 Posterior Uveal Melanoma: Management
Posterior Uveal Melanoma: ManagementPosterior Uveal Melanoma: Management
In recent years, there have been advances in the management of posterior uveal melanoma, and several options are now available (1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71, 72, 73, 74, 75, 76, 77, 78, 79, 80, 81, 82). The selected management depends on factors like the size, location, and activity of the melanoma as well as the status of the opposite eye and the age, general health, and psychological status of the patient. Each patient should undergo a detailed ophthalmic evaluation, and the size and extent of the tumor should be carefully documented with accurate drawings. The known risk factors for growth and metastasis should be considered (12,13), and the patient should then be counseled about the therapeutic options (64).
Some informative results have come from the Collaborative Ocular Melanoma Study (COMS). That study confirmed that plaque radiotherapy and enucleation offer the same prognosis for medium-sized melanomas (32). Some authorities have been critical of COMS because of its enormous cost (9).
Observation
In recent years, there has been a belief that borderline lesions in which the diagnosis is questionable should be followed with fundus photography and ultrasonography to document tumor growth before undertaking definitive treatment. There is an emerging philosophy toward active treatment rather than observation for selected small choroidal melanocytic lesions (65,66,80). This has come about because recent studies have identified risk factors that are statistically related to a greater chance of metastasis (12,13). Factors that differentiate small choroidal melanoma from choroidal nevus can be remembered by using the mnemonic TFSOM, indicating To Find Small Ocular Melanoma. The letters in this mnemonic represent T (thickness >2 mm), F (subretinal fluid), S (symptoms), O (orange pigment), and M (margin touching optic disc). Choroidal melanocytic tumors that display no factors have 3% chance for growth at 5 years and most likely represent choroidal nevi. Tumors that display two or more factors show growth in >50% of cases at 5 years (36).
Laser Photocoagulation
Some small and some medium-sized melanomas can be managed with techniques of laser photocoagulation (14,15). Standard photocoagulation is used less often today because transpupillary thermotherapy (TTT) in the infrared range using a diode laser delivery system has shown promising results in many cases (16, 17, 18, 19, 20).
Thermotherapy
Transpupillary thermotherapy involves heating the tumor by using light in the infrared range (810 nm) with a diode laser delivery system. It gives the best results in cases of melanomas <2 mm thick in which growth is documented. However, it has been used successfully for tumors up to 4 mm in thickness (16, 17, 18, 19, 20). Appropriate tumor selection is critical to successful treatment. In our experience, tumors >3 mm in thickness are best treated with plaque radiotherapy combined with TTT. Patients with tumors abutting or overhanging the optic disc or those requiring more than three sessions for tumor control are more likely to develop tumor recurrence if TTT is used as the only treatment. Potential complications of TTT include retinal branch vein obstruction, retinal traction, and induction of a retinal hole with secondary retinal detachment, which is uncommon (82). However, many patients have had adequate tumor destruction and favorable visual outcomes.
Because of the potential for vitreoretinal complications using the transpupillary technique, studies are being conducted on techniques of trans-scleral thermotherapy. The results are preliminary.
Charged Particle Irradiation
Techniques of radiotherapy using charged particles have also shown good results (37, 38, 39, 40). We have not used this technique, but reports suggest that survival data and tumor control are similar to results with plaque radiotherapy. Like plaque radiotherapy, charged particles (proton beams or helium ions) can be used for many medium-sized or large posteriorly located melanomas in which there is a reasonable chance of preserving some vision.
Plaque Brachytherapy
Plaque radiotherapy is the most commonly used method of treating uveal melanoma. Extensive experience with plaque brachytherapy has suggested that it offers good tumor control, can often preserve useful vision, and offers a prognosis comparable to that of enucleation (24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35). Plaque radiotherapy requires close cooperation among ocular oncologists, radiation oncologists, and radiation physicists. It is recognized that plaque radiotherapy can be used to treat large melanomas, macular melanoma (28), ciliary body melanoma (29), and extraocular extension of uveal melanoma (30). Similar results have been obtained with charged particle irradiation. However, anterior segment complications appear to be greater after charged particle irradiation than after plaque radiotherapy (76).
The COMS has also confirmed previous data comparing plaque radiotherapy and enucleation with regard to metastasis and mortality. In COMS, mortality rates following plaque brachytherapy with radioactive iodine-125 did not differ from mortality rates following enucleation for up to 12 years after treatment of patients with medium-sized choroidal melanoma (32,83).
Other Radiation Methods
Other methods of irradiation for uveal melanoma are under investigation, including stereotactic radiosurgery, gammaknife, and cyberknife methods (40).
Local Resection
A melanoma located in the ciliary body and peripheral choroid can be managed by local removal of the tumor (41, 42, 43, 44, 45, 46, 47, 48, 49). Several years ago, a full-thickness eye wall resection with a scleral graft
was usually employed (41). More recently, techniques of partial lamellar sclerouvectomy have been used (42, 43, 44, 45). The surgical procedure can be difficult and requires considerable skill and experience, but the results are often very gratifying (45). Supplemental plaque radiotherapy can be used after local resection if the melanoma is high grade and near the margins of resection.
was usually employed (41). More recently, techniques of partial lamellar sclerouvectomy have been used (42, 43, 44, 45). The surgical procedure can be difficult and requires considerable skill and experience, but the results are often very gratifying (45). Supplemental plaque radiotherapy can be used after local resection if the melanoma is high grade and near the margins of resection.
There has been some recent interest in removing a posterior uveal melanoma by endoresection, using vitrectomy instrumentation (49). We do not perform the procedure because we have concern about removing a malignant melanoma in a piecemeal fashion. However, we await long-term follow-up on cases managed in this manner.
