CHAPTER 115 Penetrating and Blunt Trauma to the Neck
In the neck, multiple vital structures are vulnerable to injury in a small anatomic area and are not protected by bone. Such vital structures of the neck can be divided into four groups: the air passages (trachea, larynx, pharynx, lung); vascular (carotid, jugular, subclavian, innominate, aortic arch vessels); gastrointestinal (pharynx, esophagus); and neurologic (spinal cord, brachial plexus, peripheral nerves, cranial nerves [CNs]). Signs or symptoms listed in Box 115-1 should alert the otolaryngologist that injury to any of these structures has occurred.
Box 115-1 Signs and Symptoms of Penetrating Neck Trauma
From Stiernberg C, Jahrsdoerfer RA, Gillenwater A, et al. Gunshot wounds to the head and neck. Arch Otolaryngol Head Neck Surg. 1992;118:592.
Physical Properties of Penetrating Objects
Knowledge of the physical properties and ballistics of the penetrating object can help determine a management plan and predict the risk of injury. The location of penetration also predicts risk and helps in planning for management.1 The magnitude of injury is determined by the kinetic energy that is transferred from the projectile to the target tissue: KE =  M(V1 − V2)2. KE is the kinetic energy of the projectile, M is the mass of the projectile, V1 is the initial velocity on contact, and V2 is the exit velocity. Thus differences of projectile velocity transform into kinetic energy by the second power.
M(V1 − V2)2. KE is the kinetic energy of the projectile, M is the mass of the projectile, V1 is the initial velocity on contact, and V2 is the exit velocity. Thus differences of projectile velocity transform into kinetic energy by the second power.
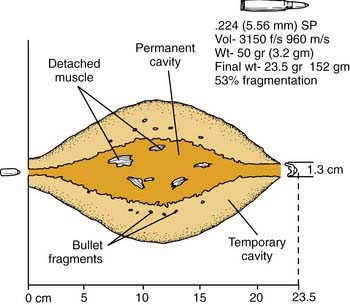
Rifle
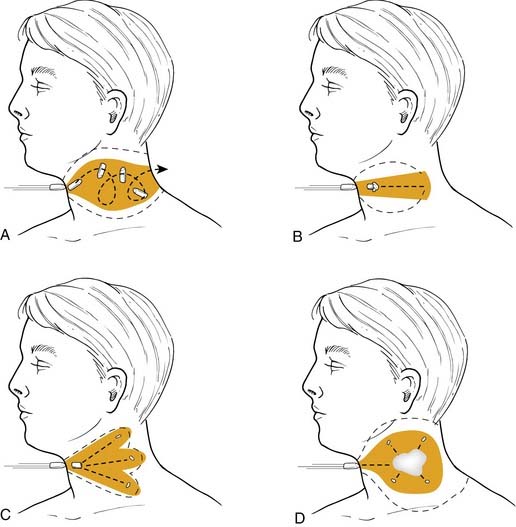
Most military rifles have a muzzle velocity of 760 m/s. High-velocity missiles (>610 m/s) not only tear tissue but transmit energy to surrounding tissue. A cavity of up to 30 times the size of the missile may be created and pulsate over 5 to 10 ms, with several waves of contraction and expansion of the tissue (Fig. 115-1).2 This may explain the finding of a punctured viscus without direct penetration and should alert the surgeon to examine the trachea and esophagus, even when a bullet wound is 2 inches away (Fig. 115-2).
Shotguns
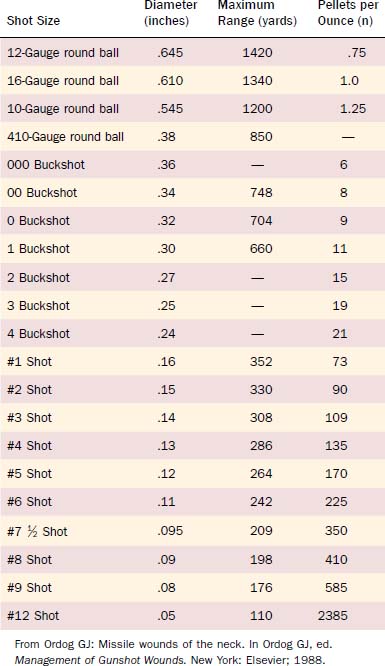
The severity of shotgun wounds is largely dependent on the distance between the weapon and the victim, the type of weapon used, and the size of the projectile (shot). Pellets tend to scatter as they travel on the basis of the distance to impact and the interior muzzle diameter (choke) of the shotgun. At close range the entire charge can act like a single missile with a KE similar to a high-velocity bullet.3 At further distances, birdshot pellets scatter and act as multiple individual missiles. With larger pellets such as buckshot, significant injuries can occur from individual pellets up to 150 yards away with a standard-length barrel. A sawed-off shotgun leads to early spraying of the shot. Shotguns are low-velocity weapons (muzzle velocity of 300 m/s).
