 Osseous, Myogenic, Neurogenic, Fibrous, and Histiocytic Tumors of the Uvea
Osseous, Myogenic, Neurogenic, Fibrous, and Histiocytic Tumors of the UveaChoroidal Osteoma
General Considerations
Choroidal osteoma (choroidal osseous choristoma) is an unusual benign bony tumor that has received much attention in the literature (1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53). Its etiology and pathogenesis are unknown, but it has typical clinical and histopathologic features. It is unilateral in 79% of cases, is bilateral in 21% of cases, and is most often diagnosed in young adult women (67%) (8). More than one family member has been affected in 5% of cases (8, 9, 10). The mean age at diagnosis is 26 years, the median age is 25 years, and it has been diagnosed in young children (17,36). Most cases are not strictly congenital: We have noted the development of choroidal osteoma in previously normal choroid. Bilateral total blindness from bilateral atypical choroidal osteoma has been recognized (15). In that case, the mother eventually had a daughter who had bilateral choroidal osteoma.
Clinical Features
Choroidal osteoma typically appears as a yellow-orange placoid, juxtapapillary or macular lesion with well-defined margins that may show pseudopodia-like projections. One study of 74 eyes with choroidal osteoma disclosed that at 10 years, tumor growth was documented in about 50%, tumor decalcification in about 50%, visual loss greater than three lines in 50%, vision of 20/200 or worse in 50%, and development of choroidal neovascular membrane in 30% (figures rounded to nearest 5%) (8). Lesions presumed to be choroidal osteoma have been associated with other ocular abnormalities, including Rieger anomaly, histiocytosis X, and others, but these associations are possibly coincidental (18,29).
The differential diagnosis includes several conditions, including sclerochoroidal calcification (21), intrascleral cartilage associated with organoid nevus syndrome (52), choroidal metastasis, amelanotic choroidal nevus and melanoma, choroidal granuloma, posterior scleritis, subretinal fibrosis, and other nonpigmented fundus lesions. The first two can be highly echogenic with ultrasonography and be indistinguishable from choroidal osteoma using that technique. However, the ophthalmoscopic features are different (21,52).
Diagnostic Approaches
Fluorescein angiography shows patchy early hyperfluorescence and intense late staining of the lesion (1, 2, 3, 4, 5). Vascular tufts are sometimes seen emerging through the bone. A-scan and B-scan ultrasonography show a highly reflective echo that persists at lower sensitivity. CT reveals a choroidal plaque with bone density. MRI shows the tumor to be hyperintense to vitreous on the T1-weighted image and hypointense to vitreous on the T2-weighted image, similar to most other choroidal tumors (51). The pathogenesis of choroidal osteoma is unknown. Serum calcium, phosphorus, and alkaline phosphatase levels are generally normal.
Pathology
Histopathologically, choroidal osteoma is composed of mature bone at the level of the choroid. The overlying retinal pigment epithelium is usually intact, a finding quite different from that in osseous metaplasia or the retinal pigment epithelium in which case there is no normal RPE in the affected area (1, 2, 3).
Management
Choroidal osteoma has traditionally been managed by observation because no specific treatment was believed to be effective. If subretinal neovascularization threatens vision, laser photocoagulation can be employed to obliterate the neovascularization and prevent extensive hemorrhage (13,14). The visual prognosis is often unpredictable. However, we have observed that if the osteoma is pure orange-yellow in color, the overlying sensory retina is more normal with optical coherence tomography, and if it is subfoveal in location, the vision remains fairly good. In contrast, if the lesion has overlying black patches of RPE proliferation, suggesting spontaneous decalcification, the retina is more damaged and vision is likely to be worse.
These observations may have therapeutic implications. If it were possible to maintain intact bone beneath the fovea or to prevent decalcification from progressing to the fovea, then better vision might be maintained. Methods for achieving this may not yet be available, but it is possible that the use of a barrier laser to prevent progressive decalcification may prove to be of some benefit is preserving better vision. Photodynamic therapy has been recently shown to induce dramatic resolution of a choroidal osteoma and associated choroidal neovascular membrane (53). This method deserves further investigation (53). The associated subretinal neovascular membrane has rarely been removed surgically (20).
Selected References
1. Gass JDM, Guerry RK, Jack RL, et al. Choroidal osteoma. Arch Ophthalmol 1978;96:428-435.
2. Shields JA, Shields CL. Osseous tumors of the uvea. In: Shields JA, Shields CL, eds. Intraocular Tumors. A Text and Atlas. Philadelphia: WB Saunders; 1992:261-271.
3. Williams AT, Font RL, Van Dyk H, et al. Osseous choristoma of the choroid simulating a choroidal melanoma. Arch Ophthalmol 1978;96:1874-1877.
