 Posterior Uveal Melanoma: Clinical Features
Posterior Uveal Melanoma: Clinical FeaturesClinical Features of Posterior Uveal Melanoma
General Considerations
Melanoma of the posterior uvea (ciliary body and choroid) is the most common malignancy encountered by ophthalmologists, and its epidemiology and clinical features are well known (1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29). It arises from melanocytes in the posterior uveal tract. The epidemiology and general aspects of uveal melanoma are discussed in detail elsewhere. Its annual age-adjusted incidence in the United States is about 6 cases per 1 million population (2,10,29). It is decidedly more common in adult whites and is uncommon in children and in dark-skinned individuals (9, 10, 11, 12, 13). Predisposing conditions for uveal melanoma include ocular melanocytosis, white race, and possibly the dysplastic nevus syndrome. The clinical features of posterior uveal melanoma are well established and are described mainly in textbooks and a few descriptive articles (1, 2, 3). It is important for ophthalmologists to be familiar with the clinical features of ciliary body and choroidal melanoma because this neoplasm can cause blindness and death.
Clinical Features of Ciliary Body Melanoma
In contrast to iris melanoma, ciliary body melanoma can often attain a larger size before it is recognized clinically. However, it is frequently associated with external ocular signs that suggest the underlying diagnosis. The most important sign is one or more dilated episcleral blood vessels (sentinel vessels). A second sign is an epibulbar pigmented lesion characteristic of transcleral extension of the tumor (2,7). When the pupil is dilated widely, the ciliary body tumor can be visualized in the affected area as a dome-shaped mass. Less frequently, it can assume a diffuse circumferential ring growth pattern (ring melanoma) (8). Ciliary body melanoma can impinge on the lens, causing subluxation and cataract. It can grow posteriorly into the choroid (ciliochoroidal melanoma) and anteriorly into the anterior chamber angle and iris (iridociliary melanoma). It can infiltrate the trabecular meshwork, causing secondary glaucoma.
Clinical Features of Choroidal Melanoma
Choroidal melanoma usually presents as a sessile or dome-shaped mass located deep to the sensory retina. A smaller posterior choroidal melanoma may have surface orange pigment at the level of the retinal pigment epithelium (1, 2, 3, 4). A secondary nonrhegmatogenous retinal detachment frequently occurs. In contrast to a rhegmatogenous detachment, in which the subretinal fluid does not shift, the fluid with melanoma and other tumors shifts with positional changes of the patient’s head. Occasionally, a choroidal melanoma can be partly or entirely nonpigmented. When the tumor is amelanotic, blood vessels in the tumor are visible ophthalmoscopically. With continued growth, a choroidal melanoma can rupture Bruch’s membrane and assume a mushroom shape. When that occurs, the tumor has a tendency to bleed, and vitreal or subretinal blood can sometimes obscure a view of the underlying tumor. Choroidal melanoma can also assume a diffuse growth pattern with only minimal elevation of the tumor (4,5). In some instances, ciliary body or choroidal melanoma can cause total cataract, secondary glaucoma, and extraocular extension into the orbit. Such tumors are generally larger and carry a worse prognosis (6,7).
Spontaneous Regression of Choroidal Melanoma
In unusual instances, choroidal melanoma has been documented to undergo spontaneous regression (27,28). A spontaneously regressed melanoma generally is relatively flat and has amelanotic areas that represent regions of necrosis in the tumor. Areas of retinal pigment epithelium alterations suggest that prior active retinal detachment has resolved. Another typical feature is a well-defined overlying area of retinoschisis (intraretinal cyst), at the base of which is a characteristic crater in the tumor. Melanomas with such necrosis can rarely recur as an active tumor after months or years (27,28).
Risk Factors for Growth and Metastasis of Small Melanocytic Choroidal Lesions
Important risk factors for growth and metastasis of small melanocytic choroidal lesions have been identified (24,25). Statistical risk factors for growth include tumor thickness >2 mm at initial diagnosis, overlying orange pigment, subretinal fluid, proximity to the optic disc, and presence of symptoms. Clinical factors predictive of possible eventual metastasis include tumor thickness >2 mm at initial diagnosis, tumor proximity to the optic disc, presence of symptoms, and documented enlargement. These should be determined and used in counseling the patient and in determining whether a lesion should be observed periodically or actively treated (24,25).
