Other Uses of Contact Lenses
Zoraida Fiol-Silva
Harold A. Stein
Although we generally think of contact lenses as cosmetic, there are numerous other uses for them. Therapeutic contact lenses constitute an important segment of the contact lens wearing population. Therapeutic lenses can be soft or rigid, conventional or special design, clear or painted, and daily or extended wear. When therapeutic lenses, most physicians think of bandage lenses, typically for the treatment of symptomatic corneal surface pathology. Although bandage lenses constitute an important segment of the therapeutic lens population, we must also think of special design rigid lenses used for the treatment of keratoconus disease, rigid lenses used in patients with irregular astigmatism of various etiologies, hybrid lenses (soft and rigid combined), occluder soft lenses, painted lenses, (numerous uses) and others.
Technologic advances in both contact lens materials and designs have made possible the development of new and broader contact lens alternatives for the treatment of patients with several anterior segment conditions. Newer alternatives provide our patients not only more but better lens choices.
The most common uses of therapeutic lenses include: bandage lenses, keratoconus design lenses, rigid lenses for the correction of irregular astigmatism of various etiologies, hybrid lenses, and painted lenses (Fig. 1).
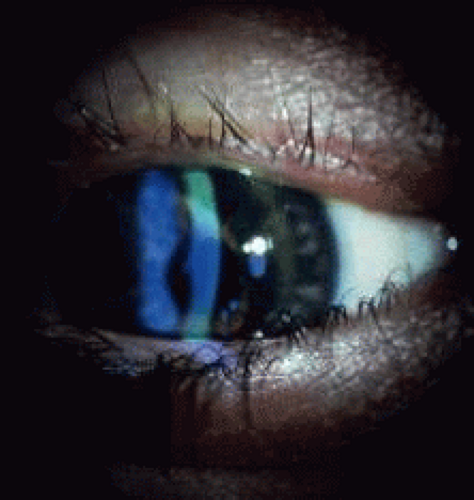 Fig. 1. Keratoconus patient fit with Nicone RGP lens. |
BANDAGE LENSES
Bandage lenses are a group of soft, thin, highly oxygen permeable lenses of various levels of water content that are typically fit loosely over the cornea for various therapeutic purposes. Although years ago several lenses were in the market exclusively for this purpose, today disposable lenses are most commonly used. The most common uses of bandage lenses are epithelial erosions, bullous keratopathy, filamentary keratitis, trichiasis, alkali burns, penetrating corneal wounds, leaking blebs after trabeculoplasty, Simmons compression shells, and postsurgical wound gaps with flat anterior chambers.
EPITHELIAL EROSIONS
Thin, highly oxygen permeable, (hydrophilic) soft lenses have been used very successfully in the treatment of epithelial corneal erosions. The purpose of the lens is not only to manage pain but also to assist in the healing process of the corneal surface. The lens assists surface healing by protecting the loose epithelium from the mechanical trauma of the eyelid, as well as by preventing adherence of the epithelium to the underlying cornea.
The authors recommend using a highly oxygen permeable, lower water content lens. A tight-fitting lens should be avoided to prevent corneal edema or other complications. Easy tear flow under the lens is very important, and the frequent use of artificial tears is highly recommended. A dry lens will actually make the condition worse.
BULLOUS KERATOPATHY
Pain management is the most valuable use of a bandage lens in patients with bullous keratopathy, although improving visual acuity is often possible and successfully accomplished as well.
Although a tight-fitting lens will likely cause further problems and complications, a very loose-fitting lens should also be avoided because it can actually worsen the symptoms resulting from the constant mechanical trauma of the lens over the corneal surface. Copious use of lubricants or artificial tears is strongly recommended.
FILAMENTARY KERATITIS
Patients with filamentary keratitis also greatly benefit from the use of a bandage soft lens. Regardless of the clinical reason for the filaments, placement of a bandage soft lens will typically help within a relatively short period. In most patients the filaments disappear within a week. Removal of the lens is advocated after the filaments disappear. The frequent use of lubricants is also very important in these patients, both during lens wear and after removal of the lens. A thin, low water content lens is also recommended in these patients.
TRICHIASIS
Although removal of the misdirected eyelashes is the preferred treatment of trichiasis, a soft bandage lens offers valuable temporary relief for this condition, particularly when the misdirected lashes cause direct trauma to the cornea.
Bandage lenses offer protection to the cornea but not the conjunctiva. It is equally important to protect the conjunctiva from the damaging effects of chronic, repeated trauma by the abnormal eyelids and eyelashes. Although patients without corneal involvement are not typically as symptomatic, care should be taken to avoid long-term deformities.
ALKALI BURNS
Bandage lenses have proven to be very helpful in promoting re-epithelialization of the cornea in patients with chemical burns. Although the contact lens will not prevent many of the complications of an alkali burn such as symblepharon and conjunctival overgrowth, they will assist in corneal epithelial healing and pain management.
As in most situations in which a bandage lens is used, a thin, highly oxygen permeable lens is recommended and lubrication is very important.