4. Joffe L, Shields JA, Fitzgerald JR. Osseous choristoma of the choroid. Arch Ophthalmol 1978;96:1809-1812.
5. Shields CL, Shields JA, Augsburger JJ. Choroidal osteoma. Surv Ophthalmol 1988;33:17-27.
6. Gass JD. New observations concerning choroidal osteomas. Int Ophthalmol 1979;1:71-84.
7. Aylward GW, Chang TS, Pautler SE, et al. A long-term follow-up of choroidal osteoma. Arch Ophthalmol 1998;116:1337-1341.
8. Shields CL, Sun H, Demirci H, et al. Factors predictive of tumor growth, tumor decalcification, choroidal neovascularization and visual outcome in 74 eyes with choroidal osteoma. Arch Ophthalmol 2005;123:658-666.
9. Cunha SL. Osseous choristoma of the choroid. A familial disease. Arch Ophthalmol 1984;102:1052-1054.
10. Noble KG. Bilateral choroidal osteoma in three siblings. Am J Ophthalmol 1990;109:656-660.
11. Shields JA, Shields CL, DePotter P, et al. Progressive enlargement of a choroidal osteoma. Arch Ophthalmol 1995;113:819-820.
12. Trimble SB, Schatz H, Schneider GB. Spontaneous decalcification of a choroidal osteoma. Ophthalmology 1988;95:631-644.
13. Grand MG, Burgess DB, Singerman LJ, et al. Choroidal osteoma. Treatment of associated subretinal neovascular membranes. Retina 1984;4:84-90.
14. Morrison DL, Magargal LE, Ehrlich DR, et al. Review of choroidal osteoma: successful krypton red laser photocoagulation of an associated subretinal neovascular membrane involving the fovea. Ophthalmic Surg 1987;18: 299-303.
15. Shields JA, Shields CL, Ellis J, et al. Bilateral choroidal osteoma associated with bilateral total blindness. Retina 1996;16:445-447.
16. Warrasak S, Suvaranamani C, Euswas A, et al. Choroidal osteoma in Oriental patients. J Med Assoc Thai 2003;86:562-572.
17. Fava GE, Brown GC, Shields JA, et al. Choroidal osteoma in a 6-year-old child. J Pediatr Ophthalmol Strabismus 1980;17:203-205.
18. Erkilic K, Ozkiris A, Evereklioglu C, et al. Rieger anomaly with bilateral choroidal osteoma: coincidence or association? Eur J Ophthalmol 2003;13: 496-499.
19. Wilson MW, Moshfeghi DM, Haik BG, et al. Choroidal osteoma in a patient with contralateral persistent hyperplastic primary vitreous. Retina 2002;22:358-360.
20. Foster BS, Fernandez-Suntay JP, Dryja TP, et al. Surgical removal and histopathologic findings of a subfoveal neovascular membrane associated with choroidal osteoma. Arch Ophthalmol 2003;121:273-276.
21. Shields JA, Shields CL. Sclerochoroidal calcification: the 2001 Harold Gifford Lecture. Retina 2002;22:251-261.
22. Gurelik G, Lonneville Y, Safak N, et al. A case of choroidal osteoma with subsequent laser induced decalcification. Int Ophthalmol 2001;24:41-43.
23. Fukasawa A, Iijima H. Optical coherence tomography of choroidal osteoma. Am J Ophthalmol 2002;133:419-421.
24. Battaglia Parodi M, Da Pozzo S, et al. Photodynamic therapy for choroidal neovascularization associated with choroidal osteoma. Retina 2001;21:660-661.
25. Pamer Z, Kovacs B. A case of a fast-growing bilateral choroidal osteoma. Retina 2001;21:657-659.
26. Ide T, Ohguro N, Hayashi A, et al. Optical coherence tomography patterns of choroidal osteoma. Am J Ophthalmol 2000;130:131-134.
27. Augsburger JJ, Shields JA, Rife CJ. Bilateral choroidal osteoma after nine years. Can J Ophthalmol 1979;14:281-284.
28. Kadrmas EF, Weiter JJ. Choroidal osteoma. Int Ophthalmol Clin 1997; 37:171-182.
29. Okada K, Minamoto A, Sakata H, et al. Bilateral choroidal osteomas associated with histiocytosis X. Jpn J Ophthalmol 1996;40:111-115.
30. Sharma S, Sribhargava N, Shanmugam MP. Choroidal neovascular membrane associated with choroidal osteoma (CO) treated with trans-pupillary thermo therapy. Ind J Ophthalmol 2004;52:329-330.
31. Tsuchihashi T, Murayama K, Saito T, et al. Midperipheral mottling pigmentation with familial choroidal osteoma. Retina 2005;25:63-68.
