Perinatal Ophthalmology
Sharon Lehman
Antenatal Ophthalmology
Certain ocular conditions, such as dacryocele,1 congenital cataract,2 retinoblastoma,3 and orbital cyst4 may be detected on prenatal ultrasound. The family with a known genetic risk of ocular disease may have concerns about the future of the child’s health. Antenatal ophthalmology is the prenatal diagnosis and counseling of patients with or at risk for ophthalmologic abnormalities. Education of the family may occur prior to the stressful time of delivery. The family with a remote history of ocular disease may benefit from an update on current treatment options. Information about the disease and treatment options may aid in a family’s decision concerning early delivery for a life-threatening condition, such as retinoblastoma, found on prenatal ultrasound. The antenatal consultation allows for prompt evaluation and treatment after birth.
Some studies show an increased rate of chromosomal abnormalities in the population of infants born after in vitro fertilization. A rate of ocular abnormalities in infants born after in vitro fertilization was found to be 26% in one study. Abnormalities included refractive errors, anisometropia, and strabismus. Ocular structural abnormalities included Coats disease, congenital cataract, coloboma, hypoplastic optic nerve, optic atrophy, congenital glaucoma, and retinoblastoma. Early detection and treatment of some of these conditions is essential for a good outcome. Careful attention to the ocular structures during prenatal ultrasound and in the early postnatal period is indicated in high-risk groups.5
Pregnancy
The hormonal changes that occur during normal pregnancy produce ocular effects.6 Changes in levels of adrenocorticotropic hormone, corticoids, gonadotropic hormone, estrogens, progesterones, melanocyte-stimulating hormone, relaxin, and others affect salt and water retention, membrane properties, vascular integrity, pigmentation, and tissue laxity.
Intraocular pressure decreases during the second half of pregnancy, returning to previous levels approximately 2 months postpartum.7 This effect may be mediated through sex hormones affecting episcleral venous pressure or relaxin increasing facility of outflow.8,9,10 Ocular rigidity does not change.7
Corneal physiology is altered, yielding some edema with a minimal increase in thickness and secondary decrease in sensitivity.11,12 Refractive changes may occur. Because of these alterations, contact lenses may pose a particular problem.
Hormonally induced pigmentation produces melasma, also known as the mask of pregnancy. Krukenberg spindles may occur.13 Results of ocular tension outflow studies remain normal, and the spindles usually show resolution in late pregnancy. Whether or not these hormonal stimuli increase the incidence or alter the course of malignant melanoma of the choroid is unclear, and there is no evidence that termination of pregnancy is beneficial.14,15
Central serous retinopathy has occurred during successive pregnancies, with remission after delivery or abortion, suggesting a hormonal influence.16 Amniotic fluid embolization may produce retinal arteriolar occlusion.17
Ptosis may occur in association with normal pregnancy. The pathophysiology is unknown. In the unusual case that does not resolve, excellent surgical correction has been obtained with small levator resections.18
Spontaneous carotid-cavernous fistulas and pituitary hypertrophy with resultant visual field changes may occur during pregnancy and be etiologically related to it.6,19 The incidence of pseudotumor cerebri does not increase in pregnancy.20
Toxemia of pregnancy is a secondary type of diastolic hypertension with associated proteinuria and edema occurring during the third trimester. It is divided into a preeclamptic stage, without seizures, and an eclamptic stage, with seizures. Retinal changes may result in visual blurring and scotomata. Initial preeclamptic changes of segmental retinal arteriolar narrowing occur first in the nasal periphery and spread toward the optic disc, followed by generalized arteriolar attenuation.21 Retinal findings, however, fail to distinguish normal from mild preeclampsia.18 Retinal hemorrhages, cotton-wool spots, intraretinal edema, ischemic optic neuropathy, papilledema, choroidal and retinal detachment, and transient cortical blindness may occur, especially with eclampsia.22,23,24 The severity and progression of retinal arteriolar changes correlate with fetal mortality and have been used as a determinant for termination of pregnancy.25 Children of toxemic mothers may show retinal changes similar to their mothers’ retinal findings.26
The serous choroidal and retinal detachments are frequently bilateral. They may rarely occur without retinal arteriolar changes present.27 Leakage into the subretinal space may be related to choroidal vascular abnormalities, retinal pigment epithelial defects, or both.21,27,28,29 Reattachment usually occurs between 1 and 3 weeks postpartum, and the prognosis for visual return is favorable.30 Premature termination of pregnancy should be considered when retinal detachments are not responsive to medical control of toxemia.27
Diabetic retinopathy may be exacerbated by pregnancy.6,31 Background retinopathy should be carefully observed during pregnancy because a proliferative phase may ensue. Early photocoagulation for proliferative changes appears to improve the prognosis, especially if treatment precedes conception. Because the long-term visual prognosis does not appear altered and early termination of pregnancy may not affect the visual outcome, termination of pregnancy for proliferative retinopathy is seldom indicated.6,32
Therapy of any ocular condition during pregnancy must consider possible adverse fetal effects.33 These include abortifacient and teratogenic effects and certain transient physiologic alterations. An example of the latter is the lowering of fetal pseudocholinesterase levels through the transplacental action of echothiophate iodide eye drops used for the treatment of glaucoma. Data concerning transient physiologic effects of most therapeutic agents are few. All agents should be used cautiously and only with clear indications.
