 Posterior Uveal Melanoma: Diagnostic Approaches
Posterior Uveal Melanoma: Diagnostic ApproachesPosterior Uveal Melanoma: Diagnostic Approaches
General Considerations
In most instances, the diagnosis of posterior uveal melanoma can be made by recognition of its classic features using slit lamp biomicroscopy or indirect ophthalmoscopy. However, the diagnosis and extent of the tumor can be supported or confirmed by the judicious use of ancillary studies such as transillumination, fluorescein angiography, indocyanine green angiography (ICGA), ultrasonography, ultrasound biomicroscopy (UBM), optical coherence tomography (OCT), computed tomography, magnetic resonance imaging, radioactive phosphorus uptake test (P32 test), and fine needle aspiration biopsy (FNAB) (1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14). In cases that are atypical ophthalmoscopically, these ancillary studies assume a more vital role in diagnosis. These techniques are discussed in detail in the literature. The most important ancillary studies are fluorescein angiography and ultrasonography. Computed tomography (CT), magnetic resonance imaging (MRI), and the P32 test are rarely necessary to make the diagnosis of uveal melanoma. However, FNAB has become the most reliable diagnostic method in cases in which the lesion is atypical and a precise diagnosis is more difficult.
Transillumination
Transillumination is a very useful technique in the diagnosis of ciliary body and anterior choroidal melanoma in certain circumstances, and several techniques of transillumination have been described (1). It is done by placing a bright light in the conjunctival fornix with dim room illumination and observing the sclera that normally transmits light posterior to the pars plicata. In the case of pigmented ciliary body melanoma and most nonpigmented melanomas, a shadow will be cast that corresponds to the location of the melanoma. In contrast, cystic lesions, leiomyomas, and several other conditions tend to transmit light rather than cast a shadow.
Fluorescein Angiography and Indocyanine Green Angiography
With fluorescein angiography, a typical choroidal melanoma shows mottled hyperfluorescence in the vascular filling phases and diffuse late staining of the mass and its overlying subretinal fluid. A larger amelanotic melanoma, particularly one that has broken through Bruch’s membrane, may show more clearly the characteristic double circulation in which both the retinal vessels and the choroidal vessels in the tumor are readily evident. Areas of tumor invasion of the overlying sensory retina are relatively hypofluorescent throughout the angiogram sequence. ICGA shows characteristic features of uveal melanoma that can be of diagnostic help in difficult cases. It can assist in visualizing the typical pattern of choroidal blood vessels in the tumor when there is overlying blood (2).
Ultrasonography
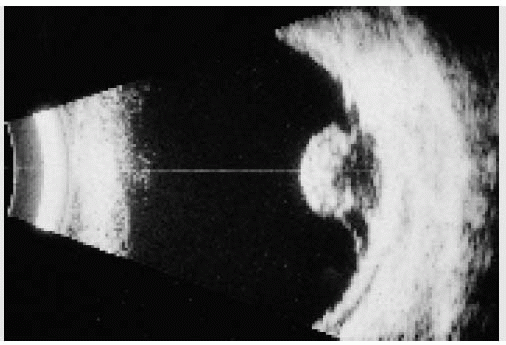
With A-scan ultrasonography, choroidal melanoma typically shows medium to low internal reflectivity, and with B-scan ultrasonography, it shows a choroidal mass pattern with acoustic hollowness and choroidal excavation. Ultrasonography can delineate small nodules of extraocular extension of the tumor (1). It is particularly helpful in eyes with opaque media from secondary cataract or vitreous hemorrhage. It is useful for confirming the diagnosis of uveal melanoma and also for measuring tumor size before and after the tumor has been treated with irradiation. In some instances, ultrasonography of a ciliary body melanoma reveals clear cavities in the lesion and a thick, solid lining of the cavitary spaces. This is called a cavitary melanoma (14), and it differs from a ciliary body cyst that has a thin lining without a solid component.
Ultrasound Biomicroscopy
UBM is a variation of ultrasonography that is used to measure the size and extent of tumors in the anterior segment of the eye. It is particularly useful for determining whether a peripheral iris tumor extends posteriorly into the ciliary body. It is helpful in differentiating a cyst from a melanoma or other solid tumors in the ciliary body area.
Computed Tomography and Magnetic Resonance Imaging
CT and MRI can be used to visualize uveal melanoma and to completely delineate larger areas of orbital extension (3). They are not usually employed to make the diagnosis of uveal melanoma because the diagnosis can be readily made in the great majority of cases by simpler and less expensive methods, particularly ophthalmoscopy and ultrasonography.
Fine Needle Aspiration Biopsy
FNAB can be used to make the diagnosis of choroid melanoma in difficult cases that defy clinical diagnosis using less invasive measures (5). The most commonly employed technique is a trans-pars plana, transvitreal approach using a 25-gauge needle. The technique is detailed in the literature and in Chapter 22 (1,5).
Radioactive Phosphorus Uptake Test
The radioactive phosphorus uptake test (P32 test) can be used to make the diagnosis in difficult cases (4). It involves intravenous injection of a low dose of radioactive phosphorus, with Geiger counter readings taken on the sclera directly over the location of the tumor after 48 hours. Malignant neoplasms generally show a positive uptake, whereas benign lesions show a negative result. Although this accurate and reliable test was used extensively in the past, it is rarely used today
because of the advent and perfection of other diagnostic techniques, particularly FNAB, which provide cytopathologic verification of the diagnosis.
because of the advent and perfection of other diagnostic techniques, particularly FNAB, which provide cytopathologic verification of the diagnosis.
Optical Coherence Tomography
Optical coherence tomography (OCT) is a more recent diagnostic tool used to measure retinal thickness and to detect subtle subretinal fluid, cystoid retinal edema, and surface wrinkling retinopathy. Although it cannot specifically diagnose a choroidal melanoma or other tumors, it can be used to detect subtle retinal changes that suggest that a tumor is growing or more aggressive than a standard nevus.
Selected References
1. Shields JA, Shields CL. Diagnostic approaches to posterior uveal melanoma. In: Shields JA, Shields CL, eds. Intraocular Tumors. A Text and Atlas. Philadelphia: WB Saunders; 1992:155-169.
2. Shields CL, Shields JA, De Potter P. Patterns of indocyanine green angiography of choroidal tumors. Br J Ophthalmol 1995;79:237-245.
3. DePotter P, Shields JA, Shields CL. Disorders of the globe. Tumors of the uvea. In: DePotter P, Shields JA, Shields CL, eds. MRI of the Eye and Orbit. Philadelphia: Lippincott; 1995:56-92.
4. Shields JA. Accuracy and limitation of the P-32 test in the diagnosis of ocular tumors. An analysis of 500 cases. Ophthalmology 1978;85:950-966.
5. Shields JA, Shields CL, Ehya H, et al. Fine needle aspiration biopsy of suspected intraocular tumors. The 1992 Urwick Lecture. Ophthalmology 1993;100:1677-1684.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