32. Coston TO, Wilkinson CP. Choroidal osteoma. Am J Ophthalmol 1978; 86:368-372.
33. Verma L, Venkatesh P, Lakshmaiah NC, et al. Osseous choristoma of the choroid. Ind J Ophthalmol 2000;48:135-137.
34. Blaise P, Duchateau E, Comhaire Y, et al. Improvement of visual acuity after photodynamic therapy for choroidal neovascularization in choroidal osteoma. Acta Ophthalmol Scand 2005;83:515-516.
35. Singh AD, Talbot JF, Rundle PA, et al. Choroidal neovascularization secondary to choroidal osteoma: successful treatment with photodynamic therapy. Eye 2005;19:482-484.
36. Mizota A, Tanabe R, Adachi-Usami E. Rapid enlargement of choroidal osteoma in a 3-year-old girl. Arch Ophthalmol 1998;116:1128-1129.
37. Lafaut BA, Mestdagh C, Kohno T, et al. Indocyanine green angiography in choroidal osteoma. Graefes Arch Clin Exp Ophthalmol 1997;235:330-337.
38. Shields CL, Shields JA, De Potter P. Patterns of indocyanine green videoangiography of choroidal tumours. Br J Ophthalmol 1995;79:237-245.
39. Yuzawa M, Kawamura A, Haruyama M, et al. Indocyanine green video-angiographic findings in choroidal osteoma. Eur J Ophthalmol 1994;4:191-198.
40. Giuffre G. Vascular modifications within a choroidal osteoma. Doc Ophthalmol 1993;83:349-356.
41. Bloom PA, Ferris JD, Laidlaw A, et al. Appearances of choroidal osteomas with diagnostic imaging. Br J Radiol 1992;65:845-848.
42. Trimble SN, Schatz H. Decalcification of a choroidal osteoma. Br J Ophthalmol 1991;75:61-63.
43. Rose SJ, Burke JF, Brockhurst RJ. Argon laser photoablation of a choroidal osteoma. Retina 1991;11:224-228.
44. Buettner H. Spontaneous involution of a choroidal osteoma. Arch Ophthalmol 1990;108:1517-1518.
45. McLeod BK. Choroidal osteoma presenting in pregnancy. Br J Ophthalmol 1988;72:612-614.
46. Hoffman ME, Sorr EM. Photocoagulation of subretinal neovascularization associated with choroidal osteoma. Arch Ophthalmol 1987;105:998-999.
47. Burke JF Jr, Brockhurst RJ. Argon laser photocoagulation of subretinal neovascular membrane associated with osteoma of the choroid. Retina 1983;3:304-307.
48. Kline LB, Skalka HW, Davidson JD, et al. Bilateral choroidal osteomas associated with fatal systemic illness. Am J Ophthalmol 1982;93:192-197.
49. Kelinske M, Weinstein GW. Bilateral choroidal osteomas. Am J Ophthalmol 1981;92:676-680.
50. Teich SA, Walsh JB. Choroidal osteoma. Ophthalmology 1981;88:696-698.
51. DePotter P, Shields JA, Shields CL, et al. Magnetic resonance imaging of choroidal osteoma. Retina 1991;11:221-223.
52. Shields JA, Shields CL, Eagle RC Jr, et al. Ocular manifestations of the organoid nevus syndrome. Ophthalmology 1997;104:549-557.
53. Shields CL, Materin MA, Mehta S, et al. Regression of extrafoveal choroidal osteoma following photodynamic therapy. Arch Ophthalmol. In press.
▪ Choroidal Osteoma: Clinical Features
Some clinical variations of choroidal osteoma are shown. All patients had ultrasonographic support of the diagnosis, and many also had computed tomography performed, which also supported the diagnosis.
1. Joffe L, Shields JA, Fitzgerald J. Osseous choristoma of the choroid. Arch Ophthalmol 1978;96:1809-1812.
2. Shields JA, Shields CL, DePotter P, et al. Progressive enlargement of a choroidal osteoma. Arch Ophthalmol 1995;113:819-820.
3. Shields CL, Sun H, Demirci H, et al. Factors predictive of tumor growth, tumor decalcification, choroidal neovascularization and visual outcome in 74 eyes with choroidal osteoma. Arch Ophthalmol 2005;123:658-666.