Selected References
1. Gass JDM. Choroidal malignant melanoma. In: Gass JDM, ed. Stereoscopic Atlas of Macular Diseases, 3rd ed., Vol. 1. St. Louis: CV Mosby; 1987: 190-192.
2. Shields JA, Shields CL. Posterior uveal melanoma: clinical and pathologic features. In: Shields JA, Shields CL, eds. Intraocular Tumors. A Text and Atlas. Philadelphia: WB Saunders; 1992:117-136.
3. Shields JA. Posterior uveal melanoma. In: Guyer DR, Yannuzzi LA, Chang S, et al. Retina-Vitreous-Macula, Vol. 2. Philadelphia: WB Saunders; 1999: 1067-1073.
4. Font RL, Spaulding AG, Zimmerman LE. Diffuse malignant melanomas of the uveal tract. Trans Am Acad Ophthalmol Otolaryngol 1968;72:877-895.
5. Shields CL, Shields JA, DePotter P, et al. Diffuse choroidal melanoma: clinical features predictive of metastasis. Arch Ophthalmol1996:114:956-963.
6. Shields CL, Shields JA, Shields MB, et al. Prevalence and mechanisms of secondary intraocular pressure elevation in eyes with intraocular tumors. Ophthalmology 1987;94:839-846.
7. Shields JA, Shields CL. Massive orbital extension of posterior uveal melanoma. J Ophthalmic Plast Reconstr Surg 1991;7:238-251.
8. Demirci H, Shields CL, Shields JA, et al. Ring melanoma of the ciliary body: report on twenty-three patients. Retina 2002;22:698-706.
9. Biswas J, Kabra S, Krishnakumar S, et al. Clinical and histopathological characteristics of uveal melanoma in Asian Indians. A study of 103 patients. Ind J Ophthalmol 2004;52:41-44.
10. Scotti J, Fraumeni JF Jr, Lee JH. Melanomas of the eye and other noncutaneous sites: epidemiologic aspects. J Natl Cancer Inst 1976;56:489-491.
11. Shields CL, Shields JA, Milite J, et al. Uveal melanoma in teenagers and children. A report of 40 cases. Ophthalmology 1991;98:1662-1666.
12. Singh AD, Shields CL, Shields JA, et al. Uveal melanoma in young patients. Arch Ophthalmol 2000;118:918-923.
13. Phillpotts BA, Sanders RJ, Shields JA, et al. Uveal melanomas in black patients: a case series and comparative review. J Nat Med Assoc 1995;87: 709-714.
14. Shields JA, Rodrigues MM, Sarin LK, et al. Lipofuscin pigment over benign and malignant choroidal tumors. Trans Am Acad Ophthalmol Otolaryngol 1976;81:871-881.
15. Spaide RF, Spirn MJ. Saccular aneurysms in a case of choroidal melanoma. Retina 2003;23:726-728.
16. Lois N, Shields CL, Shields JA, et al. Cavitary melanoma of the ciliary body. A study of eight cases. Ophthalmology 1998;105:1091-1098.
17. Zhang JJ, Demirci H, Shields CL, et al. Cavitary melanoma of ciliary body simulating a cyst. Arch Ophthalmol 2005;123:569-571.
18. Brown GC, Shields JA. Choroidal melanomas and paving-stone degeneration. Ann Ophthalmol 1983;15:705-708.
19. Eagle RC, Shields JA. Pseudoretinitis pigmentosa secondary to preretinal malignant melanoma cells. Retina 1982;2:51-55.
20. Shields JA, Shields CL, Kimmel A, et al. Contralateral blindness from chiasmal extension of unsuspected choroidal melanoma. Ophthalmic Plast Reconstr Surg 2004;20:384-387.
21. Shields JA, Naseripour M, Shields CL, et al. Choroidal melanoma in an immunosuppressed child with minimal change nephrotic syndrome. Retina 2004; 24:454-455.
22. Manquez ME, Shields CL, Demirci H, et al. Choroidal melanoma in a teenager with Klippel Trenaunay syndrome. Arch Ophthalmol. In press.
23. Singh AD, Shields CL, Shields JA, et al. Occurrence of retinoblastoma and uveal melanoma in the same patient. Retina 2000;20:305-306.
24. Shields CL, Shields JA, Kiratli H, et al. Risk factors for growth and metastasis of small choroidal melanocytic lesions. Ophthalmology 1995;102: 1351-1361.