Teratogenicity
A teratogen is an agent that by acting during the embryonic or fetal period produces morphologic or functional malformations that become apparent postnatally. Most known teratogens are drugs, environmental chemicals, infectious agents, radiation, or deficiency states.
Approximately 3% to 5% of all neonates have a congenital anomaly requiring medical attention, and approximately one third of these conditions are life-threatening.34,35,36 Congenital anomalies are the single largest cause of infant mortality, the second largest cause of death between ages 1 and 4 years, and the third largest cause of death between ages 5 and 14 years.37 It is estimated that almost half of the children in hospitals were admitted because of prenatally acquired defects.34 The specific contribution of teratogenicity to this enormous morbidity and mortality is unknown.
The mechanism of action of teratogenic agents is varied.38 These agents may act directly on the mother by interfering with the supply of vital nutrients, disturbing enzyme systems, or altering placental function. More commonly, they cross the placenta and directly affect the embryo or fetus. Malformations may result from disturbances in cell interactions and differentiation, cell biochemistry, cell migration, and vascularization inhibition pathways. Malformation production is dependent not only on the teratogenic potential of a substance but also on the time of exposure, dose, maternal factors, and embryo or fetal susceptibility.
The most vulnerable period for malformation production is during organogenesis. Organogenesis of the human eye occurs between 24 and 40 days’ gestation.39 The developmental processes occurring at the time of insult are likely to be affected, producing sequential malformations. Thus, a rubella viremia in the first trimester often results in cataracts, glaucoma, and retinopathy.40 The eyes are usually spared in the congenital rubella complex if viremia occurs after major organogenesis is complete.41
Dose and the maternal immune state, patterns of enzyme detoxification, and placental status determine embryo and fetal exposure to these agents.42 Certain teratogens exhibit their effects at low doses, whereas a defined level is necessary for others.43 Except for radiation and radiomimetic agents, few direct data are available for humans.
Because it controls morphologic and biochemical development, the genotype of the embryo/fetus is a major determinant of teratogenic susceptibility.38 For example, thalidomide produced no teratogenic effects in rats and mice and was then marketed.44 Certain inbred strains of experimental animals have a much higher susceptibility to specific teratogens than do others of the same species.34,38 Perhaps similar multifactorial mechanisms are operative in the human phenytoin, trimethadione, and fetal alcohol syndromes, in which certain malformations are statistically increased yet their production is still not common.
Much of our knowledge of teratogenic agents comes from work with experimental animals. Because of biochemical, placental, and developmental differences, teratogenicity in animals does not imply teratogenicity in humans, nor does safe use in animals imply safe use in humans.35
Conditions necessary for establishing teratogenicity are convincing evidence of contact at critical developmental periods, reproducible epidemiologic data, and a consistent set of defects.45
The literature on teratogenicity is vast; a number of excellent reviews and catalogs are available.34,36,46,47,48,49,50,51,52 A detailed history of possible teratogenic exposure is indicated in the investigation of all birth defects. Any defect with a possible teratogenic etiology should be reported to the National Institute of Environmental Health Sciences’ Environmental Teratology Information Center. Their in-depth listings are available through the National Library of Medicine (Toxline, Toxlit, Toxnet).