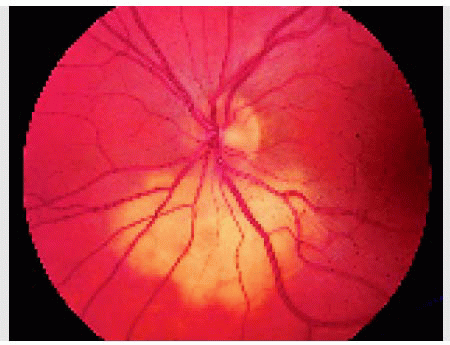
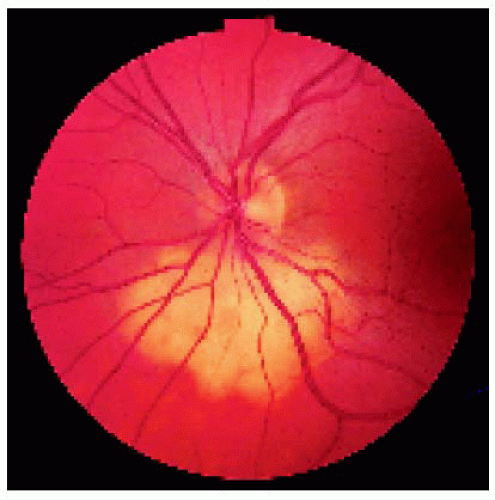 Figure 14.1. Choroidal osteoma inferior to the optic disc in a 30-year-old woman. Prior to referral, the patient was suspected to have a choroidal metastasis elsewhere, and breast biopsy was done in the hope of locating the primary neoplasm. Eventually, ultrasonography showed a bony plaque, supporting the diagnosis of choroidal osteoma. |
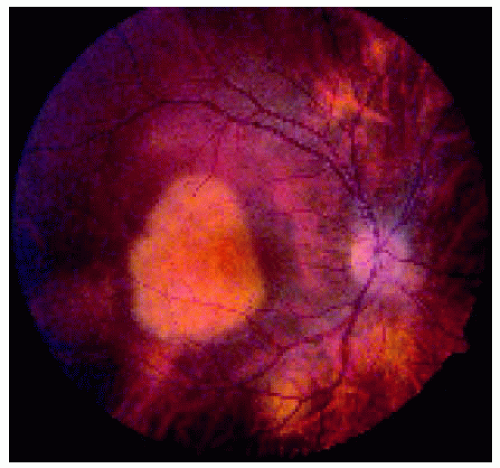 Figure 14.2. Choroidal osteoma in the macular region of the right eye in a 28-year-old man. The patient had a similar macular lesion in the left eye. |
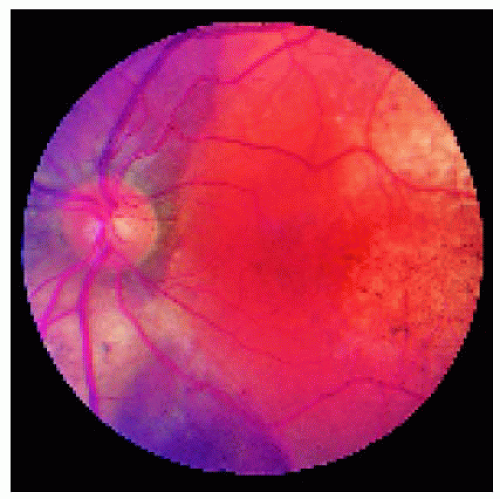 Figure 14.3. Irregular choroidal osteoma inferior to the optic disc and extending into the foveal region in a 16-year-old girl. |
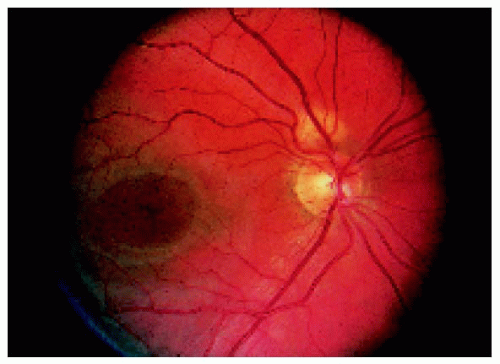 Figure 14.4. Opposite eye of the patient shown in Figure 14.3, showing small, early choroidal osteoma superior to the optic disc. The same area had been photographed 2 years earlier, and no lesion was present. |
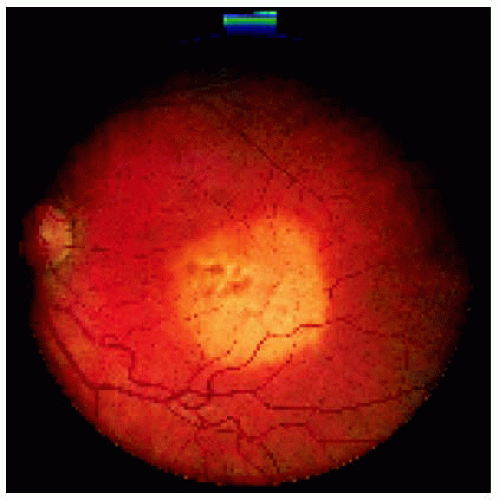 Figure 14.5. Small choroidal osteoma in the foveal region in a 20-year-old woman. The lesion was originally diagnosed as an amelanotic choroidal nevus. The lesion subsequently showed progressive growth and developed ultrasonographic evidence of calcium. |
