Purpose
To describe the clinical characteristics of ciliary body tumors, surgical outcomes, and factors associated with poor visual outcome and metastasis.
Design
Retrospective case series.
Methods
Medical records of 27 patients with ciliary body tumors who underwent partial lamellar sclerouvectomy in a single-center setting (Seoul, South Korea) were reviewed. Surgical outcomes were reviewed, and clinical characteristics were analyzed with respect to visual prognosis and globe retention rate.
Results
Tumors were diagnosed histopathologically as benign in 8 (30%) cases and as melanoma in 19 (70%) cases. Patients had a median age of 48 years. The median follow-up was 3.5 years (range, 0.5 to 6 years). The tumors had a median diameter of 11 mm and a median thickness of 9 mm. The globe was retained in 20 (74%) eyes, with visual acuity of 20/400 or better in 13 (48%) eyes and 20/40 or better in 6 (22%) eyes. Choroidal involvement of tumor ( P = .003), larger diameter of tumor ( P < .001), and thicker tumor ( P < .001) were associated with poor visual outcome. Local recurrence ( P = .003) and presence of epithelioid cells ( P = .040) were predictive factors for metastasis in melanoma patients. Kaplan-Meier estimates of metastasis-free survival at 3 and 5 years for melanoma patients were 82% and 55%, respectively.
Conclusions
Partial lamellar sclerouvectomy is a reasonable primary therapeutic option in ciliary body tumors, and good visual prognosis is expected in selected cases.
Iridocyclectomy for removing ciliary body tumor is a well-known surgical procedure today. The first such attempt seems to be been by Zirm, who reported a local excision of melanosarcoma of the ciliary body in a 25-year-old woman in 1911. Local excision of cilliary body tumor that involves choroid is technically more challenging because of less accessible surgical location and relatively larger tumor size. In 1961, Stallard illustrated a technique for removing a choroidal melanoma by creating a lamellar scleral flap, and in 1966 he reported 2 cases managed by this technique, which he called partial choroidectomy . Since the 1960s, many techniques and the results of local resection of ciliary body tumors with or without choroidal involvement have been reported using various descriptive terms, including partial lamellar sclerouvectomy , transscleral local resection , eye wall resection , and block excision . Local resection of uveal melanoma is not performed widely because of technical difficulties and fears of iatrogenic tumor dissemination. However, it is becoming less controversial because of the growing consensus that local resection does not adversely affect the survival of melanoma patients. In addition, surgical and anesthetic advances have improved ocular outcomes.
Reports on ciliary body tumors in Asian patients are very limited, mainly because of the rare incidence of uveal melanoma in pigmented races. In this report, we present our experience with ciliary body tumors of various kinds that were managed by local resection using a partial lamellar sclerouvectomy in a Korean population. We present clinical characteristics of the tumors and their surgical outcomes and identify prognostic factors.
Methods
This retrospective study was approved by the Institutional Review Board of the Yonsei University College of Medicine before the review of data began and adhered to the tenets of the Declaration of Helsinki. A review of medical records was performed on all patients with tumors of the ciliary body with or without iris or choroidal extension, or both, who underwent partial lamellar sclerouvectomy in the Ophthalmology Department of Yonsei University College of Medicine (Seoul, South Korea) between September 2005 and August 2011.
Patient selection was determined by a careful assessment of ocular and systemic findings and the preference of the patient. In general, local resection was considered if ciliary body tumors were less than 15 mm in largest diameter and did not extend 7 mm posterior to equator. However, larger tumors were resected on occasions. In all cases, enucleation and radiotherapy were mentioned as treatment options. There were 4 patients with ciliary body melanoma who underwent primary enucleation because of large tumor size or patient preference. These patients are not included in this study. During the study period, no patient with ciliary body melanoma underwent radiotherapy alone.
Surgical Technique
All surgeries were performed by a single surgeon (S.C.L). In general, surgery followed previously described techniques. In brief, general anesthesia was used to keep the systemic blood pressure low. After the conjunctival peritomy was made and the tumor was localized using indirect ophthalmoscopy and transillumination, a lamellar scleral flap was prepared carefully to be approximately 80% to 90% of the scleral thickness approximately 5 mm outside the tumor margin. Sometimes, limited space only permitted a 3- to 4-mm tumor margin. The flap was hinged posteriorly for tumors extending posterior to the ora serrata and anteriorly at the limbus if the tumor was small and extended anteriorly to the iris root. For large tumors, the globe was decompressed using limited pars plana vitrectomy. An incision was made through the inner scleral fibers around the tumor to expose the uveal tract. The tumor was removed along with dissected inner scleral fibers and normal uveal tissues. The scleral flap then was sutured back to its original position.