PENETRATING CORNEAL WOUNDS
Bandage soft lenses have been used very successfully in the treatment of patients with small penetrating corneal wounds that have clean edges (without irregularities) and good apposition, without iris prolapse or incarceration. In most instances these are trauma patients (Fig. 2), although the perforations may be seen in some postsurgical patients such as after refractive surgery, radial keratotomy (RK).
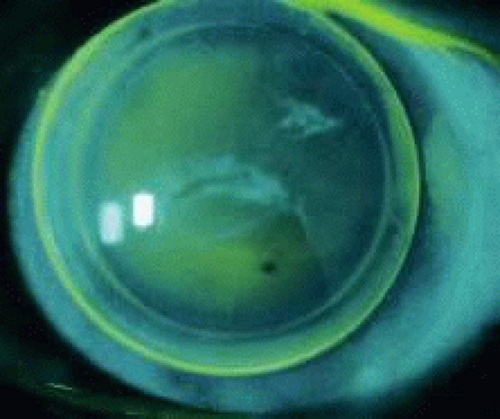 Fig. 2. Posttrauma patient with resultant corneal scar and aphakia fit with RGP lens. |
The lens provides tamponading of the wound and thus assists in the restoration of the anterior chamber and promotes wound healing. Bandage lenses have also been used after corneal transplantation in patients who have a small wound gape, particularly when resuturing is not possible or is complicated.
GLAUCOMA SURGICAL PROCEDURES
Through the years, bandage lenses have been very helpful in some glaucoma procedures. Flat anterior chambers secondary to a wound leak from a small perforation on the bleb can be resolved with the use of a large-diameter, thin, low water content soft lens. In these cases, the lens will provide a tamponading effect that will facilitate wound closure and healing, thus allowing the reformation of the anterior chamber and providing protection from infection and other complications. In some instances, tissue adhesive has been used very successfully with the bandage lens.
A bandage lens is helpful when the Simmons compression shell is used. In these cases the lens is placed between the shell and the cornea to offer protection from the mechanical trauma of the shell against the cornea.
SPECIALTY LENSES
Other than the traditionally recognized bandage soft lenses, there are other therapeutic uses for contact lenses. Some are soft lenses; many are rigid lenses, typically rigid gas permeable (RGP) lenses. Specialty lenses are mostly used in situations in which neither spectacles nor a conventional lens would improve visual acuity or relieve patients from debilitating symptoms. Some examples are keratoconus, after corneal transplantation, irregular astigmatism of various etiologies, color deficiency (particularly red-green), diplopia, anisometropia, cosmetically unsightly eyes, iris abnormalities with resultant monocular diplopia, photophobia, glare, halos, or decreased vision.
KERATOCONUS DESIGN LENSES
Patients with keratoconus disease comprise a significant portion of the population of therapeutic contact lens wearers (Figs. 3 and 4). Although patients with early forms of the disease may obtain reasonably good visual acuity with either spectacles or conventional soft lenses, most patients require special design, rigid lenses to obtain functional vision. Eliminating the need for corneal transplantation would be ideal. Because of the high degree of irregular astigmatism and the nature and location of the ectasia that patients with keratoconus have, conventional lens fitting does not provide these patients with either an adequate fit or reasonable comfort or visual acuity.
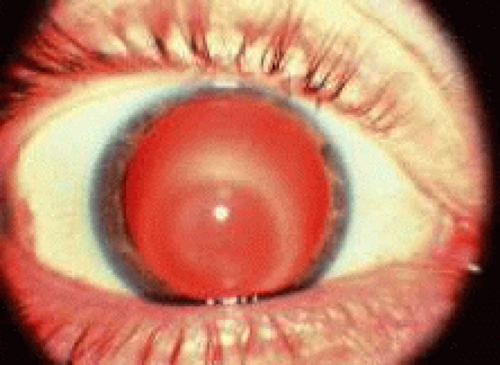 Fig. 3. Keratoconus. Corneal ectasia outline using retro illumination. |
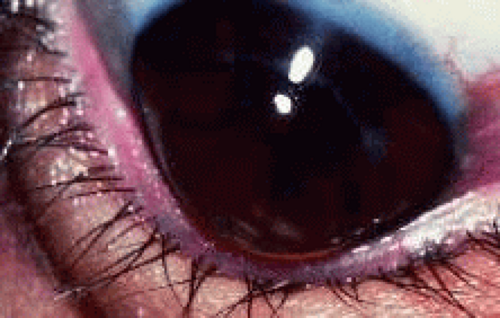 Fig. 4. Keratoconus—Munson’s sign. |
The purpose of a contact lens in patients with keratoconus is to cover the irregular astigmatism and the distorted anterior surface of the ectatic cornea, thus providing a regular, spherical optical surface in front of the eye. The lens would effectively restore the smooth optical properties of the cornea (Figs. 5 and 6).