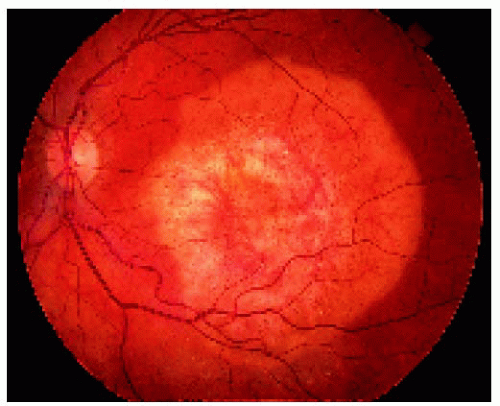 Figure 14.6. Appearance of the lesion shown in Figure 14.5 after 6 years. Note the significant enlargement. It continues to enlarge after 12 years, and the vision has slowly deteriorated. |
▪ Choroidal Osteoma: Wide-Angle Imaging
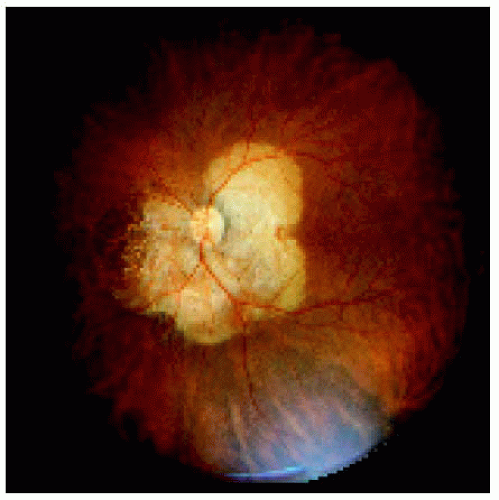 Figure 14.7. Wide-angle fundus image of circumpapillary choroidal osteoma in the left eye of a woman. Note the visibility of the choroidal vessels nasally (to the left), which represents areas of spontaneous decalcification of the tumor. |
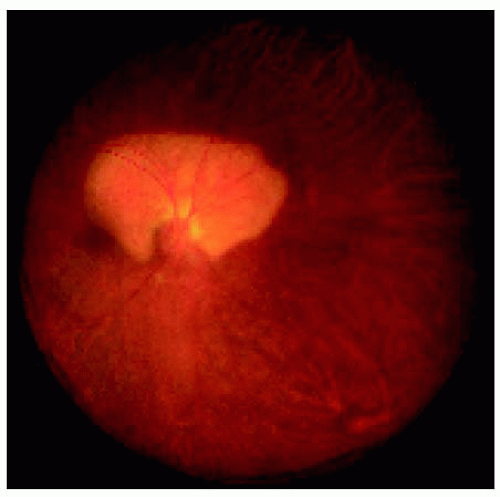 Figure 14.8. Yellow-orange choroidal osteoma extending superiorly from the optic disc in an 11-year-old girl. |
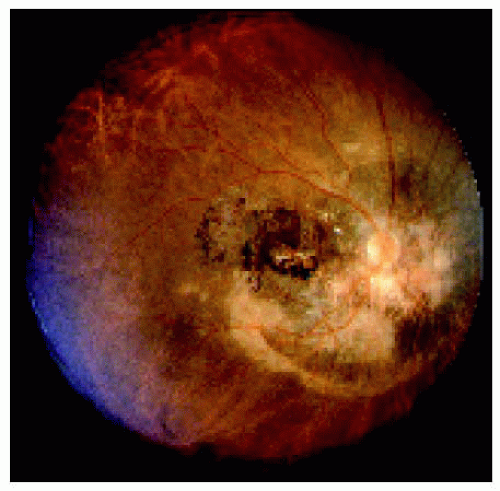 Figure 14.9. Choroidal osteoma in right eye with extensive decalcification. There is marked tumor decalcification in foveal region. This 36-year-old woman has been followed photographically for >30 years. There has been progressive decalcification in the foveal region, and the vision has remained stable at finger counting in this eye. |
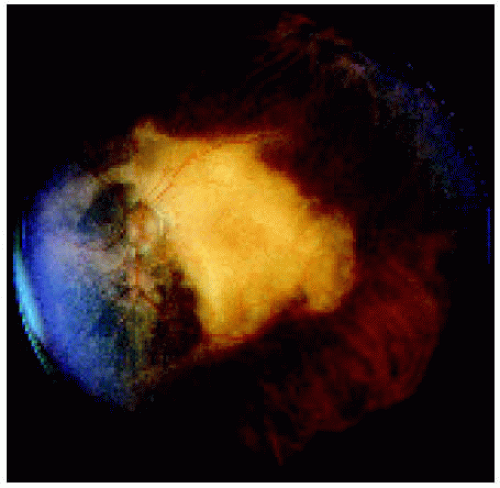 Figure 14.10. Left eye of the patient shown in Figure 14.9. Note that the nasal decalcification has not reached the fovea and the vision has remained at 20/30 for 30 years, whereas the tumor has shown slow decalcification that still spares the fovea. |
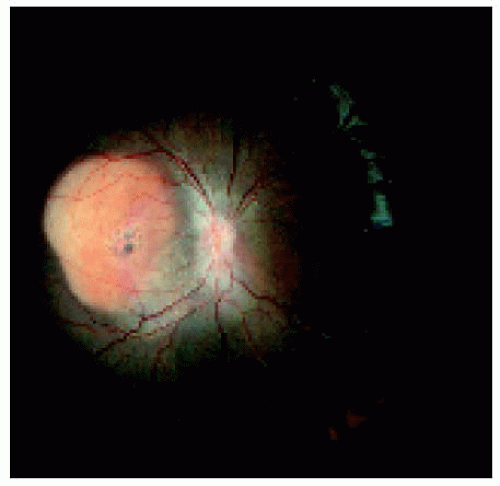 Figure 14.11. Subfoveal choroidal osteoma in a 12-year-old African American boy. |