Any retinal tear was managed with vitreoretinal surgery and silicone oil tamponade, combined with lensectomy in cases where cataract or lens damage was present. Adjunctive brachytherapy using a 20-mm 106 Ru plaque was used after sclerouvectomy in melanoma cases that were first seen after October 2006, when plaque radiotherapy became available in our institution. An apex dose of approximately 100 Gy was delivered 1 mm from the inner surface of the sclera during brachytherapy. When a diagnosis of uveal melanoma or malignancy was clinically uncertain, adjunctive brachytherapy was delayed until pathologic confirmation. However, in this study cohort, no tumor involved delayed brachytherapy. Surgical clearance of uveal melanoma was considered adequate if normal uveal tissue was present beyond the tumor margin or inadequate if tumor was present at the resection margin.
Statistical Analysis
The results were analyzed using SPSS software version 15.0 (SPSS Inc, Chicago, Illinois, USA). The Mann–Whitney U test was used to compare clinical characteristics between benign and malignant tumors. A linear regression test was applied to determine clinical characteristics correlated with final visual acuity and development of rhegmatogenous retinal detachment. The log-rank test was used to compare survival according to each baseline risk factor. Kaplan-Meier survival curves were used to estimate the rate of metastasis-free survival. A P value less than .05 was considered to be statistically significant.
Results
Between September 2005 and August 2011, a total of 27 patients underwent partial lamellar sclerouvectomy for ciliary body tumors, which were histopathologically benign in 8 (30%) cases and malignant in 19 (70%) cases. Benign tumors on histopathologic examination included melanocytoma (2 cases), adenoma of the nonpigment epithelium of the ciliary body (2 cases), adenoma of the pigment epithelium of the ciliary body (1 case), schwannoma (1 case), leiomyoma (1 case), and medulloepithelioma (1 case). Of 8 benign cases, 3 (38%) cases have been described previously. All 19 cases of malignant tumors were melanoma, including 5 (26%) spindle-cell type, 11 (58%) mixed-cell or epithelioid-cell type, and 3 (16%) tumors with no reported cell type. Of 19 melanoma cases, 12 (63%) cases had an adequate surgical clearance and 7 (37%) cases had inadequate surgical clearance. Fine-needle aspiration biopsy was performed in 2 cases of melanoma and 1 case of schwannoma before sclerouvectomy. Using fine-needle aspiration biopsy, definitive diagnosis was made in melanoma cases, but not in the schwannoma case.
The median age of patients at the time of surgery was 48 years (range, 11 to 83 years). Patients with benign tumors were younger (31 vs 54 years; P = .025). There were 14 women (52%). The median follow-up was 3.5 years (range, 0.5 to 6 years). Demographic information of patients at presentation is listed in Table 1 .
| Feature | Total (n = 27) | Benign (n = 8) | Malignant (n = 19) |
|---|---|---|---|
| Sex, no. (%) | |||
| Male | 13 (48) | 3 (34) | 10 (53) |
| Female | 14 (52) | 5 (66) | 9 (47) |
| Median age (range), y | 48 (11 to 83) | 31 (11 to 83) | 54 (21 to 73) |
| Involved eye, no. (%) | |||
| Right | 14 (52) | 5 (66) | 9 (47) |
| Left | 13 (48) | 3 (34) | 10 (53) |
| Associated systemic findings, no. (%) | |||
| Hypertension | 1 (4) | 0 | 1 (5) |
| Previous pulmonary tuberculosis | 5 (18) | 1 (12) | 4 (21) |
| Thyroid cancer | 1 (4) | 1 (12) | 0 |
| Atopy dermatitis | 1 (4) | 1 (12) | 0 |
| None | 19 (70) | 5 (64) | 14 (74) |
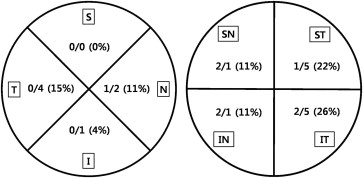
The tumor was located in the inferotemporal quadrant in 7 (26%) cases and in the supertemporal quadrant in 6 (22%) cases ( Figure 1 ). Tumor diameter ranged from 2.0 to 16.5 mm (median, 11 mm). Tumor height ranged from 1.5 to 13 mm (median, 9 mm). Tumors that were smaller in diameter and thickness generally were benign ciliary body lesions with iris extensions. There were 5 (19%) such tumors requiring a partial lamellar scleroiridocyclectomy. The tumor was located primarily in the ciliary body, with iris and choroidal extension in 6 (22%) patients requiring a partial lamellar scleroiridocyclochroidectomy. In 16 (59%) patients, the tumor was located in both the ciliary body and adjacent choroid, requiring sclerochoroidectomy ( Table 2 ). Partial lamellar sclerouvectomy was followed by vitrectomy with silicone oil tamponade in 22 (81%) cases because of intraoperative vitreous hemorrhage, retinal tear, retinal detachments, or vitreous prolapse with the fear of postoperative retinal detachment.