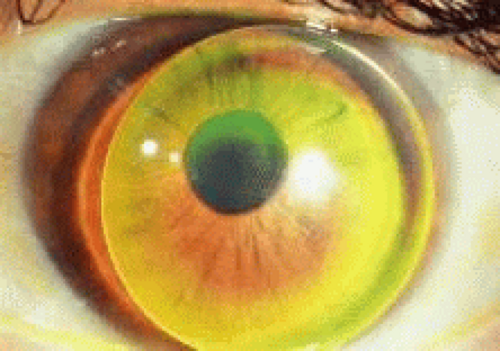 Fig. 5. Advanced keratoconus fit with Nicone RGP lens with resultant 20/25 vision. |
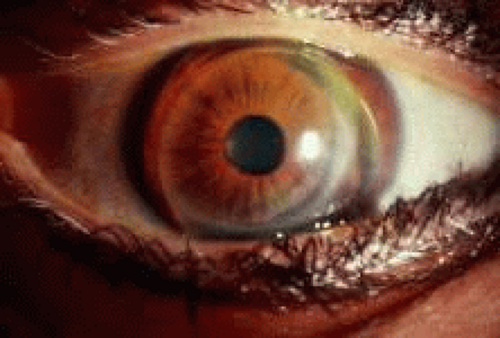 Fig. 6. Fellow eye of patient in Figure 5—after penetrating keratoplasty. Acuity without correction: 20/200 Fit with keratoconus lens design improving visual acuity to 20/30. |
There are numerous keratoconus lens designs available in the market. The primary goal of each design is to allow adequate fitting over the diseased cornea with minimal or no direct mechanical trauma to the normal tissue. This is typically accomplished with designs that incorporate several different posterior curvatures in which the central curvature is steeper and the peripheral curves are flatter. Some lenses are bicurved, tricurved, or even multicurved. Aspheric lenses are often used.
Some of the lens designs available today for patients with keratoconus include:
Soper Cone—bicurved
Nicone—tricurved (Fig. 7)
Aspheric lenses (complex)
Mc Guire
Rose K
Comfort Kone
KAS Lens
Valley K
Porus K
Formacon
Piggy-back lenses
Softperm (hybrid)
Scleral (haptic) lenses
Flexlens Tricurve keratoconus lens (soft)
Flexlens Harrison keratoconus lens (soft)
Dura-T
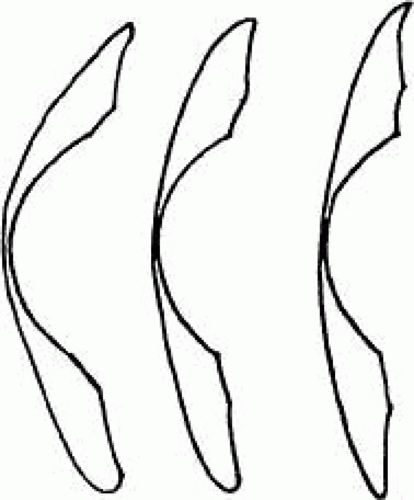 Fig. 7. Nicone lens design—for keratoconus patients. |
Although some of these lenses may be available in PMMA hard lens material, it is highly recommended that gas permeable materials be used to avoid further compromise on an already diseased cornea.
In the hands of an experienced contact lens fitter, most moderate and many advanced cases of keratoconus can be successfully fitted with contact lenses (Fig. 8). Today, a much lower percentage of keratoconus patients require corneal transplantation, because of the technologic advances and the many contact lens options available.
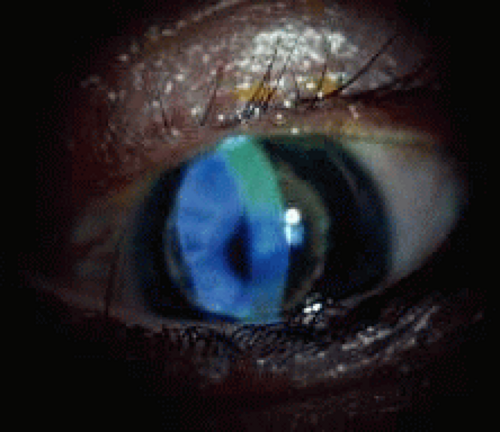 Fig. 8. Keratoconus patient successfully fit with Nicone lens. |
IRREGULAR ASTIGMATISM
Significant irregular astigmatism can result from ocular surgery, although it is most commonly seen in patients with penetrating injuries or in patients with significant corneal surface pathology. When the amount and extent of the irregular astigmatism is mild, soft contact lenses can be used successfully. When soft lenses are used, it is recommended that a thick lens be used. The thicker lenses will allow less flexure, thus creating an effective tear-lens layer.
In most cases, a rigid lens is needed due to the large amount of irregular astigmatism. Rigid lenses will usually provide patients with a better visual acuity. Whenever possible, a thin, spherical gas permeable lens is preferred. The fitting technique may vary, although care should be given to protecting the cornea from lens trauma to the areas of protrusion (Fig. 9). Although a relatively thin lens is recommended, flexure will be a problem if the lens selected is too thin. In patients who cannot tolerate rigid lenses, either piggy-back lenses or a hybrid lens may be used successfully.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