Caution should be exercised in exposing any woman of childbearing age to potential teratogenic agents. Much of the vulnerable period of organogenesis has usually occurred before pregnancy is diagnosed.
Ocular Teratogens
A number of researchers have extensively reviewed drugs that are commonly administered to pregnant women and environmental ocular teratogenic chemicals to which pregnant women might be exposed.53,54,55
Suggestive Ocular Teratogenicity in Humans
Certain agents are suggestive ocular teratogens in humans but lack the criteria for the establishment of definite teratogenicity. The suggestion is based on known teratogenicity in experimental animals, with or without isolated reports in humans, and the known pharmacologic effects of these agents. Rare human exposure, nonuniformity of postexposure anomalies, or failure to document effects prospectively or statistically casts some doubt on the ocular teratogenicity of these agents in humans. Still, to risk teratogenic exposure, patients must have an absolutely vital need for the agent.
Suggestive ocular teratogens include phenothiazines, chloroquine, quinine, anticonvulsants, coumarin derivatives, cancer chemotherapeutic agents, and various “street drugs.” Maternal hyperthermia is also a suggestive teratogen. The Prospective Collaborative Perinatal Project revealed a greatly increased risk for cataracts after first-trimester boric acid, iodide, and phenylpropanolamine exposure; this association was previously unsuspected and not correlated experimentally. A greater than fivefold risk of coloboma formation after sulfisoxazole exposure was also noted.46
Phenothiazine, Chloroquine, and Quinine
In utero exposure to phenothiazine and chloroquine has resulted in retinotoxic effects in experimental animals,56,57 with case reports in humans.58,59 Chloroquine-induced anophthalmia and microphthalmia have been noted in rats. Quinine exposure in utero has been associated with congenital glaucoma and ganglion cell toxicity resulting in optic atrophy.60,61,62
Anticonvulsants
Anticonvulsant medication is necessary in approximately 1 in 200 pregnancies.66 Certain major malformations such as cleft lip and palate and congenital heart disease may be more frequent in offspring of epileptic women taking anticonvulsants. A host of other anomalies including ophthalmic abnormality are found.
A constellation of abnormalities has been found in infants exposed to phenytoin in utero.67,68,69 A pattern of abnormality sufficient to be ascribed to the phenytoin is found in 5% to 10% of infants exposed. Another 30% demonstrate some of the abnormalities.
Ophthalmologic findings include hypertelorism, epicanthic folds, ptosis, strabismus, persistent hyperplastic primary vitreous, optic nerve coloboma, and optic nerve hypoplasia.67,68,70,71,72,73
Glaucoma, prominent iris vessels, defective lacrimal apparatus, microphthalmia, retinoschisis, uveal and retinal coloboma, and retinal dysplasia have also been reported.71,73,74,75,76,77
Whether or not in utero exposure to phenytoin increases the likelihood of mental deficiency or learning disability remains unresolved.78,79 There may be an increased incidence of malignancies, especially of the neural crest, such as neuroblastoma.80
Epicanthus and V-shaped eyebrows are frequent features. Strabismus and myopia may be present.
The features of the fetal hydantoin and trimethadione syndromes have significant overlap. Similar anomalies have been reported with other antiepileptic drugs including primidone,81 carbamazepine,82 and valproic acid.83 This general increase in abnormalities may be contributed to by individual drugs, a common teratogenic mechanism of drug metabolites, a common genetic predisposition to epilepsy. and the malformation either through close linkage or etiologic mechanism, or deficiency states. Evidence that genetically determined levels of the enzyme epoxide hydrolase determine risk of anomaly helps explain many findings. This enzyme detoxifies common oxidative metabolites of antiepileptic drugs. Its level helps to explain individual susceptibility, familial recurrences, heteropaternal fraternal twin discordances, and the similarity of abnormality produced by various drugs.84
An alternative mechanism may involve interference in folic acid metabolism by valproate, carbamazepine, phenytoin, and phenobarbital.85,86
The risks to the fetus must be carefully explained to prospective mothers with epilepsy. It is hoped that enzyme assays will prove useful in better determining individual susceptibility to teratogenic effects.84 Because combination therapy is particularly hazardous, the minimal dose of a single control drug is recommended.68
Several of the ophthalmologic disorders found in children with fetal anticonvulsant exposure are potentially amblyogenic. Early ophthalmologic screening is suggested in this group of children.