25. Shields CL, Cater JC, Shields JA, et al. Combination of clinical factors predictive of growth of small choroidal melanocytic tumors. Arch Ophthalmol 2000;118:360-364.
26. Shields JA, Shakin EP, Shields CL, et al. Diffuse amelanotic balloon cell melanoma of the choroid. Ophthalmic Practice 1992;10:226-228.
27. Shields CL, Shields JA, Santos CM, et al. Incomplete spontaneous regression of choroidal melanoma associated with inflammation. Arch Ophthalmol 1999;117:1245-1247.
28. Lambert SR, Char DH, Howes E Jr, et al. Spontaneous regression of a choroidal melanoma. Arch Ophthalmol 1986;104:732-734.
29. Seddon JM, Young TA. Epidemiology of uveal melanoma. In: Ryan SJ, Hinton DR, Schachat AP, eds. Retina, 4th ed. St. Louis: Elsevier Mosby; 2006: 692-697.
▪ Ciliary Body Melanoma: Sentinel Blood Vessels
Although dilated episcleral blood vessels usually signify an underlying ciliary body melanoma, they can occasionally be seen with other, less common tumors like ciliary body metastasis, leiomyoma, schwannoma, melanocytoma, and epitheliomas (adenomas) of the nonpigmented or pigmented ciliary epithelium. On rare occasions, a dilated episcleral vessel is seen as a normal variant with no evidence of a ciliary body mass.
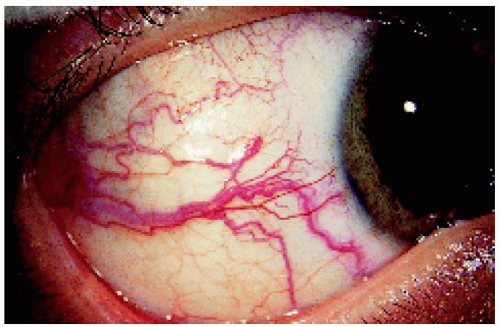 Figure 7.1. Large typical sentinel blood vessels temporally in a 38-year-old man. |
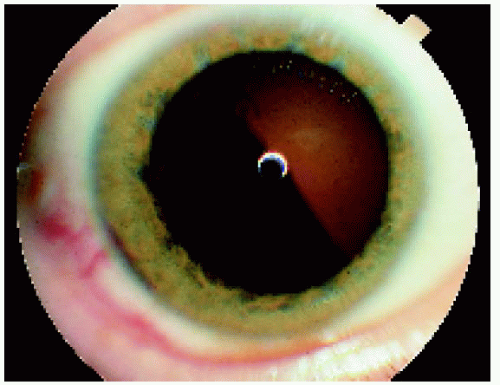 Figure 7.2. Photograph through the dilated pupil of the patient shown in Figure 7.1, clearly showing the pigmented ciliary body mass. |