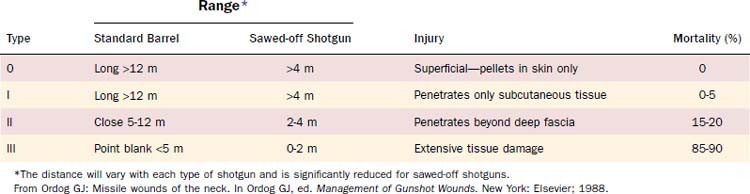
Birdshots are pellets with a diameter less than or equal to 3.5 mm (0.13 inch) and are categorized as No. 4 shot or smaller. Buckshots have a diameter greater than 3.5 mm and have a greater range, causing significant injury up to 150 meters. This is in contrast to birdshots, which have a 12-m maximum range of serious injury (Tables 115-1 and 115-2). Each pellet injury from a buckshot blast is similar to a bullet injury from a handgun. Buckshot wounds are usually more serious than handgun bullet wounds because of the number of missiles involved.
Knife and Stab Injuries
Knife, ice-pick, cut-glass, or razor-blade injuries usually proceed along more predictable pathways. However, what appears to be a single-entry wound may be from multiple stab wounds. The history of the attack may be of some help to the physician in determining whether the blow was overhand or underhand, whether both the attacker and the recipient were standing, and other similar details. Compared with gunshot wounds to the neck, cervical stab wounds have a higher incidence of subclavian vessel laceration.4 This is because stabbings to the neck often occur in a downward direction with the knife slipping over the clavicle and into the subclavian vessels.5 In gunshot wounds the direction of the projectile is more perpendicular to the neck; thus the clavicle can protect the subclavian vessels. In regard to spinal injuries, neck stab wounds have a lower incidence than cervical bullet wounds.5
Mandatory versus Elective Exploration
For the stable patient, the choice of management remains controversial: either mandatory exploration for all penetrating neck wounds or selective exploration with observation. Retrospective studies have supported both mandatory surgical exploration and selective surgical exploration.6,7 For the selective surgical approach, it is emphasized that the clinical status of the patient should be monitored closely by frequent observation and medical examination using diagnostic radiology and surgical endoscopy. In civilian injury this is often possible, but in times of war or civilian catastrophe, resources such as radiography and observation beds may not be available for large numbers of casualties.
Until World War II, the mortality of penetrating neck wounds ranged from 7% to 15%. By the end of the Vietnam War, it was reduced to 3% to 6% (Table 115-3).7 However, mortality remains high if major vascular structures (carotid or subclavian arteries) or the cervical spinal cord is injured. During the Vietnam War, it was customary to explore all patients with penetrating neck wounds below the platysma layer under general anesthesia, regardless of preoperative findings. The idea of mandatory exploration was also advocated by Fogelman and Steward in 1956 for civilian injuries. This philosophy was followed until the mid-1980s by most general trauma centers in large cities in the United States. However, it was realized that in many instances significant injuries to major structures did not occur. This reasoning led some surgeons to follow a more selective approach for these injuries. However, advocates for mandatory exploration believe that exploration has time-proven success. Each of the proponents gives arguments that support their views, both medically and economically (Table 115-4).
Table 115-3 Mortality of Penetrating Neck Trauma in Wartime and Current Civilian Practice
| Incident | Injuries (n) | Mortality (%) |
|---|---|---|
| Civil War | 4114 | 15 |
| Spanish-American War | 188 | 18 |
| World War I | 594 | 11 |
| World War II | 851 | 7 |
| Current civilian practice | n/a | 3-6 |
n/a, not available.
From McConnell D, Trunkey D. Management of penetrating trauma to the neck. Adv Surg. 1994;27:97.
Table 115-4 Mandatory versus Selective Management of Neck Wounds
| Consideration | Mandatory | Selective |
|---|---|---|
| Diagnosis | Potential life-threatening injuries can be missed by the preoperative workup. | Most major injuries can be diagnosed preoperatively; routine exploration can miss some injuries. |
| Skill and resources |