Coumarin Derivatives
An association exists between the use of coumarin derivatives (Coumadin, dicumarol, sodium-warfarin, phenindione) in the first trimester of pregnancy and a phenocopy of the autosomal dominant Conradi-Hünermann syndrome, which is a form of chondrodysplasia punctata (dysplastic stippled epiphyses).87,88,89 As with Conradi syndrome, cataracts are reported.90
Midtrimester use leads to a high incidence of central nervous system abnormality including optic atrophy and hydrocephalus.90,91,92,93
Microphthalmos, posterior embryotoxon/mesodermal dysgenesis, and hypertelorism have also been reported.93,94,95 Exposure to warfarin between 8 and 12 weeks’ gestation resulted in an infant with the Dandy-Walker malformation, anterior segment dysgenesis (Peter anomaly), and agenesis of the corpus callosum.95
Cancer Chemotherapeutic Agents
Through their mechanism of action, cancer chemotherapeutic agents are potent teratogens.34 All classes of these agents, including antibiotics (actinomycin D), metaphase inhibitors (vincristine, vinblastine, colchicine), alkylating agents (nitrogen mustard, tretamine, busulfan, cyclophosphamide), the antimetabolites (6-amine-nicotinamide, 6-mercaptopurine, idoxuridine, azaserine, cytosine arabinoside, methotrexate), and procarbazine have been shown in experimental animals to result in major ocular abnormalities after in utero exposure. The abnormalities include anophthalmia, microphthalmia, and malformations of the lids, optic cup, cornea, lens, and retina.53,96,97,98,99 Although the agents are highly suggestive, the low fertility rate of women usually on multiple agents has made specific teratogenic detection difficult. Cloudy corneas were noted after in utero human exposure to busulfan (Myleran).100
Street Drugs
Abusers of street drugs (cocaine, narcotics, marijuana, benzodiazepines, barbiturates, lysergic acid diethylamide [LSD], amphetamines, and others) usually use multiple drugs of unknown potency and purity, have poor prenatal care and a high incidence of other health problems, and frequently are malnourished.101 The teratogenic potential of these drugs is therefore difficult to assess. For all these drugs, the issue of congenital malformation production has been raised but has not been substantiated.52,101
Cocaine use leads to a high incidence of abruptio placentae.102 Neonatal cerebral infarcts and dilated/tortuous iris vessels are reported.103,104 Microphthalmia with persistent hyperplastic primary vitreous in one eye and a retinopathy of prematurity (ROP)-like picture in the contralateral eye in a mother who smoked crack cocaine throughout pregnancy is reported.105 She additionally abused marijuana, alcohol, and tobacco.105
Benzodiazepine has been reported to produce characteristic facies, growth aberrations, and central nervous system abnormality resembling the fetal alcohol syndrome.106
LSD, an apparent potent mutagen, may have teratogenic potential resulting in ocular abnormalities.107 Abnormalities of lens development have been induced in mice.108 Anophthalmia, microphthalmia, optic atrophy, persistent hyperplastic primary vitreous (PHPV), retinal detachment, and retinal dysplasia with intraocular cartilage have been reported in humans.109,110,111
Hyperthermia
Maternal hyperthermia of 102.2°F (39°C) or greater lasting for 1 or more days during the first trimester may result in a pattern of central nervous system dysfunction and facial dysmorphogenesis.112,113 Mental deficiency with altered muscle tone and increased deep tendon reflexes is characteristic. Facial features include microphthalmia, micrognathia, midfacial hypoplasia, palatal and lip clefts, and ear anomalies. Microphthalmia was found in more than 50% of those exposed between 4 and 7 weeks’ gestation. Möbius syndrome has also been attributed to maternal hyperthermia.114
Definite Ocular Teratogenicity in Humans
Definite human ocular teratogenicity has been demonstrated for retinoids, thalidomide, folate antagonists, organic mercurials, ethanol, radiation, and infectious agents.
