweb, veils, a ring, spot or multiple spots. These come from thickened posterior hyaloid membrane, Weiss ring, or cells that have been dispersed into the vitreous. Floaters that occur before the age of 40 years and are chronic in presentation are most often due to vitreous degeneration without posterior vitreous detachment. However, it may only take a single floater of recent onset to indicate the development of a posterior vitreous detachment.
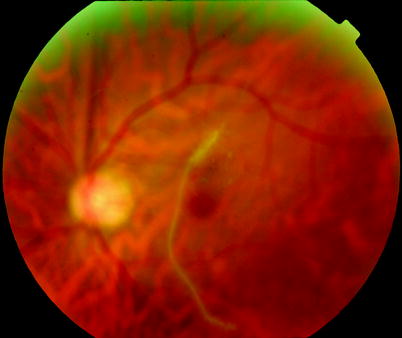
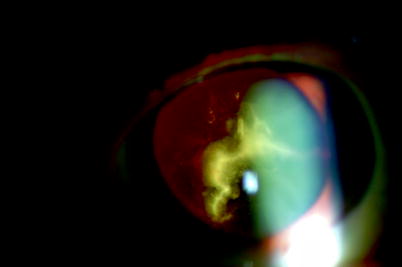
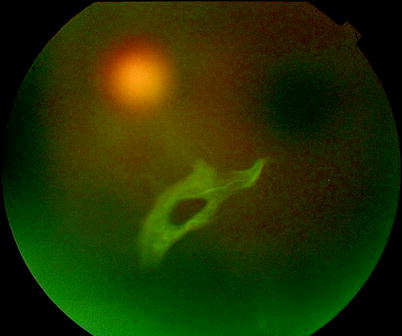
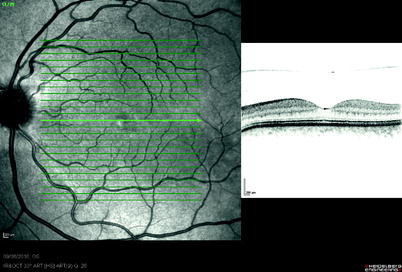
Fig. 4.5
Large ‘pipe-cleaner’-shaped vitreous opacities can be seen in moderate or highly myopic eyes without the presence of PVD. If you operate to remove these for symptomatic reduction of floaters, be aware that a vitreoschisis must be looked for and removed; otherwise, the posterior hyaloid may separate later on and cause RRD (see Chap. 7)
Fig. 4.6
If vitreous opacities are very symptomatic, these can be removed by vitrectomy. Beware of the high myope with apparent PVD who in fact has a vitreoschisis (see Chap. 6)
Fig. 4.7
A Weiss ring is apparent in this picture. A Weiss ring may take various forms in different eyes, and as the Weiss ring moves more anteriorly in the eye, it becomes less in focus and less noticeable by the patient
Fig. 4.8
An occult separation of the posterior hyaloid membrane from the macula, only visible on OCT
Flashes
Introduction
Photopsia is the experience of light from non-photic stimulation; the first description in the modern era was from Purkinje in 1819 (Purkinje 1819), who attributed them to traction. In 1935 and 1940, Moore described ‘lightning streaks’ (Moore 1935) with a ‘flash-like appearance of the lights; their position, sometimes slanting but usually vertical, and almost always to the outer side of the eyes, persisting for periods of up to 3 months; and their association with the sudden development of muscae volitantes, or the presence of visible vitreous opacities’. In 1940, he added more cases using the term lightning flashes (Moore 1940) and developed streaks in his own eye in 1947 (Moore 1947). He initially thought the phenomenon to be wholly benign, although he commented that ‘I used systematically to dilate the pupils and to take the visual fields in fear lest they might indicate some early organic retinal lesion, such as a commencing detachment, vascular disease, or perhaps an early neoplasm’ (Moore 1935). The flashes were attributed to posterior vitreous detachment (PVD) by Verhoeff (1941) in 1941 and the risk of retinal detachment associated with lightning flashes noted by Berens et al. (1954) in 1954. In 2008, ‘black flashes’ or negative flashes were described at the commencement of the PVD (Williamson et al. 2008) which have been attributed to traction of the vitreous on the optic nerve head, see below.
Clinical Characteristics
Patients experience ‘lightning flashes’ in the temporal periphery of their visual field that typically last a second at a time. Their exact pathogenesis is obscure but may be due to depolarisation of the receptors from tugging of the vitreous base on the retina. They may occur on eye movements. If the patient produces repeated eye movements over a short time, the flashes gradually reduce in severity. This may be because the retina loses the ability to respond due to repeated depolarisation of the receptors. Sometimes they are better seen at night. In some patients, black temporal flashes are seen for a few hours before the lightning flashes and floaters occur (Williamson et al. 2008). These are thought to be produced by the Weiss ring pulling on the optic nerve head before it separates. The forces applied in this way to the surface of the nerve head block axoplasmic flow in the superficial nerve fibres, thereby inducing a negative peripheral visual phenomenon. As soon as the Weiss ring separates, the symptoms change to floaters and lightning flashes. Typically, the lightning flashes of PVD are vertical, temporally placed and instantaneous flashes. If the flashes in a patient with PVD are oblique or horizontally orientated, not in the temporal visual field or not typical instantaneous flashes, the patient is more likely to have a PVD with a retinal tear or rhegmatogenous retinal detachment (Goodfellow et al. 2009).
