 Choroidal Nevus
Choroidal NevusChoroidal Nevus
General Considerations
Choroidal melanocytic nevus is the most common intraocular tumor (1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23), occurring in about 5% of adults. It probably is a precursor of most choroidal melanomas. Therefore, clinicians should be aware of choroidal nevus and its variations.
Clinical Features
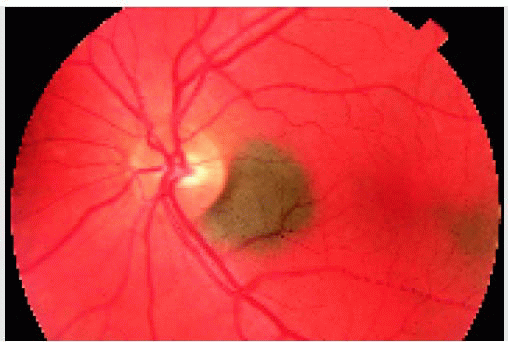
Although it may be congenital, choroidal nevus is rarely observed in young children. The precursor cells may be present at birth but do not become clinically apparent until puberty, perhaps due in part to acquisition of pigment of a previously nonpigmented lesion. It usually is first detected in adulthood and can be flat or minimally elevated and pigmented or amelanotic. It is usually between 1.5 to 5 mm in diameter and usually <2 mm in thickness. Overlying drusen develop with time. Detachment of the retinal pigment epithelium (RPE) and choroidal neovascularization (CNV) of a nevus are uncommon (12, 13, 14).
The frequency with which a choroidal nevus grows or evolves into melanoma has been addressed in several reports (9, 10, 11). Statistical risk factors for growth include tumor thickness >2 mm at initial diagnosis, overlying orange pigment, subretinal fluid, proximity to the optic disc, and presence of symptoms (1,9,11). Clinical factors predictive of possible eventual metastasis include tumor thickness >2 mm, tumor proximity to the optic disc, tumor-related symptoms, and documented enlargement (10,11).
Diagnostic Approaches
Fluorescein angiographic features vary from hypofluorescence of smaller, darker lesions to more hyperfluorescence of larger, less-pigmented lesions. Ultrasonography has limited diagnostic value but can be used for baseline thickness measurements for elevated lesions that will be followed periodically. Optical coherence tomography (OCT) can detect subtle subretinal fluid, cystoid retinal edema, and RPE alterations, but is not of value in diagnosis of the nevus itself (17,18).
Pathology
Histopathologically, a choroidal nevus is composed of a low-grade, spindle-shaped, ovoid or round melanocyte with variable amounts of cytoplasmic pigmentation. A specific variant of nevus, melanocytoma, is discussed later. Secondary changes on the adjacent structures are discussed subsequently under pathology of posterior uveal melanoma.
Management
A typical choroidal nevus requires no treatment. Baseline fundus photography and ultrasonography should be done and the patient should be examined every 6 to 12 months to detect growth of the lesion. In cases with symptomatic secondary subretinal fluid or CNV, specific methods of laser photocoagulation, transpupillary thermotherapy, or photodynamic therapy have been employed to bring about resolution of the fluid (1). Lesions that show growth or have two or more risk factors for growth or metastasis should generally be managed like a small melanoma (9, 10, 11,20), a subject covered subsequently.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