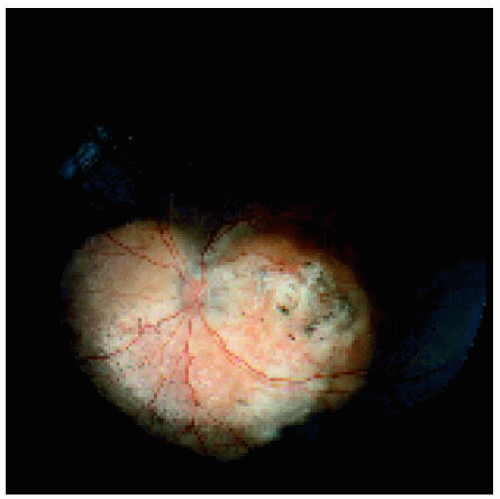 Figure 14.12. Choroidal osteoma that extends inferior to the optic disc and foveal area. Note the orange color superiorly, which represents viable osteoma, and an area of decalcification in the macular area, accounting for visual loss. |
▪ Choroidal Osteoma: Choroidal Neovascularization, Decalcification, and Familial Occurrence
1. Morrison DL, Magargal LE, Ehrlich DR, et al. Review of choroidal osteoma: successful krypton red laser photocoagulation of an associated subretinal neovascular membrane involving the fovea. Ophthalmic Surg 1987;18:299-303.
2. Shields JA, Shields CL, Ellis J, et al. Bilateral choroidal osteoma associated with bilateral total blindness. Retina 1996;16:445-447.
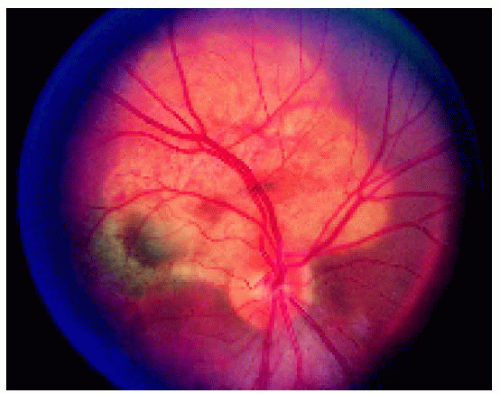 Figure 14.13. Choroidal osteoma superior to the optic disc, with the choroidal neovascular membrane extending into the foveal region. Note the gray lesion in the foveal area, characteristic of a choroidal neovascular membrane. |
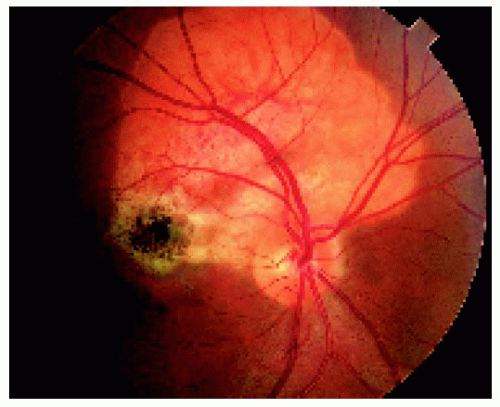 Figure 14.14. Same lesion shown in Figure 14.13 after laser photocoagulation to the juxtafoveal neovascular membrane. Note the proliferation of the retinal pigment epithelium at the site of the photocoagulation adjacent to the foveola. |