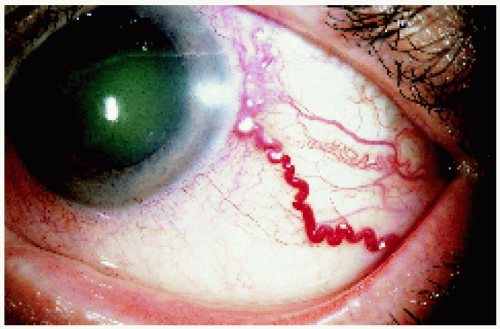 Figure 7.3. Large solitary sentinel vessel over a ciliary body melanoma in a 60-year-old man. |
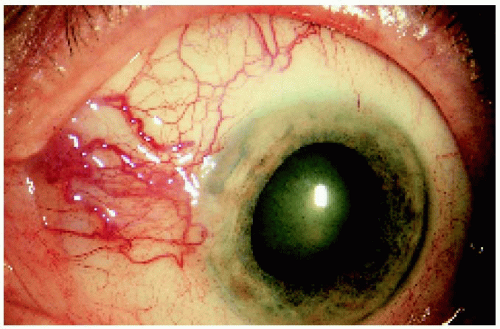 Figure 7.4. Multiple sentinel vessels over a ciliary body melanoma in a 77-year-old man. |
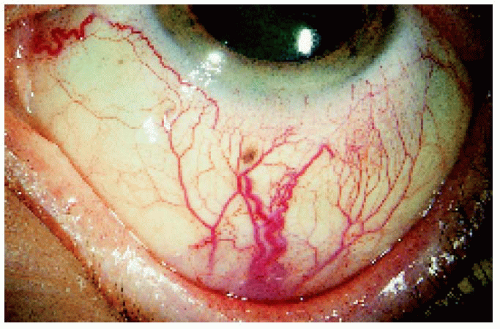 Figure 7.5. Inferior and nasal sentinel vessels over a large ciliary body melanoma in an 84-year-old woman. |
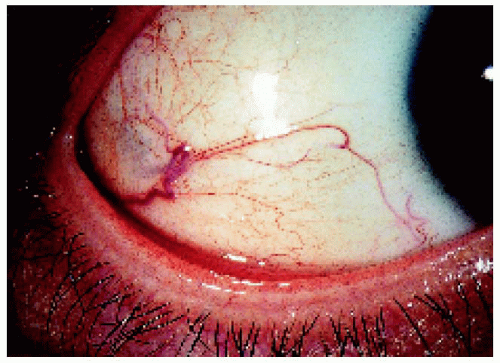 Figure 7.6. Pseudo-sentinel vessel in a 27-year-old person with an otherwise normal eye. Indirect ophthalmoscopy, gonioscopy, ultrasound biomicroscopy, and transillumination were performed to rule out the possibility of a small occult melanoma, and it was not present. |
▪ Ciliary Body Melanoma: Transcleral Extension
Ciliary body melanoma can frequently extend through emissary channels to appear in the episcleral tissues, sometimes forming an extraocular mass. It is more likely to occur with larger, more aggressive tumors, particularly those that grow in a ring pattern. In rare instances, anterior extraocular extension can invade the overlying conjunctiva. Transcleral extension usually imparts a worse systemic prognosis.
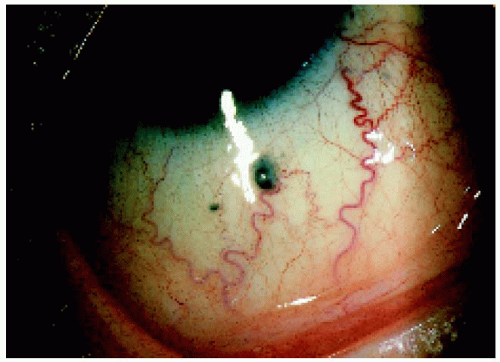 Figure 7.7. Two small foci of transcleral extension inferiorly in a 65-year-old man. |
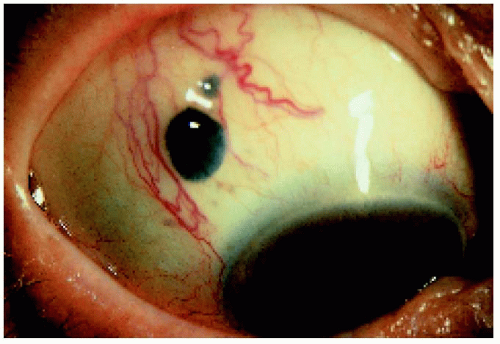 Figure 7.8. More prominent nodules of transcleral extension superiorly in a 77-year-old woman. |
