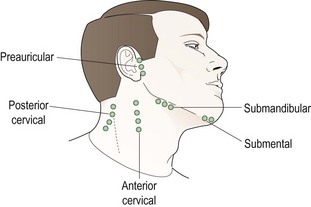
9 (a) Simple observation of the patient’s physical features can be useful. For example, obesity is a risk factor for hypertension and carotid artery disease. (b) A palpable preauricular node can be helpful information in determining the cause of a red eye. In addition, differential diagnosis of the cause of the red eye can begin in the case history with questions regarding the duration, recurrence and laterality of the red eye, any discomfort and type of discharge. (c) While mild to moderate hypertension does not cause headache, the presence of pulsating, suboccipital headaches that subside during the day, particularly in an older patient, may suggest acute hypertension and thus the need for sphygmomanometry.1 (d) Episodes of transient loss of vision (amaurosis fugax) may be present in carotid artery stenosis which requires further investigation. Amaurosis fugax is a sudden onset, painless loss of vision in one eye that is described as a curtain coming down over the vision. The vision loss generally lasts longer than one minute.2 The medical history in a patient with a red eye may be important in the differential diagnosis. For example, a history of a recent upper respiratory tract infection and contact with another person with a red eye could be suggestive of viral origin to the red eye, the history of a urogenital infection could be suggestive of Chlamydia, a history of cold sores is suggestive of herpes simplex virus conjunctivitis and a history of allergy with intensive itching is suggestive of allergic conjunctivitis.3 A history of hypertension, cardiovascular disease, cerebrovascular disease, obesity, physical inactivity, heavy alcohol intake, smoking, diabetes mellitus and hyperlipidaemia are important when considering if blood pressure measurement is indicated. When there is a positive family history the risk of developing hypertension is increased two to four times.4 The patient’s medical history should also include the current medical care for systemic conditions, frequency of monitoring for the conditions, previous and planned investigations for the conditions, medications prescribed and compliance with medication use. For example, if a patient has been diagnosed as hypertensive, is taking medication regularly and having their blood pressure regularly monitored, then there would be little need for optometric testing. If, however, the patient was previously diagnosed with hypertension, stopped taking their medication 6 months ago due to an adverse reaction and has not seen their physician to follow up, it would be prudent to take a blood pressure reading and advise the patient accordingly even in the absence of abnormalities on the ocular fundus examination. Ocular fundus features suggesting hypertension and the possible need for sphygmomanometry are discussed in section 9.3 and Table 9.1. Ocular risk factors for significant carotid artery stenosis include emboli (Hollenhorst plaques), retinal vascular occlusions, peripheral retinal haemorrhages with dilated and tortuous veins (hypoperfusion retinopathy), microrubeosis iridis, ocular ischaemic syndrome, anterior ischaemic optic neuropathy, normal tension glaucoma and asymmetric diabetic retinopathy which is less advanced ipsilateral to the stenosis.5,6 Table 9.1 Simplified classification of hypertensive retinopathy as proposed by Wong and Mitchell17 The lymph nodes are situated along the course of the lymphatic vessels. They are bean-shaped organs containing large numbers of leukocytes and phagocytes which filter out infectious and toxic material and destroy it. When infection occurs the nodes become enlarged and often painful and inflamed because of the production of anti-inflammatory lymphocytes and plasma cells.7 The lymphatic system of the head and neck is important in infections of the eye (Figure 9.1), particularly the preauricular lymph nodes which receive lymph from the upper eyelid, the outer half of the lower eyelid and the lateral canthus. They are located 1 cm anterior and slightly inferior to the tragus of the external ear at the temporomandibular joint. The submandibular lymph nodes lie in close proximity to the submandibular gland and drain lymph from the medial portion of the upper and lower eyelids, the medial canthus and the conjunctiva. They also drain lymph from the submental nodes that are located under the tip of the chin. The mental nodes also drain anterior aspects of teeth, tongue and lower lip so if an oral infection is present then they may be enlarged and this should not be mistaken for a sign of an ocular infection. The superior cervical nodes are located inferior to the ear and superficial to the sternocleidomastoid muscle. They receive lymph from the occipital nodes as well as the preauricular and post auricular nodes.7 The skin and orbicularis oculi muscles drain into the deep cervical nodes near the internal jugular vein (Figure 9.1). 1. Wash your hands thoroughly. 2. Stand in front of the seated patient. 3. Place the index and middle fingers of each hand in front of the tragus of the patient’s external ears. 4. Slowly move your fingers in a circular motion to slide the patient’s skin over the underlying bony structures of the temporo-mandibular joint and search for swollen lymph nodes. These will feel like a small pebble or bean under the patient’s skin. A slight depression of the joint is the normal finding. 5. Compare the right and left sides to help determine whether a swollen node is present. 6. If lymphadenopathy is found, its laterality (right, left or bilateral), size (big or small), mobility, warmth and tenderness should be determined. 1. All these lymph nodes are in the neck area (Figure 9.1) and should be palpated using the tips of your index, middle and ring fingers of both hands (the submental can be palpated using just one hand). Slowly move your fingers in a circular motion to slide the patient’s skin over the underlying bony structures and/or muscle and search for swollen lymph nodes, which will feel like a small pebble or bean under the patient’s skin. 2. In each case, if lymphadenopathy is found, its laterality (right, left or bilateral if appropriate), size (big or small), mobility, warmth and tenderness should be determined. 3. To assess the cervical nodes, palpate at the angle of the jaw and slowly move your fingers down, continuing to palpate to the base of the neck. 4. To assess the submandibular nodes, palpate just under the edge of the jawbone. 5. To assess the submental lymph nodes, palpate under the tip of the chin. 1. Viral conjunctivitis: visible preauricular lymphadenopathy often greater on the side of the more involved eye and accompanied by ear, nose and throat symptoms. 2. Severe bacterial lid conditions such as preseptal cellulitis or infection in the medial canthal region: preauricular or submental lymphadenopathy. 3. Parinaud’s oculoglandular conjunctivitis: often visible preauricular lymphadenopathy. 4. Chlamydial conjunctivitis or trachoma: preauricular lymphadenopathy. 5. Following the resolution of an ocular infection (several weeks). The presence of preauricular lymphadenopathy will therefore help rule in one of the above conditions when it is present although if it is not present the condition cannot be reliably ruled out.8
Physical examination procedures
9.1 Differential diagnosis information from other assessments
9.1.1 Observations and symptoms
9.1.2 General medical history and family history
9.1.4 Fundus examination
Grade of retinopathy
Retinal signs
Systemic associations
None
No detectable signs
None
Mild
Generalised arteriolar narrowing, focal arteriolar narrowing, arteriovenous nicking, opacity (‘copper wiring’) of arteriolar wall, or a combination of these signs
Modest association with risk of clinical stroke, subclinical stroke, coronary heart disease, and death
Moderate
Haemorrhage (blot, dot, or flame-shaped), microaneurysm, cotton-wool spot, hard exudate, or a combination of these signs
Strong association with risk of clinical stroke, subclinical stroke, cognitive decline, and death from cardiovascular causes
Malignant
Signs of moderate retinopathy plus swelling of the optic disc
Strong association with death
9.2 Lymphadenopathy in the head–neck region
9.2.1 The lymph nodes in the head and neck
9.2.3 Procedure for palpating the preauricular lymph nodes
9.2.4 Procedure for palpating the cervical, submandibular and submental lymph nodes
9.2.6 Interpretation
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Physical examination procedures