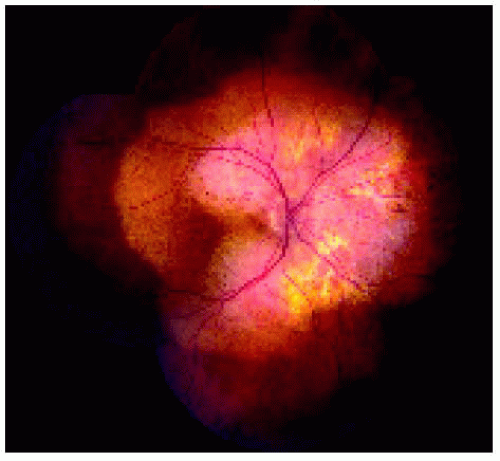 Figure 14.15. Large circumpapillary choroidal osteoma in a 30-year-old woman with extensive decalcification nasally and in the papillomacular bundle. Note the more orange color in the peripheral portion of the lesion, which represents intact bone without decalcification. |
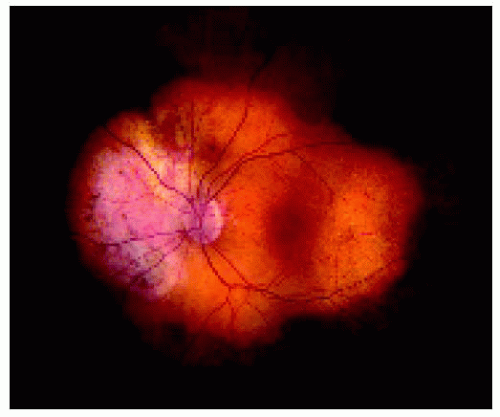 Figure 14.16. Opposite eye of the patient in Figure 14.15, showing a large choroidal osteoma with decalcification nasally. Again the calcified intact bone is more orange in color. |
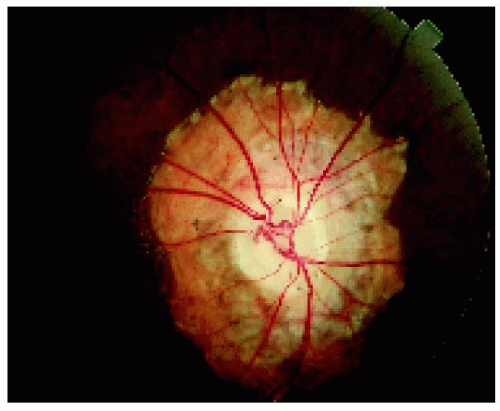 Figure 14.17. Circumpapillary choroidal osteoma in the right eye of a 20-year-old woman who has no light perception with both eyes. Note the pallor of the optic disc, indicating marked optic atrophy. |
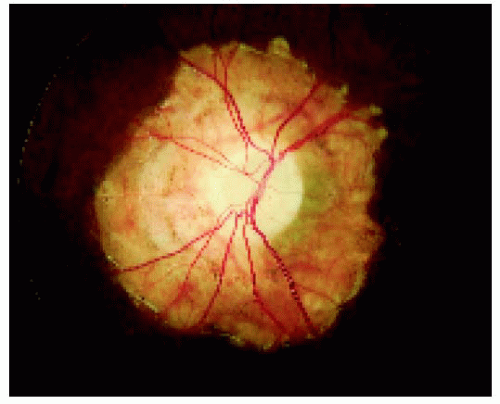 Figure 14.18. Left eye of the patient shown in Figure 14.17, demonstrating similar findings as seen in the right eye. Drusen of the optic discs were also visualized and documented with ultrasonography. This patient subsequently had a child with similar bilateral fundus lesions and blindness in both eyes. |
▪ Choroidal Osteoma: Fluorescein Angiography and Optical Coherence Tomography (OCT) Findings
Ancillary studies like fluorescein angiography and OCT have no pathognomonic features in choroidal osteoma, but they can be helpful in detecting choroidal neovascularization and effects of the adjacent, respectively.
Shields CL, Materin MA, Mehta S, et al. Regression of extrafoveal choroidal osteoma following photodynamic therapy. Arch Ophthalmol. In press.