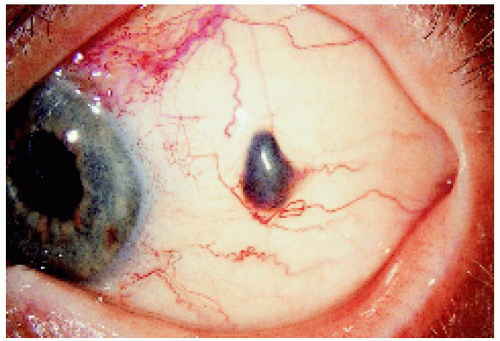 Figure 7.9. Slightly more posteriorly located nodule of transcleral extension in an 83-year-old man. |
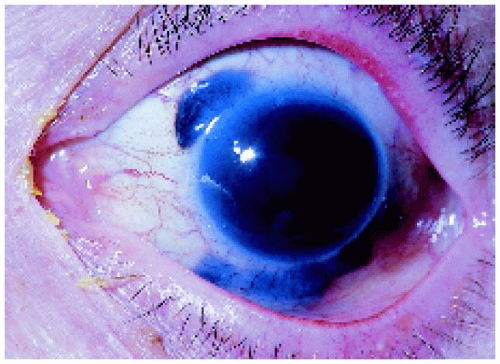 Figure 7.10. Multiple foci of a transcleral extension secondary to a ring melanoma of ciliary body in a 70-year-old woman. Ring melanoma with a transcleral extension carries a worse prognosis. |
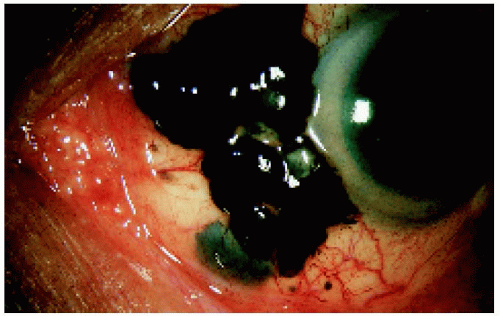 Figure 7.11. Massive transcleral extension and invasion of the overlying conjunctiva in a 58-year-old man with a ciliary body melanoma. |
 Figure 7.12. Massive extraocular extension of a neglected ciliary body melanoma in an 80-year-old man for whom orbital exenteration was required. He had declined treatment for a relatively small ciliary body melanoma detected 3 years earlier. |
▪ Ciliary Body Melanoma: Iris Extension
A ciliary body melanoma can grow through the iris root and appear as a mass in the peripheral portion of the iris, simulating a primary iris tumor. Unlike a primary iris melanoma, anterior extension of a ciliary body melanoma tends to pass through the iris root and produce a tumor-induced iridodialysis.
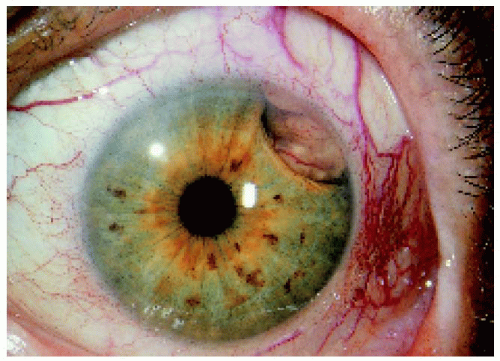 Figure 7.13. Iris extension of a superotemporal ciliary body melanoma in a 70-year-old woman. Note the sentinel vessels. |
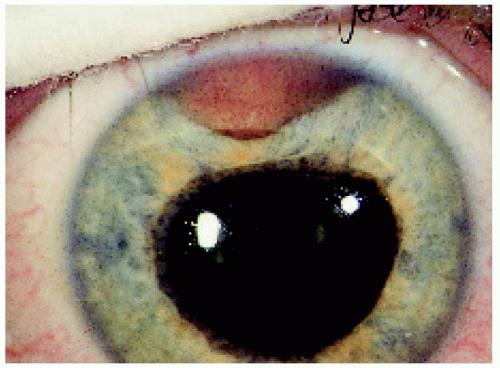 Figure 7.14. Iris extension of a superior ciliary body melanoma in a 52-year-old woman. |
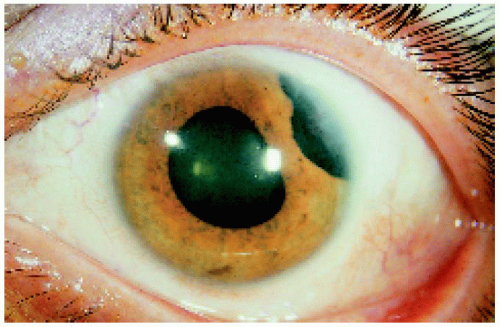 Figure 7.15. Iris extension of a superior ciliary body melanoma in a 37-year-old woman. |