These visual phenomena should be discriminated from the flashes that occur with other disorders, such as the zigzag lights of migraine, flickering stars associated with occipital ischaemia and the rare coloured lights of the acute zonal outer occult retinopathy (AZOOR) syndromes. Mostly, this photopsia is centrally placed in the visual field and therefore can be easily discriminated. Slower more mid-peripheral flashes are produced by the leading edge of some retinal detachments often shaped like a comet’s tail.
Patients who experience symptoms during posterior vitreous separation have a 10 % risk of developing a retinal tear (van Overdam et al. 2001; Sharma et al. 1999; Hikichi and Trempe 1994). Flashes from PVD usually subside in a few months, whilst floaters get less but may not disappear entirely (Serpetopoulos 1997). The floaters lessen as the opacities on the posterior surface of the vitreous sink lower in the eye but also because they move anteriorly and are less in focus than when they were nearer the inner surface of the retina. Severe floaters can be bothersome, and in a few patients, PPV is required to clear the vision. Rarely flashes will persist for years more often associated with vitreous attached young myope RRD (i.e. flashes associated with RRD rather than PVD) and very rarely after PVD. Occasionally, patients will have flashes after PPV.
Fig. 4.9
There are multiple causes of photopsia
Table 4.2
Different presentations of flashes
Flashes | |||||||
|---|---|---|---|---|---|---|---|
Diagnosis | Duration | Colour | Location | Shape | Stimulus | Other symptoms | Flickering |
PVD | Seconds or less | White | Temporal periphery | Crescentic vertical | Eye movements | Floaters | No |
Migraine | 20–30 min | Not typically | Paracentral | Arcuate | Stress, food | Scotoma headache nausea | Yes |
Zigzag | |||||||
Occipital ischemia | Minutes | Nil | Central | Petaloid | Neck movements exertion | Yes | |
Cystoid macular oedema | Constant | Variable | Central | Pinpricks | Nil | Poor vision | Yes |
Outer retinal or RPE abnormality | Minutes | Blue | Paracentral | Blobs | Nil | Scotoma | No |
Purple | Spirals | ||||||
Retinal detachment | Seconds | Golden | Central/paracentral | Comet oblique horizontal | Eye movements | Visual field loss | No |
4.1.2 Signs
Detection of PVD

Fig. 4.10
In an eye with forward displacement of a PVD, the posterior hyaloid membrane can be seen in the anterior vitreous cavity
A posterior vitreous detachment can be diagnosed by examining the eye with a 90-dioptre lens. Definitively, if a Weiss ring is present, then a PVD has occurred. Sometimes this is not obvious, but it is possible to see the posterior hyaloid membrane. This is more subjective, but it can be reassuring to observe the space behind the membrane; if this is optically clear, it suggests that there is no vitreous gel at this location. A partial posterior vitreous detachment is a diagnosis that should be made only with care. It can be extremely difficult to determine whether there are remaining vitreous attachments. Likely residual attachments are at the optic disc, chorioretinal scars and epiretinal membranes at the macula and neovascular tissue. Usually, a posterior vitreous detachment occurs completely, soon after the onset of symptoms probably in a few hours. There remain a few patients in whom the posterior vitreous detachment progresses over a few weeks as evidenced by the formation of new retinal breaks in the first 6 weeks after onset of symptoms in 1.8–3.4 % (Hollands et al. 2009).
Shafer’s Sign
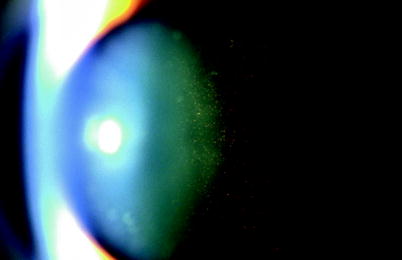
Fig. 4.11
Pigment granules in the vitreous are good indicators of the presence of a retinal tear from PVD
In most patients with tears, retinal pigment epithelial cells released through the tear will be visible in the anterior vitreous (Shafer’s sign). This is highly predictive of a retinal tear (approximately 90 %) (Tanner et al. 2000; Dayan et al. 1996; Byer 1994; Brod et al. 1991; Sharma et al. 1999). In symptomatic PVD, 10 % of patients will develop retinal tears. Most tears are present when the patient presents; however, 10 % of tears are be detected at 6 weeks from onset of symptoms (constituting theoretically 1 % of all cases with symptomatic PVD) (Richardson et al. 1999; Dayan et al. 1996). Breaks found in asymptomatic eyes are less likely to lead to retinal detachment (Byer 1998).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