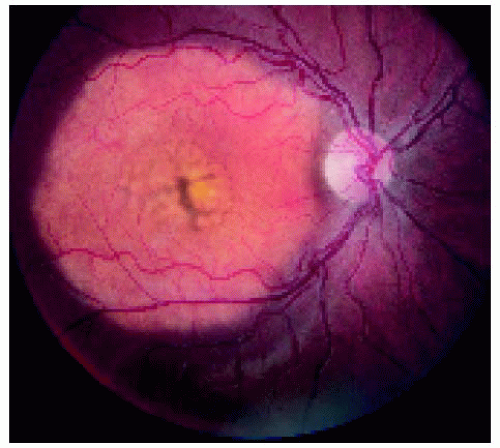 Figure 14.19. Choroidal osteoma in the macular region of the right eye. Note the central pigment disruption, which probably represents early decalcification. |
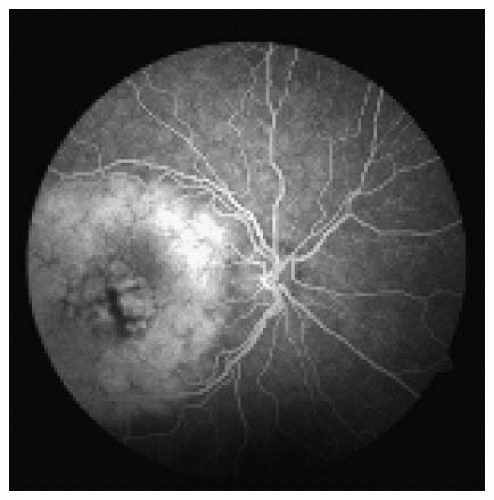 Figure 14.20. Fluorescein angiogram of the lesion shown in Figure 14.19 in the full venous phase. Note the hyperfluorescence of the lesion and hypofluorescence of the central pigment proliferation. |
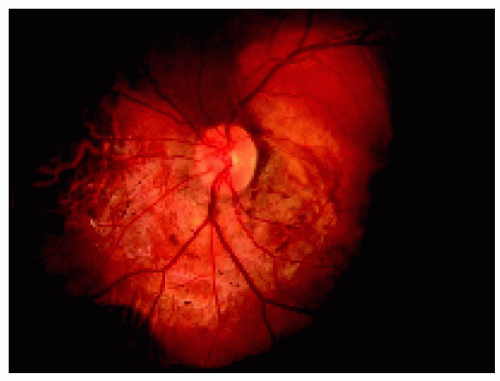 Figure 14.21. Large circumpapillary choroidal osteoma in the left eye of a 35-year-old man. Note the focal hemorrhages on the surface, possibly from a choroidal neovascular membrane. |
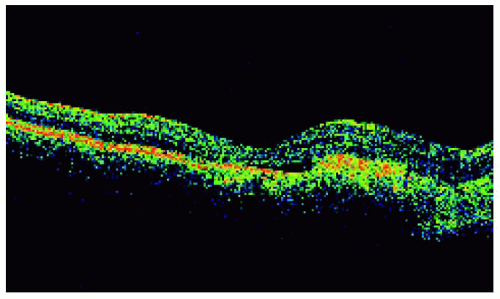 Figure 14.22. Optical coherence tomography (OCT) of the lesion shown in Figure 14.21, demonstrating thickening of the retinal pigment epithelium/photoreceptor area, compatible with the choroidal neovascular membrane seen angiographically. Note the relative shadow in the choroid, a typical OCT finding in choriodal osteoma. The main lesion is to the right in this OCT. |
 Figure 14.23. Small choroidal osteoma superior to the optic disc. It was elected to treated the patient because of choroidal neovascular membrane and persistent hemorrhage. She was treated with photodynamic therapy. |
 Figure 14.24. Appearance of the lesion in Figure 14.23, 9 months after photodynamic therapy, demonstrating resolution of hemorrhage and choroidal neovascular membrane, leaving subretinal fibrosis. Note that the osteoma appears to have disappeared and ultrasound echo became less apparent. |
▪ Choroidal Osteoma: Ultrasonography, Computed Tomography, Magnetic Resonance Imaging, and Clinicopathologic Correlation
1. Gass JDM, Guerry RK, Jack RL, et al. Choroidal osteoma. Arch Ophthalmol 1978;96:428-435.
2. Williams AT, Font RL, Van Dyk HJ, et al. Osseous choristoma of the choroid simulating a choroidal melanoma. Arch Ophthalmol 1978;96:1874-1877.
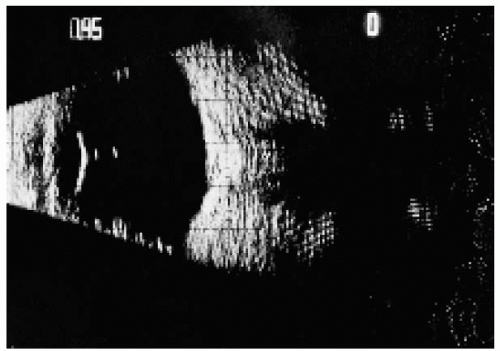 Figure 14.25. B-scan ultrasonogram of the patient in Figure 14.10, showing a placoid lesion in the posterior pole with an acoustic shadow in the orbital fat posterior to the lesion.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|