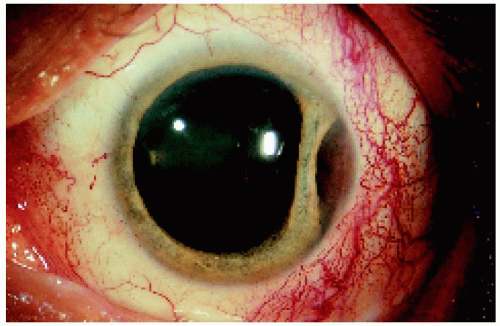 Figure 7.16. Iris extension of a temporal ciliary body melanoma in a 54-year-old man. Note the sentinel vessels and the accordionlike folds in the iris. The ciliary body component of the tumor can be visualized through the dilated pupil. |
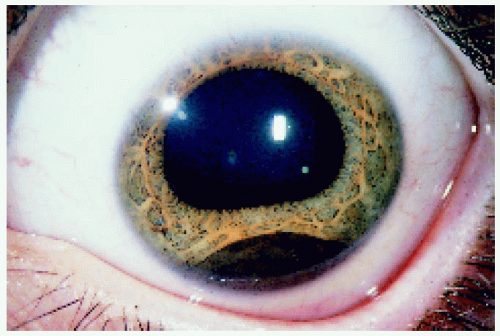 Figure 7.17. Iris extension of an inferior ciliary body melanoma in a 16-year-old girl. |
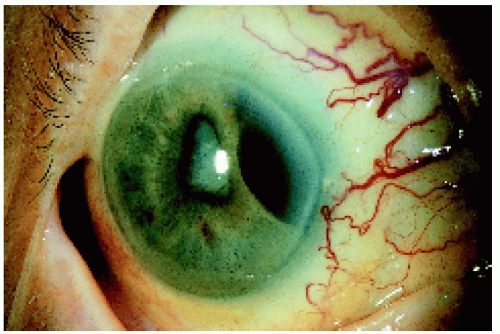 Figure 7.18. Iris extension and secondary cataract in an 85-year-old man with a large temporal ciliary body melanoma. Note the numerous sentinel vessels. |
▪ Ciliary Body Melanoma: Appearance Through a Dilated Pupil
Ciliary body melanoma generally appears as a dome-shaped pigmented mass that can encroach on the lens, producing subluxation and cataract. It can extend posteriorly into the choroid (ciliochoroidal melanoma). Occasionally it grows in a ring rather than a nodular pattern.
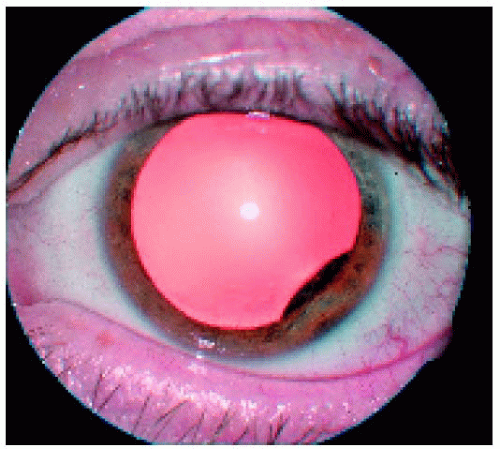 Figure 7.19. Relatively small ciliary body melanoma located inferotemporally in the left eye. Note also the subtle extension through the peripheral iris. |
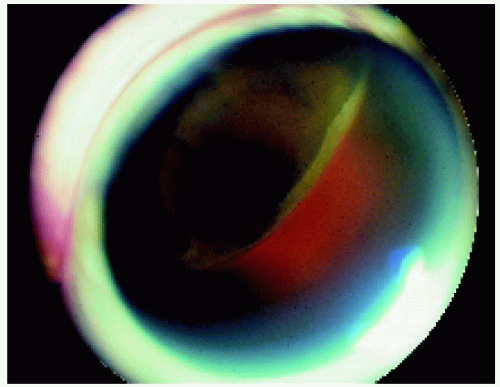 Figure 7.20. Ciliary body melanoma in a 63-year-old man. The tumor has extended into the choroid and lifted the ora serrata, so that it is visible on the dome of the tumor. |
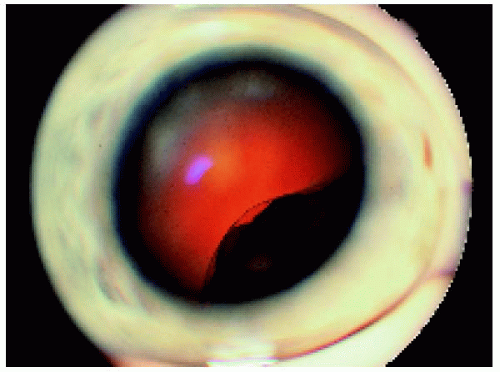 Figure 7.21. Ciliary body melanoma with an irregular surface in a 47-year-old man.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|