| Feature | Total (n = 27) | Benign (n = 8) | Malignant (n = 19) | P Value a |
|---|---|---|---|---|
| Median visual acuity (range), logMAR | ||||
| Initial | 0.5 (0 to 2) | 0.15 (0 to 1.3) | 0.7 (0 to 2) | .119 |
| Final | 0.9 (0 to 3) | 0.2 (0 to 2) | 1.3 (0.5 to 3) b | .031 |
| Median follow-up (range), y | 3.5 (0.5 to 6.0) | 1.7 (0.5 to 6.0) | 3.7 (1.0 to 5.0) | .095 |
| Median tumor size (range), mm | ||||
| Largest basal diameter | 11.0 (2.0 to 16.5) | 5.2 (2.0 to 11.0) | 12.5 (2.7 to 16.5) | <.001 |
| Height | 9.0 (1.5 to 13) | 4.2 (1.5 to 8.0) | 10.0 (5.0 to 13.0) | <.001 |
| Surgery, no. (%) | ||||
| Scleroiridocyclectomy | 5 (19) | 5 (63) | 0 | |
| Scleroiridocyclochoroidectomy | 6 (22) | 2 (25) | 4 (21) | |
| Sclerocyclochoroidectomy | 16 (59) | 1 (12) | 15 (79) | |
| Combined PPV | 7 (26) | 3 (37) | 4 (21) | |
| Combined PPV + cataract surgery | 15 (55) | 1 (12) | 14 (52) | |
| Adjunctive 106 Ru brachytherapy | 14 (52) | 0 | 14 (74) | |
| Secondary enucleation | 7 (26) | 0 | 7 (37) | |
| Systemic metastasis, no. (%) | 5 (19) | 0 | 5 (26) | |
| Pathologic features, no. (%) | ||||
| Melanoma | 19 (70) | 0 | 19 (100) | |
| Melanocytoma | 2 (7) | 2 (26) | 0 | |
| Adenoma, NPCE | 2 (7) | 2 (26) | 0 | |
| Adenoma, PCE | 1 (4) | 1 (12) | 0 | |
| Schwannoma | 1 (4) | 1 (12) | 0 | |
| Leiomyoma | 1 (4) | 1 (12) | 0 | |
| Medulloepithelioma | 1 (4) | 1 (12) | 0 |
a Mann–Whitney U test between benign tumors and malignant tumors.
Postoperative occurrences of adverse events were subdivided into 3 periods, namely intraoperative (occurring at the time of surgery and the first 24 hours after surgery), early (between 24 hours and 3 months), and late (after 3 months; Table 3 ). Vitreous hemorrhage was the most common adverse event occurring during or with the first 24 hours after surgery in 11 (41%) cases. Hyphema also was present commonly during the postoperative period in 8 (30%) cases. Retinal break and detachment of the retina occurred in 8 (30%) cases during or with the first 24 hours after surgery and were treated with vitrectomy and silicone oil tamponade. During the early period, 4 (15%) cases of retinal detachment, proliferative vitreoretinopathy, or both occurred and underwent vitrectomy and silicone oil tamponade. Of these 4 cases, 1 patient had undergone surgery for intraoperative retinal detachment. During the late postoperative period, retinal detachment with proliferative vitreoretinopathy occurred in 2 (8%) patients who previously had undergone vitrectomy and silicone oil tamponade for intraoperative and early postoperative retinal detachments. They were not treated because further surgery was not deemed visually or anatomically beneficial. Retinal detachment was associated with tumor extension over ora serrata ( P = .043; R 2 = 0.167). Cataract developed in 4 (15%) cases, 2 during the early postoperative period and 2 during the late postoperative period. Preretinal fibrosis—usually in the area of the resection—macular pucker, or both were present in 5 (19%) cases in the late postoperative period. No surgery was performed for these cases.
| Occurrence | Intraoperative (< 24 h) | Early (24 h to 3 mos) | Late (> 3 mos) |
|---|---|---|---|
| Vitreous hemorrhage | 11 (41%) | 1 (11%) | 0 |
| Hyphema | 8 (30%) | 0 | 0 |
| Retinal detachment | 8 (30%) | 4 (15%) | 2 (8%) |
| Choroidal detachment | 1 (4%) | 0 | 1 (4%) |
| Retinal/subretinal hemorrhage | 3 (11%) | 0 | 0 |
| Cataract | 0 | 2 (8%) | 2 (8%) |
| Epiretinal membrane | 0 | 0 | 5 (19%) |
| Corneal opacity | 0 | 0 | 1 (4%) |
| Sympathetic ophthalmia | 0 | 0 | 1 (4%) |
| Elevated intraocular pressure | 0 | 0 | 1 (4%) |
| Neovascular glaucoma | 0 | 0 | 1 (4%) |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