Retinoids
Long recognized as teratogenic in experimental animals, retinoids have now been shown to produce malformations in humans.115,116 Isotretinoin (Accutane) (13-cis-retinoic acid) is an oral synthetic vitamin A derivative useful in the treatment of cystic acne.117 It has been marketed in the United States since 1982. Exposure during the first trimester leads to a high incidence of anomaly.115,118 Affected infants typically exhibit defects of the central nervous system, head and face (particularly microtia/anotia, micrognathia, cleft palate, and a flat depressed nasal bridge), heart (especially cotruncal and aortic arch anomaly), thymus, and ocular structures.115,118 Central nervous system abnormality includes microcephaly, hydrocephalus/hydranencephaly, posterior fossa cysts, hypoplastic cerebellum, decreased cortical tissue, and calcifications.115,118,119,120,121 Ocular effects include microphthalmia, hypertelorism, antimongoloid slant of the palpebral fissures similar to Treacher Collins syndrome, and cortical blindness.118,119,121,122 Facial palsy is not uncommon.115
Another vitamin A congener, etretinate, introduced in the United States in 1986, is effective against psoriasis. Its teratogenic effects are similar to isotretinoin. Unlike isotretinoin, however, etretinate is stored in adipose tissue and released into the circulation for a long time even after treatment has been stopped. Teratogenic effects have been induced even 1 year after discontinuing the medication.123 No safe interval from the time of drug cessation has been established.
Thalidomide
The introduction of thalidomide led to a dramatic increase in a particular malformation complex; with withdrawal of this drug from the market, this complex has virtually disappeared. Few agents represent such clear-cut teratogens in humans. Thalidomide, introduced in 1956, was in widespread use in Europe but never released in the United States. In 1961, an increased incidence of severe limb deformities was recognized.124,125 The drug was withdrawn in the same year. Ocular involvement occurred in 25% of children exposed. Teratogenicity of thalidomide occurs between 20 and 36 days after fertilization. Ocular abnormalities include uveal colobomas, pigmentary retinopathy, microphthalmos, glaucoma, ptosis, facial nerve palsy, aberrant lacrimation, pupillary abnormalities, and strabismus. Rarer eye movement abnormalities such as Möbius and Duane syndromes are also reported.126
Folic Acid Antagonists
Folic acid antagonists are used as anticancer chemotherapeutic and antimicrobial agents. Members of this class have been shown to be potent abortifacients.127 Aminopterin (4-aminopteroylglutamic acid) produces proptosis and hypertelorism owing to abnormalities of cranial ossification.128,129,130,131 Methotrexate has produced similar abnormalities.132,133
Organic Mercurials
Organic mercurials enter the environment as industrial wastes and through their use as fungicides. After introduction into the environment, concentration in seafood and grain-eating animals presents potential toxic sources. Toxic doses produce a neurologic disorder (Minamata disease) characterized by visual field constriction, decreased visual acuity leading to blindness, tremors, deafness, dementia, and death.134,135,136 In utero exposure produces a similar condition, often of greater severity and permanence than that found in the mother.137,138,139,140 Blindness has resulted from in utero exposure.141
The commonly used preservative thimerosal is a mercury-containing fungicide. Very-high-dose thimerosal, typically applied to pregnant rabbits, resulted in fetal tissue accumulation without morphologic teratogenic effect.142
Ethanol
Ethanol used excessively during pregnancy results in a fetal malformation complex known as fetal alcohol syndrome (Figs. 39-1, 39-2, 39-3).143,144,145 Important criteria for diagnosis include low birth weight, growth retardation, central nervous system dysfunction, microcephaly, and characteristic facies.