Enucleation
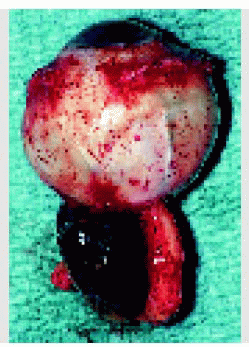
Enucleation is appropriate for large melanomas in which there is little hope of salvaging useful vision with more conservative treatments or for tumors that surround or invade the optic nerve. Although there is some flexibility, depending on the other clinical factors, we generally lean toward enucleation when a melanoma is >18 mm in diameter and 10 mm in thickness because the morbidity is greater following radiotherapy for tumors that large.
There are a number of techniques for replacing the orbital volume with an implant. In recent years, we have used a 20-mm hydroxyapatite implant wrapped with eye bank sclera. More recently, we have used a polymer-coated hydroxyapatite implant (75). When there was a sizable circumscribed nodule of orbital extension of uveal melanoma, in several cases we used a method of enucleation via a lateral orbitotomy approach as an alternative to orbital exenteration (56).
The subject of pre-enucleation external irradiation for uveal melanoma has been a topic of some debate. A COMS report (51) verified a prior report that there is no difference in patient survival when comparing enucleation only with enucleation preceded by external beam radiation for medium-sized choroidal melanomas (50).
Orbital Exenteration
Occasionally, a uveal melanoma shows massive orbital extension, at the time of initial diagnosis, and in such cases, primary orbital exenteration is often warranted. We have generally used an eyelid-sparing technique in such cases (57,58). The technique is illustrated in Chapter 25.
Combination Methods
In recent years, there has been increasing use of combined methods to treat a posterior uveal melanoma. Many patients have been treated by methods of plaque radiotherapy combined with TTT and local resection followed by plaque radiotherapy and other combined methods. At the time of this writing, most choroidal melanomas on our service are treated with plaque radiotherapy combined with TTT. With this approach, tumor control has been achieved in greater than 95% of cases (36).
Genetic Studies
Recent genetic studies of uveal melanoma have shown abnormalities on chromosomes 1, 3, 6, 8, 11, and 13. The most significant predictor of poor life prognosis at this time is chromosome 3 monosomy (77, 78, 79). Cytogenetic analysis can also be performed on fine needle aspiration biopsy specimens (79). Patients with monosomy 3 abnormality are being offered more rigorous follow-up and management with systemic chemotherapy or immunotherapy protocols.
Systemic Treatment
The management of choroidal melanoma will be improved if effective systemic therapies can be identified. Techniques of hepatic artery chemoembolization with a variety of agents and local surgical removal of selected solitary distant metastasis have met with limited success. In the future, it is expected that primary treatment of uveal melanoma will be mostly directed toward eradicating subclinical distant metastasis (65,66). It is most likely that the ideal management will be very early detection and prompt treatment of small uveal melanoma combined with intensive systemic therapy in the form of chemotherapy, immunotherapy, gene therapy, and/or other methods with techniques yet to be determined.
Selected References
1. Shields JA, Shields CL. Management of posterior uveal melanoma. In: Shields JA, Shields CL, eds. Intraocular Tumors. A Text and Atlas. Philadelphia: WB Saunders; 1992:171-205.
2. Shields JA, Shields CL, Donoso LA. Management of posterior uveal melanomas. Surv Ophthalmol 1991;36:161-195.
3. Zimmerman LE, McLean IW, Foster WD. Does enucleation of the eye containing a malignant melanoma prevent or accelerate the dissemination of tumour cells? Br J Ophthalmol 1978;62:420-425.
4. Zimmerman LE, McLean IW. An evaluation of enucleation in the management of uveal melanomas. Am J Ophthalmol 1979;87:741-760.
5. Seigel D, Myers M, Ferris F, et al. Survival rates after enucleation of eyes with malignant melanoma. Am J Ophthalmol 1979;87:751-765.
6. Manschot WA, Van Peperzeel HA. Choroidal melanoma—enucleation or observation? A new approach. Arch Ophthalmol 1980;98:71-77.
7. Straatsma BR, Fine SL, Earle JD. The Collaborative Ocular Melanoma Study Research Group. Enucleation versus plaque irradiation for choroidal melanoma. Ophthalmology 1988;95:100-104.
8. Shields CL, Shields JA. Clinical features of small choroidal melanoma. Curr Opin Ophthalmol 2002;13:135-141.
9. Benson WE. The COMS: why was it not stopped sooner? Arch Ophthalmol 2002;120:672.
10. Robertson DM. Changing concepts in the management of choroidal melanoma. Am J Ophthalmol 2003;136:161-170.
11. Gass JDM. Observation of suspected choroidal and ciliary body melanomas for evidence of growth prior to enucleation. Ophthalmology 1980;87;523-528.
12. Shields CL, Shields JA, Kiratli H, et al. Risk factors for growth and metastasis of small choroidal melanocytic lesions. Ophthalmology 1995;102:1351-1361.
13. Shields CL, Cater JC, Shields JA, et al. Combination of clinical factors predictive of growth of small choroidal melanocytic tumors. Arch Ophthalmol 2000;118:360-364.
14. Foulds WS, Damato BE. Low energy long-exposure laser therapy in the management of choroidal melanoma. Graefes Arch Clin Exp Ophthalmol 1986;224:26-31.
15. Shields JA, Glazer LC, Mieler WF, et al. Comparison of xenon arc and argon laser photocoagulation in the treatment of choroidal melanomas. Am J Ophthalmol 1990;109:647-655.
16. Oosterhuis JA, Journee-de Korver HG, Kakebeeke-Kemme HM, et al. Transpupillary thermotherapy in choroidal melanomas. Arch Ophthalmol 1995; 113: 315-321.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