 Figure 39-1. Infant with severe microphthalmos secondary to fetal alcohol syndrome. |
 Figure 39-2. Computed tomography scan of infant with severe microphthalmos secondary to fetal alcohol syndrome. |
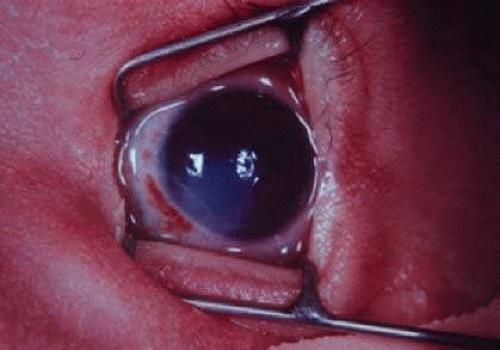 Figure 39-3. Segmental corneal opacification consistent with the Peter anomaly seen in fetal alcohol syndrome. |
Problems in development range from behavior and learning difficulties with normal intelligence to significant mental retardation. The fetal alcohol syndrome accounts for a significant percentage (8% to 17%) of children with developmental delay.146,147
The incidence of the full syndrome varies in the range of 1:300 to 1:750 of all live births.148 In children born to drinking alcoholic mothers, the incidence of the full syndrome is in the range of 30%.147,149 These drinking alcoholic mothers were those who reported drinking 1 ounce or more of absolute alcohol per day during pregnancy or before pregnancy recognition or reported drinking 45 or more drinks per month.149 A lesser percentage of children were affected among mothers who drank less than this. No level of alcohol consumption is known to be safe.
That the full-blown syndrome occurs in a minority of significantly exposed infants suggests genetic influences in susceptibility or detoxification. Whether alcohol itself or an oxidative metabolite such as acetaldehyde is the direct teratogen is unclear.148
The spectrum of ocular findings in the fetal alcohol syndrome suggests a risk of harmful effects on the eyes at any time in gestation.147
Horizontally short palpebral fissures constitute a hallmark of this condition.150 Palpebral fissure size in Hispanics and blacks at 3 days of age was found to be slightly larger than in whites.151 The horizontal shortening of the palpebral fissures is primarily the result of a marked increase in the intercanthal distances between the medial canthi with normal interpupillary distance (primary telecanthus).152
Other frequent (between one quarter and one half affected) ocular features include blepharoptosis, epicanthal folds, strabismus, retinal vascular tortuosity (both arterial and venous), and optic disc hypoplasia.147,152,153,154
Less frequent ocular findings are myopia, long eyelashes, microphthalmia, anterior segment dysgenesis (including unilateral/bilateral Peter and Axenfeld anomalies), steep corneal curvature, cataract (may be unilateral), and persistent hyaloids.147,152,153,154
A mouse model suggests that the anterior segment anomalies result from acute insult to the optic primordia at a very specific time that corresponds in humans to the third week after fertilization.155
Radiation
Radiation is the best-studied teratogen. In utero radiation exposure of experimental animals produces cataracts, microphthalmia, anophthalmia, and coloboma in a high percentage of cases when 10 to 100 rad are delivered during sensitive development periods. These data have been summarized by Brent.156 Retinal cellular deficiency results from in utero loss of radiosensitive neuroblasts in monkeys exposed to 200 to 300 rad.157
Knowledge of the human teratogenicity of radiation has been obtained after atomic bomb explosions and therapeutic or diagnostic x-ray exposure. No increased incidence of ocular abnormalities (including cataracts) occurred among in utero survivors of the atomic explosions in Hiroshima and Nagasaki.158
Therapeutic radiation of 500 rad or more in the first trimester (especially 3–11 weeks’ gestation) is associated with frequent microphthalmia, pigment degeneration of the retina, and cataracts.159 Because of these effects, therapeutic abortion has been recommended for fetuses receiving as little as 10 rad of radiation between the 18th day and the end of the first trimester.157
Infections
Rubella, cytomegalovirus, toxoplasmosis, mumps, Venezuelan equine encephalitis virus, syphilis, parvovirus B19, varicella, and perhaps herpes simplex and the acquired immunodeficiency syndrome162 produce human ocular teratogenicity.
Teratogenicity of Ocular Therapeutic Agents
Ophthalmologists must be aware of the teratogenic potential of any therapeutic agent prescribed for women of childbearing age. Fortunately, few agents likely to be used in the treatment of ocular disorders have known teratogenic potential in humans. Topical ocular instillation of substances with teratogenic potential has resulted in abnormalities in experimental animals.163,164
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


